
Abstract
Introduction
Hyperthermia is common in brain-injured patients and associated with a worse outcome. As brain rather than body temperature reduction, theoretically, is the most important in cerebral protection, there is logic in targeting cooling at the brain. Selective brain cooling can, in theory, be obtained by cooling the skull or by heat loss from the upper airways. In this preliminary safety and efficacy study, we report clinical data from brain-injured patients who because of hyperthermia were treated with intranasal cooling.
Methods
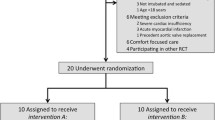
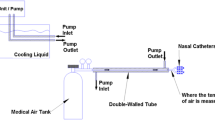
Nine intubated brain-injured patients with hyperthermia were treated using a prototype intranasal balloon system perfused with cold saline. Temperature in the cerebrum, esophagus, and bladder was monitored together with intracranial pressure.
Results
In only two of nine patients, normothermia was reached in the esophagus and in only four of nine patients it was reached in the bladder. When normothermia was reached, the time to normothermia was delayed. In the brain, normothermia was reached in two of five patients after approximately 72 h. Median temperature curves from the first 72 h of cooling showed that normothermia was not reached in any of the three compartments. The temperature in the brain and bladder were on average 0.6 and 0.5 °C higher than in the esophagus. ICP increased with increasing brain temperature. We found no signs of clinical important injury to the nasal mucosa from the cold saline or pressure in the balloons.
Conclusion
In brain-injured patients with hyperthermia, cooling with a prototype intranasal balloon system was clinically inadequate as the effect was delayed and not brain selective.






Similar content being viewed by others

References
Albrecht RF, Wass CT, Lanier WL. Occurrence of potentially detrimental temperature alterations in hospitalized patients at risk for brain injury. Mayo Clin Proc. 1998;73:629–35.
Kilpatrick MM, Lowry DW, Firlik AD, Yonas H, Marion DW. Hyperthermia in the neurosurgical intensive care unit. Neurosurgery. 2000;47:850–5.
Georgilis K, Plomaritoglou A, Dafni U, Bassiakos Y, Vemmos K. Aetiology of fever in patients with acute stroke. J Intern Med. 1999;246:203–9.
Cairns CJ, Andrews PJ. Management of hyperthermia in traumatic brain injury. Curr Opin Crit Care. 2002;8:106–10.
Diringer MN, Reaven NL, Funk SE, Uman GC. Elevated body temperature independently contributes to increased length of stay in neurologic intensive care unit patients. Crit Care Med. 2004;32:1489–95.
Li J, Jiang JY. Chinese Head Trauma Data Bank: effect of hyperthermia on the outcome of acute head trauma patients. J Neurotrauma. 2012;29:96–100.
Grande PO, Reinstrup P, Romner B. Active cooling in traumatic brain-injured patients: a questionable therapy? Acta Anaesthesiol Scand. 2009;53:1233–8.
Polderman KH. Induced hypothermia and fever control for prevention and treatment of neurological injuries. Lancet. 2008;371:1955–69.
Arrich J, Holzer M, Herkner H, Mullner M. Hypothermia for neuroprotection in adults after cardiopulmonary resuscitation. Cochrane Database Syst Rev. 2009;4:CD004128.
Jacobs S, Hunt R, Tarnow-Mordi W, Inder T, Davis P. Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Rev. 2007;4:CD003311.
Badjatia N. Hyperthermia and fever control in brain injury. Crit Care Med. 2009;37:S250–7.
Harris BA, Andrews PJ, Murray GD. Enhanced upper respiratory tract airflow and head fanning reduce brain temperature in brain-injured, mechanically ventilated patients: a randomized, crossover, factorial trial. Br J Anaesth. 2007;98:93–9.
Andrews PJ, Harris B, Murray GD. Randomized controlled trial of effects of the airflow through the upper respiratory tract of intubated brain-injured patients on brain temperature and selective brain cooling. Br J Anaesth. 2005;94:330–5.
Koehn J, Kollmar R, Cimpianu CL, et al. Head and neck cooling decreases tympanic and skin temperature, but significantly increases blood pressure. Stroke. 2012;43:2142–8.
Covaciu L, Allers M, Lunderquist A, Rubertsson S. Intranasal cooling with or without intravenous cold fluids during and after cardiac arrest in pigs. Acta Anaesthesiol Scand. 2010;54:494–501.
Covaciu L, Allers M, Enblad P, Lunderquist A, Wieloch T, Rubertsson S. Intranasal selective brain cooling in pigs. Resuscitation. 2008;76:83–8.
Harris B, Andrews P. Intranasal selective brain cooling in pigs. Resuscitation. 2008;78:102–3.
Einer-Jensen N, Khorooshi MH. Cooling of the brain through oxygen flushing of the nasal cavities in intubated rats: an alternative model for treatment of brain injury. Exp Brain Res. 2000;130:244–7.
Covaciu L, Weis J, Bengtsson C, et al. Brain temperature in volunteers subjected to intranasal cooling. Intensive Care Med. 2011;37:1277–84.
Abou-Chebl A, Sung G, Barbut D, Torbey M. Local brain temperature reduction through intranasal cooling with the RhinoChill device: preliminary safety data in brain-injured patients. Stroke. 2011;42:2164–9.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–10.
Mcilvoy L. Comparison of brain temperature to core temperature: a review of the literature. J Neurosci Nurs. 2004;36(1):23–31.
Schwab S, Spranger M, Aschoff A, Steiner T, Hacke W. Brain temperature monitoring and modulation in patients with severe MCA infarction. Neurology. 1997;48:762–7.
Acknowledgments
Quickcool AB provided the cooling device and the esophagus and cerebral temperature probes. The company also afforded technical assistance and funding for a research nurse.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Springborg, J.B., Springborg, K.K. & Romner, B. First Clinical Experience with Intranasal Cooling for Hyperthermia in Brain-Injured Patients. Neurocrit Care 18, 400–405 (2013). https://doi.org/10.1007/s12028-012-9806-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-012-9806-x