
Abstract
Background
Hyperglycemia has a detrimental effect in several acute neurological critical illnesses. No consensus exists on the optimal management of hyperglycemia in spontaneous intracerebral hemorrhage (sICH). Our aim was to determine whether blood glucose (BG) would predict 30-day mortality in sICH.
Methods
All patients with a well-defined diagnosis of sICH admitted into 24 h in three primary referred centers were included in this prospective observational follow-up study. Patients had extensive monitoring of BG values and those with BG values >8.29 mmol/l (150 mg/dl) received a variable intravenous insulin dose to maintain BG concentrations during the first 72 h after sICH between 3.32 and 8.29 mmol/l (60–150 mg/dl) using pre-specified insulin dosing schedule protocol.
Results
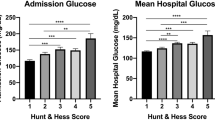
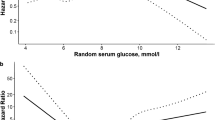
Between January 1, 2002, and December 31, 2003, 295 consecutive patients (mean ± SD age 66 ± 12 years) were prospectively included. A 1.0 mmol/l (18 mg/dl) increase in the BG concentration at admission was associated with a 33% mortality increase (OR: 1.33; 95%CI: 1.22–1.46; P < 0.0001). Adjusting for demographics, risk factors, stroke severity, and surgery there was no change in the increased risk. During the first 12 h after sICH, the insulin treatment protocol was enabling to reduce mortality (OR: 1.36, 95%CI: 1.14–1.61; P = 0.0005, per 1 IU increase) while thereafter this association was greatly attenuated and not more significant.
Conclusions
Hyperglycemia is a common condition after sICH and may worsen prognosis. Very early insulin therapy apparently does not improve prognosis. These results raise concern about routine clinical practice implementation of this intervention without any evidence from randomized trials.



Similar content being viewed by others

References
Robinson LE, van Soeren MH. Insulin resistance and hyperglycemia in critical illness: role of insulin in glycemic control. AACN Clin Issues 2004;15:45–62.
Lam AM, Winn HR, Cullen BF, Sundling N. Hyperglycemia and neurological outcome in patients with head injury. J Neurosurg 1991;75:545–51.
Michaud LJ, Rivara FP, Longstreth WT Jr, Grady MS. Elevated initial blood glucose levels and poor outcome following severe brain injuries in children. J Trauma 1991;31:1356–62.
Yang SY, Zhang S, Wang ML. Clinical significance of admission hyperglycemia and factors related to it in patients with acute severe head injury. Surg Neurol 1995;44:373–7.
Rovlias A, Kotson S. The influence of hyperglycemia on neurological outcome in patients with severe head injury. Neurosurgery 2000;46:335–43.
Martini SR, Kent TA. Hyperglycemia in acute ischemic stroke: a vascular perspective. J Cereb Blood Flow Metab 2007;27:435–51.
Demchuk AM, Morgenstern LB, Krieger DW, Linda CT, Hu W, Wein TH, et al. Serum glucose level and diabetes predict tissue plasminogen activator-related intracerebral hemorrhage in acute ischemic stroke. Stroke 1999;30:34–9.
Bruno A, Levine SR, Frankel MR, Brott TG, Lin Y, Tilley BC, et al. Admission glucose level and clinical outcomes in the NINDS rt-PA Stroke Trial. Neurology 2002;59:669–74.
Frontera JA, Fernandez A, Claassen J, Schmidt M, Schumacher HC, Wartenberg K, et al. Hyperglycemia after SAH: predictors, associated complications, and impact on outcome. Stroke 2006;37:199–203.
Capes SE, Hunt D, Maimberg K, Pathak P, Gerstein HC. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke 2001;32:2426–32.
Fogelholm R, Murros K, Rissanen A, Avikainen S. Admission blood glucose and short term survival in primary intracerebral haemorrhage: a population based study. J Neurol Neurosurg Psychiatry 2005;76:349–53.
Passero S, Ciacci G, Ulivelli M. The influence of diabetes and hyperglycemia on clinical course after intracerebral hemorrhage. Neurology 2003;61:1351–6.
Kimura K, Iguchi Y, Inoue T, Shibazaki K, Matsumoto N, Kobayashi K, et al. Hyperglycemia independently increases the risk of early death in acute spontaneous intracerebral hemorrhage. J Neurol Sci 2007;255:90–4.
Langouche L, Vanhorebeek I, Van den BG. Therapy insight: the effect of tight glycemic control in acute illness. Nat Clin Pract Endocrinol Metab 2007;3:270–8.
Adams HP Jr, del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke 2007;38:1655–711.
Gray CS, Hildreth AJ, Sandercock PA, O’Connell JE, Johnston DE, Cartlidge NE, et al. Glucose–potassium–insulin infusions in the management of post-stroke hyperglycaemia: the UK Glucose Insulin in Stroke Trial (GIST-UK). Lancet Neurol 2007;6:397–406.
Broderick J, Connolly S, Feldmann E, Hanley D, Kase C, Krieger D, et al. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke 2007;38:2001–23.
Broderick JP, Adams HP Jr, Barsan W, Feinberg W, Feldmann E, Grotta J, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: A statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 1999;30:905–15.
Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974;2:81–4.
Hemphill JC III, Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ICH score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke 2001;32:891–7.
Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2000;23 Suppl 1:S4–19.
Di Napoli M, Papa F, Bocola V. C-reactive protein in ischemic stroke: an independent prognostic factor. Stroke 2001;32:917–24.
Godoy DA, Pinero G, Di Napoli M. Predicting mortality in spontaneous intracerebral hemorrhage: can modification to original score improve the prediction? Stroke 2006;37:1038–44.
Williams LS, Rotich J, Qi R, Fineberg N, Espay A, Bruno A, et al. Effects of admission hyperglycemia on mortality and costs in acute ischemic stroke. Neurology 2002;59:67–71.
Kothari RU, Brott T, Broderick JP, Barsan WG, Sauerbeck LR, Zuccarello M, et al. The ABCs of measuring intracerebral hemorrhage volumes. Stroke 1996;27:1304–5.
Fogelholm R, Avikainen S, Murros K. Prognostic value and determinants of first-day mean arterial pressure in spontaneous supratentorial intracerebral hemorrhage. Stroke 1997;28:1396–400.
Franke CL, van Swieten JC, Algra A, van Gijn J. Prognostic factors in patients with intracerebral haematoma. J Neurol Neurosurg Psychiatry 1992;55:653–7.
Lee TH, Ryu SJ, Chen ST. The prognostic value of blood glucose in patients with acute stroke. J Formos Med Assoc 1991;90:465–70.
Melamed E. Reactive hyperglycaemia in patients with acute stroke. J Neurol Sci 1976;29:267–75.
Tuhrim S, Dambrosia JM, Price TR, Mohr JP, Wolf PA, Hier DB, et al. Intracerebral hemorrhage: external validation and extension of a model for prediction of 30-day survival. Ann Neurol 1991;29:658–63.
Woo J, Lam CW, Kay R, Wong AH, Teoh R, Nicholls MG. The influence of hyperglycemia and diabetes mellitus on immediate and 3-month morbidity and mortality after acute stroke. Arch Neurol 1990;47:1174–7.
Moulin T, Tatu L, Crepin-Leblond T, Chavot D, Berges S, Rumbach T. The Besancon Stroke Registry: an acute stroke registry of 2,500 consecutive patients. Eur Neurol 1997;38:10–20.
Flibotte JJ, Hagan N, O’Donnell J, Greenberg SM, Rosand J. Warfarin, hematoma expansion, and outcome of intracerebral hemorrhage. Neurology 2004;63:1059–64.
Gray CS, Scott JF, French JM, Alberti KG, O’Connell JE. Prevalence and prediction of unrecognised diabetes mellitus and impaired glucose tolerance following acute stroke. Age Ageing 2004;33:71–7.
Mechanick JI. Metabolic mechanisms of stress hyperglycemia. JPEN J Parenter Enteral Nutr 2006;30:157–63.
Lu A, Tang Y, Ran R, Ardizzone TL, Wagner KR, Sharp FR. Brain genomics of intracerebral hemorrhage. J Cereb Blood Flow Metab 2006;26:230–52.
Song EC, Chu K, Jeong SW, Jung KH, Kim SH, Kim M, et al. Hyperglycemia exacerbates brain edema and perihematomal cell death after intracerebral hemorrhage. Stroke 2003;34:2215–20.
Dandona P, Chaudhuri A, Ghanim H, Mohanty P. Proinflammatory effects of glucose and anti-inflammatory effect of insulin: relevance to cardiovascular disease. Am J Cardiol 2007;99:15B–26B.
Wang J, Dore S. Inflammation after intracerebral hemorrhage. J Cereb Blood Flow Metab 2007;27:894–908.
Xi G, Keep RF, Hoff JT. Mechanisms of brain injury after intracerebral haemorrhage. Lancet Neurol 2006;5:53–63.
Aljada A, Ghanim H, Mohanty P, Kapur N, Dandona P. Insulin inhibits the pro-inflammatory transcription factor early growth response gene-1 (Egr)-1 expression in mononuclear cells (MNC) and reduces plasma tissue factor (TF) and plasminogen activator inhibitor-1 (PAI-1) concentrations. J Clin Endocrinol Metab 2002;87:1419–22.
Chaudhuri A, Janicke D, Wilson MF, Tripathy D, Garg R, Bandyopadhyay A, et al. Anti-inflammatory and profibrinolytic effect of insulin in acute ST-segment-elevation myocardial infarction. Circulation 2004;109:849–54.
Hua Y, Xi G, Keep RF, Wu J, Jiang Y, Hoff JT. Plasminogen activator inhibitor-1 induction after experimental intracerebral hemorrhage. J Cereb Blood Flow Metab 2002;22:55–61.
Kagansky N, Levy S, Knobler H. The role of hyperglycemia in acute stroke. Arch Neurol 2001;58:1209–12.
Pulsinelli WA, Waldman S, Rawlinson D, Plum F. Moderate hyperglycemia augments ischemic btrain damage: a neuropathologic study in the rat. Neurology 1982;32:1239–46.
Dietrich WD, Alonso O, Busto R. Moderate hyperglycemia worsens acute blood-brain barrier injury after forebrain ischemia in rats. Stroke 1993;24:111–6.
de Court, Kleinholz M, Holm P, DeVoe G, Schmitt G, Wagner KR, et al. Hemorrhagic infarct conversion in experimental stroke. Ann Emerg Med 1992;21:120–6.
Author information
Authors and Affiliations
Corresponding authors
Appendix
Appendix
Neurointensive Care Unit protocol for glycemic management
Goal
The goal of this protocol was maintaining BG concentrations between 3.32 and 8.29 mmol/l (60–150 mg/dl).
Monitoring
BG concentrations were evaluated by routine laboratory determinations or finger-stick testing using the following schedule:
-
1.
Routine laboratory determinations were made at admission and then Q 8 h until stabilization. After this target Q 12 h.
-
2.
Bedside monitoring with trips (Medisense, Precision Plus, Abbott Laboratories, United Kingdom) Q 2 h until the patient was within the target on more than 3 consecutive readings.
-
3.
Once obtained target, monitoring Q 4 h.
-
4.
If BG concentrations were unstable or out of ranges: resuming monitoring Q 2 h.
Treatment of Hyperglycemia
-
1.
In diabetic patients, stop long-acting insulin and/or antidiabetic oral medications.
-
2.
Insulin was not given with the first two determinations. Corrections beginning with the third value.
-
3.
Schedule regimen for corrections with intravenous (i.v.) short-acting insulin (Table 1A).
-
4.
If BG concentrations >19.34 mmol/l (>350 mg/dl) in 2 consecutive measurements or diabetic patients with ketoacidosis, hyperosmolar coma, patients with mechanical ventilation or sepsis: insulin infusion protocol was started with hourly BG monitoring (Table 1A).
Hypoglycemia Management
-
1.
Give 50% dextrose in water (D50W) using the following formula: (100 − Glucose level) × 0.3 = ml D50W i.v. bolus.
-
2.
Check BG every 30 min.
-
3.
If BG < 3.32 mmol/l (<60 mg/dl), repeat previous steps and call attending physician.
Rights and permissions
About this article
Cite this article
Godoy, D.A., Piñero, G.R., Svampa, S. et al. Hyperglycemia and Short-term Outcome in Patients with Spontaneous Intracerebral Hemorrhage. Neurocrit Care 9, 217–229 (2008). https://doi.org/10.1007/s12028-008-9063-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-008-9063-1