
Abstract
Malaria remains one of the main infectious diseases in intertropical regions. The malaria parasite has a complex life cycle in its mammalian host, switching between variable forms as it traverses through different tissues and anatomic locations, either intra- or intercellularly. During its journey, the parasite encounters and interacts with the host immune system, which functions to prevent infections and limit ensuing pathologies. One important component of the host immune system is the dendritic cells (DC) network. DC form a heterogeneous group of pathogen-sensing and antigen-presenting cells that play a crucial role in the initiation of adaptive immunity. Here, we review the known and unknown interactions between the malaria parasites and the DC system, starting from the inoculation of the parasite in the skin up to its exit from the liver, also known as the pre-erythrocytic stage of the infection, and discuss how deciphering these interactions may contribute to our understanding of the Plasmodium parasite biology as well as to the induction of immune protection via vaccination.
Similar content being viewed by others

Introduction
The malaria parasite
Malaria is one of the oldest infectious diseases of mankind [1], which still exert a high burden on human health and society. This disease is induced by a unicellular protozoan parasite of the genus Plasmodium. Five different species, P. falciparum, P. vivax, P. malariae, P. ovale and P. knowlesi, are known to infect humans, inducing a wide range of pathologies.
The parasite has 2 different life-cycle phases in the insect versus mammalian host. Infection in the mammalian host begins when an infected female Anopheles mosquito takes a blood meal, thus injecting few dozen sporozoites (spz) present in the salivary glands of the insect vector into the dermis of the mammalian host [2–4] (Fig. 1). As spz are motile, they traverse through the skin, and most of them will reach a skin capillary where after entering into the vessel lumen, the spz are carried away by the blood flow, ultimately ending up in the liver or the spleen [5]. In the liver sinus, spz are arrested through specific interactions with liver proteoglycans that protrude into the capillary lumen through the space of Disse [6]. To penetrate the liver parenchyma and reach their definitive liver target cell—the hepatocyte—spz cross the sinusoidal barrier, made up of a continuous layer of endothelial cells with large fenestrae interspersed with Kupffer cells (resident liver macrophages), Ito cells and dendritic cells (DC). Once this barrier is passed, spz continue to glide through several hepatocytes before they finally settle definitively in one, forming a parasitophorous vacuole [7]. Inside this vacuole, each spz differentiates and multiplies extensively to generate an exoerythrocytic schizont, containing thousands of liver merozoites. In mouse models of infection, it has been shown that mature liver merozoites are concentrated in vesicles, called merosomes that are released into the blood stream [8] and mainly disintegrate in the pulmonary capillaries of the lungs [9]. The released merozoites infect red blood cells (RBC), ending the pre-erythrocytic stage while initiating the erythrocytic stage of the infection. The invading merozoite forms a parasitophorous vacuole inside the infected RBC where it first develops into a uninucleated ring form. The parasite then further matures and divides into a multinucleated blood-stage schizont that will subsequently rupture, releasing 4–20 merozoites, depending on the parasite species, into the bloodstream where they can now infect new RBC. During the blood stage of infection, a subpopulation of merozoites will develop into gametocytes that may be taken up by mosquitoes during a blood meal, thus completing the life-cycle phase of the parasite within the mammalian host. These parasites will subsequently undergo a new developmental phase in the insect vector to produce de novo spz.

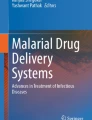
Interaction between Plasmodium and host dendritic cells during the pre-erythrocytic phase of malaria infection in mice. Sporozoites (spz) are injected into the skin by an infected Anopheles mosquito. They migrate in the tissue via extracellular gliding and by crossing skin cells. Langerhans cells (LC) lying in the outer epidermis (1) and resident dermal CD103+ and CD11b+ dendritic cells (DC) (2) can capture parasitic antigen(s) present at this initial infection site and migrate to the skin draining lymph node (dLN) where they subsequently prime specific T-cell responses. The source of parasite antigen can be the whole spz (live or dead) and/or parasite-derived vesicles (V) that are released during locomotion and covered with GPI-anchored surface proteins. Presence of salivary components (SC) left by the mosquito may modulate the local immune response and influence skin DC functions. Some spz enter the lymphatics (L) and end up in the skin dLN, providing a direct source of antigen to the resident DC there (3). Moreover, a few spz can differentiate into exoerythrocytic forms (EEF) inside cutaneous keratinocytes or endothelial cells in the dLN, thus expanding the set of parasitic antigens that may potentially be recognized by the host DC. We hypothesize that CD103+ dermal DC and CD8+ DC in the dLN would be more likely to cross-present parasitic antigens to CD8+ T cells, while CD11b+ dermal DC (migratory or resident) would preferentially induce CD4+ T cells. Inflammatory monocyte (Mo)-derived dendritic cells (MoDC) may also be recruited to the site of infection (4). Most of the spz cross the endothelial wall of a blood capillary (BC) and are carried away by the blood flow. Some are trapped in the spleen, where resident conventional DC (CD8+, CD4+, CD8−CD4−) and plasmacytoid DC (pDC) can take up parasitic antigens(s) and induce T-cell responses locally (5). Based on homology with DC subsets in non-lymphoid organs, we hypothesize that spleen CD8+ and CD4+ DC can preferentially activate CD8+ and CD4+ T-cell responses, respectively. The role of splenic pDC and CD8−CD4− cDC is unknown. When spz reach the liver, they leave the sinus lumen (SL) by squeezing in between liver sinusoidal endothelial cells (LSEC) or migrating through Kupffer cells (KC) and DC lying in the sinusoidal barrier (6). Once in the liver parenchyma, the spz traverses several hepatocytes (He) before invading one by forming a parasitophorous vacuole (PV), within which it differentiates into EEFs. After extensive multiplication, the early trophozoite (T) form differentiates into an exoerythrocytic schizont (Sc) filled with merozoites (Mz). The relative contribution of resident liver versus inflammatory recruited DC is unknown at this stage (7), but liver CD8+ DC have been shown to be capable of priming a liver-stage antigen-specific CD8+ T-cell response [100]. CD11b+ liver DC (migratory or resident) can potentially capture parasitic antigens and migrate to the liver dLN to activate CD4+ T-cell responses (8). The role of the NK1.1+ DC subset in this process is still under debate. The source of parasitic antigens for liver DC can be the infected hepatocyte or parasite-derived vesicles that are shed during migration. After maturation, parasites escape the liver in merosomes (Me) in order to avoid phagocytosis (9); these hepatocyte-derived structures enter the blood stream where they mainly disintegrate in the lung microvasculature, releasing infective Mz. This marks the transition from the pre-erythrocytic to the erythrocytic stage of infection, where Mz invade and multiply within red blood cells (RBC)
In the mammalian host, the pre-erythrocytic stage of infection is asymptomatic while it is the blood phase that is responsible for the clinical manifestations and pathologies associated with this disease. Symptoms of malaria usually develop 10–15 days after being first bitten by an infected mosquito and include high fever, muscle aches and chills [10]. Most patients successfully clear the infection upon the start of appropriate medical treatment, but in some individuals, severe pathologies such as anemia and cerebral malaria can develop, leading to death [10].
The fight against malaria has for many years consisted of two approaches. The first being mosquito control through the use of insecticides such as dichlorodiphenyltrichloroethane (DDT) or impregnated mosquito bed nets and the second being patient treatment through the use of potent antimalarial drugs such as chloroquine [11]. However, there has been clear evidence that mosquitoes have developed resistance against a wide range of insecticides [12] while the parasites are also fast gaining resistance against most available antimalarial drugs [13]. As with many diseases, a vaccine would present a potent tool to control and potentially even eliminate malaria. However, despite many years of effort, researchers have yet to develop an effective vaccine that is capable of conferring protection in more than 50% of vaccinated individuals. On the other hand, sterile immunity, defined as the absence of blood-stage parasites after a spz challenge, has been successfully induced experimentally in humans via repeated immunization with radiation-attenuated spz or with live spz under drug prophylaxis [14, 15]. These high levels of protection have never been obtained with any subunit vaccines tested so far. This could potentially be due to the use of inappropriate antigen(s) in these subunit vaccines. This is compounded by the fact that there is still a lack of validated correlates of protection in human populations, thus hindering the rational development and improvement of existing vaccines.
The absence of correlates of protection results from an incomplete understanding of host immunity against malaria. For many years, researchers have focused on the study of adaptive immunity in an attempt to define the immune mechanisms that should be either induced in order to confer protection or inhibited to prevent pathology such as cerebral malaria [16]. However, in recent years, with the emergence of new concepts and the development of novel tools, the role of innate immunity against malaria has been progressively uncovered [17]. Among them, dendritic cells have been discovered to interact closely with the malaria parasite during infection, in particular during blood infection. However, much remains to be done in order to fully delineate the role of dendritic cells in the antimalarial response. This new knowledge is likely to facilitate the development of new molecular targets for immunotherapy and vaccine development.
The dendritic cell system: classification of DC subsets
Dendritic cells (DC) are a heterogeneous population of rare hematopoietic cells found in virtually all non-lymphoid and lymphoid tissues, where they form a network of pathogen-sensing and antigen-presenting cells [18, 19]. DC are at the crossroads of innate and adaptive immunity and are therefore crucial for the development of protective and/or immunopathological responses. The main role of DC is to induce specific immunity against invading pathogens while maintaining tolerance to self-antigens [18]. Phenotypically, DC are identified by the constitutive expression of the CD11c integrin as well as major histocompatibility class II (MHCII) molecules. However, it is now established that this definition is too broad and that there are many different subsets of DC, each with their own unique phenotype, homeostasis and immune functions.
Several subsets of DC have been described in mice and humans. Anatomically, DC can be divided into those that reside in lymphoid versus non-lymphoid tissues (Fig. 2).

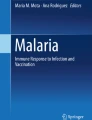
Dendritic cell subsets in lymphoid and non-lymphoid organs of mouse (black box) and their human equivalents (red box). In mouse lymphoid organs, 4 different DC subsets are found. They are pDC, CD8+, CD4+ and CD4− DC. While in murine non-lymphoid organs, 3 subsets are present—CD103+, CD11b+ DC and Langerhans cells. In human tissues, the presence of pDC, CD141+, CD1c+/CD1a+, CD14+ DC and Langerhans cells have been reported. Monocytes can also differentiate into DC during inflammation (mo-DC). It has been demonstrated that murine CD8+ and CD103+ DC are phenotypically and functionally homologous to human CD141+ DC. On the other hand, the relationship between murine CD4+/CD4−/CD11b+ DC and human CD1c+/CD14+ DC is still unclear
In mice, lymphoid tissues DC are further categorized into two groups: the plasmacytoid DC (pDC) and the conventional DC (cDC), with the latter encompassing both the CD8+ and CD8− DC populations. The CD8− DC population can be further subdivided into the CD4+ and CD4− DC subsets [20].
Non-lymphoid organs DC are found in all peripheral tissues at steady state. DC that populate the outer epidermal layer of stratified epithelia are called Langerhans cells (LCs) while DC in connective tissues are called interstitial DC [21]. These tissue-resident DC are also named migratory DC due to their ability to migrate to the draining lymph node (dLN) both at steady state and under inflammatory conditions. In analogy to the conventional DC present in lymphoid tissues, two interstitial DC subsets also coexist in the steady state but can be distinguished via their surface expression of the integrins CD103 (alphaE-beta7 integrin) and CD11b [22]. More importantly, although non-lymphoid organ CD103+ DC and lymphoid organ CD8α+ DC express different phenotypic markers, recent studies have shown that they are actually functionally homologous subsets, thus indicating that a homogenous DC lineage may exist across all lymphoid and non-lymphoid tissues [23]. In contrast, although non-lymphoid organ CD11b+ DC and lymphoid organ CD4+ DC express similar phenotypic markers, they appear to be functionally heterogeneous and may actually comprise of multiple cellular subsets, including contaminating monocytes and macrophages.
During inflammation, the composition of resident DC population changes. Depending on the type and degree of inflammation, tissue-resident DC are either absent or reduced from injured sites, due to their death or migration to the LNs, and are replaced by newly recruited blood-derived DC. In addition, in response to microbial or inflammatory stimuli, two additional DC subsets can be found in inflamed tissues: pDC and blood monocytes–derived inflammatory DC (mo-DC). Both serve to amplify the innate immune response to infection and act as antigen-presenting cells to contribute to adaptive responses [24, 25].
Investigations on human DC have largely been conducted on in vitro generated DC derived from peripheral blood monocytes or hematopoietic stem cell precursors. Very little is known about human DC, especially those present in non-lymphoid tissues. Nevertheless, phenotypic subsets of human DC have been described in several tissues including the blood, skin and lungs [26]. In blood, there are plasmacytoid DC (pDC) and at least two subsets of DC that are defined by their expression of CD1c (BDCA-1) and CD141 (BDCA-3) (Fig. 2). CD16+ cells define another subset [27], although it is often considered as a minor monocyte population. In tissues, DC that are similar to the blood DC subsets have been characterized, with the exception of Langerhans cells that are uniquely present in the epidermis ([26], and Haniffa and Ginhoux, unpublished data). However, cutaneous CD1c+ DC often are identified as CD1a+ DC, a marker not expressed by blood CD1c+ DC. It is also known that an additional subset of CD14+ DC that shares more features with monocytes or macrophages exists in tissues [28]. Finally, in line with what has been observed in murine models, it is only under inflammatory conditions that subpopulations of pDC and blood monocytes-derived DC are recruited to the peripheral tissues [29].
Comparative transcriptomics between murine and human DC subsets have allowed the identification of murine and human DC subsets that are phenotypically and functionally homologous to each other. For instance, there are phenotypic and gene expression similarities between human CD141 (BDCA-3)+ blood DC with murine LN resident CD8+ DC and non-lymphoid tissue CD103+ DC. CD141+ blood DC have also been determined to be homologues of the murine CD8+/CD103+ LN DC [30]. Through this work, a unifying framework of DC subtypes has begun to be revealed [31, 32]. Moreover, there is also preliminary evidence suggesting that both human blood and tissue CD141+ DC are homologous to the murine CD8+/CD103+ DC lineage (Ginhoux et al., unpublished data) (Fig. 2).
The dendritic cell system: immune functions of DC subsets
Several reports have suggested that the different DC subsets can be associated with distinct or potentially overlapping functions in both tolerance and immunity [33]. Each DC subset expresses overlapping but distinct profiles of extracellular and intracellular pathogens recognition receptors such as toll-like receptors, lectin receptors and phagocytic receptors. For example, the homologous CD103+ and CD8+ murine DC subsets share similar gene expression profiles, expressing a unique repertoire of immune and chemokine receptors such as DEC205 [34], TLR3 [35], CLEC9A [36], langerin [22] and XCR1 [30]. These subset specific expression profiles are even partially conserved across species as human CD141+ DC also uniquely express TLR3, CLEC9A and XCR1 [31, 37–39]. More importantly, these distinct expression profiles of immune receptors endow DC subsets with unique pathogen recognition and internalization properties. This might be of particular relevance in the study of how certain pathogens like Plasmodium interact with DC during infection since Plasmodium sequentially adopts forms that are morphologically and molecularly distinct during different stages of its life cycle and therefore could potentially be recognized by distinct DC subsets. However, the receptors that mediate Plasmodium parasite forms capture and internalization by DC remain yet unknown.
The different DC subsets also have distinct antigen-processing and presentation machineries that confer them unique immune roles [33]. For instance, murine CD8+ and CD103+ DC specialize in cross-presenting cell-associated antigens to CD8+ T cells [40, 41], while their splenic CD8−CD4+ counterparts (also known as CD11b+ DC) are more effective at presenting antigens to CD4+ T cells [42]. CD11b+ DC, whether resident or inflammatory, also play a key role at inflammatory sites by supporting the local expansion of effector and regulatory T cells [43], as well as restimulating memory CD8+ T cells [44]. Finally, monocyte-derived inflammatory DC have been demonstrated to be important in the control of Listeria monocytogenes or Leishmania infections [24].
Much less is known about the functional differences between the various DC subsets found in man. As mentioned earlier, investigations on human DC have largely been conducted on DC populations that were derived in vitro. Using such in vitro derived DC, it has been suggested that humoral and cellular immunity is regulated by different human DC subsets with distinct intrinsic properties [45]. For instance, CD14+ DC have been demonstrated to strongly promote antibody response development via the priming of CD4+ follicular helper T cells that are involved in inducing B cell isotype switching and differentiation into plasma cells. Langerhans cells have also been shown to prime and cross-prime naive CD8+ T cells and preferentially induce the differentiation of T helper 2 (Th2) cytokine-secreting CD4+ T cells. CD1c+ DC have been demonstrated to activate CD8+ T cells. In contrast to CD1c+ DC, the blood CD141+ DC subset is known to exhibit specialized cross-presentation function [31, 37–39]. In addition, we have preliminary data to indicate that the cutaneous CD141+ DC subset is more efficient at cross-presentation than all other dermal DC subsets (Haniffa and Ginhoux, unpublished data).
Pre-erythrocytic-stage Plasmodium and DC: an inevitable encounter
As Plasmodium completes its life cycle within the mammalian host, it transits through different anatomic sites, all of which present a different microenvironment and selection pressure on the parasite. To survive in these diverse microenvironments and invade different cell types, the parasite sequentially switches between different life forms that are morphologically and molecularly distinct. As a result, the antigenic repertoire expressed by the parasite also varies at different stages of its life cycle. Not only does this unique ability to switch antigenic repertoire and constantly adapt to the changing host microenvironment confer the parasite with the means to avoid detection by the host immune system, it also means that there may be varied interactions between the parasite and the host immune system at these different anatomic sites. This is especially imperative in parasite–DC interactions since different DC subsets are uniquely distributed in the host.
In this review, we have focused on discussing the potential interactions between pre-erythrocytic-stage parasites with host DC, which, in contrast to that of blood-stage parasites [46], have not yet been reviewed. Here, we have described the parasite–DC interactions that occur either during natural infection or after vaccination, focusing on the DC subsets involved. In particular, we have covered the following important questions: What is the source of parasite antigen for DC and where does antigen uptake occur? Where do activated DC relocate to prime the adaptive immune response? How does the parasite modulate DC function?
Pre-erythrocytic-stage parasite: dendritic cell interactions during infection
The sporozoite and DC in the skin
When an infected mosquito bites the host, the skin is the site where the host immune system first encounters the parasite [3, 4]. Elegant real-time imaging studies in mice have shown that spz glide in this tissue [2, 47] and traverse local host cells [48]. Within an hour, 50% of the inoculated spz would have already left the dermis and entered the blood circulation after crossing the endothelial walls of blood vessels that lie within the skin [2]. However, some spz remain in the dermis, ultimately dying locally after their motility has been exhausted [49]. It has also been observed in some rodent Plasmodium species that spz may infect cutaneous cells such as keratinocytes, hair follicle–associated cells, and initiate a development into exoerythrocytic forms (EEF) [50]. Lastly, ~20% of the spz enter lymphatic vessels and end up in the proximal draining lymph node (dLN) where they are trapped [2, 49, 51]. It has previously been reported by Amino et al. [48] that a rapid recruitment (within 25 min post-infection) of myelomonocytic cells composed of macrophages, granulocytes and DC occurs in the dermis after an infectious bite. In that study, DC were simply characterized as CD11c+ cells, and the exact nature of the DC subsets involved in this process, be it interstitial CD103+ and CD11b+ DC subsets, Langerhans cells or inflammatory monocyte-derived DC, remains unknown.
It has been postulated that the sporozoites’ capacity to traverse host cells by breaching cellular membranes and migrating in and out of the cells helps the parasite in avoiding detection and destruction by dermal phagocytic cells like neutrophils, macrophages and DC, thus assuring its way out of the bite site [48]. This parasitic escape strategy likely limits the capacity of DC to phagocytose live spz and migrate to the draining lymph nodes for the presentation of spz antigens to naïve T cells. However, DC can still acquire parasitic antigens by phagocytozing dying or dead parasites. In addition, spz within the skin release a trail of vesicles covered with parasitic antigens during the gliding and traversal process such as the circumsporozoite (CS) protein, thrombospondin-related protein (TRAP) and cell-traversal protein for ookinetes and sporozoites (CelTOs) [52–54] and secrete proteins like phospholipase [55], MAEBL [56] and perforin-like protein 1 (PLP1) [57] that aid in parasite migration through the cells. These parasitic proteins can all potentially be scavenged by skin DC. Previous reports of existent immune responses against CSP and TRAP during natural infection further provide evidence that these parasitic antigens are captured and presented [58, 59]. However, it is still not known whether skin DC loaded with spz or other parasite-derived antigens can migrate to the draining lymph nodes to prime T cells.
Sporozoites injected in the skin also enter the lymphatics, leading to significant enlargement of the draining lymph nodes [49]. In the lymph nodes, the spz have been shown to be closely associated with CD11c+ cells [2]. These are likely to be either resident or migratory DC, and this close parasite-DC association can lead to phagocytosis of the whole spz or of parasitic debris by the DC. Some spz can also invade endothelial cells in the dLNs and partially develop inside a parasitophorous vacuole into schizonts [2]. In this way, spz and other exoerythrocytic form (EEF) parasites can locally provide a direct source of antigen to DC present in the skin dLNs.
It is interesting to note that in a mouse model of infection where radiation-attenuated spz are inoculated into the murine skin by mosquitoes, the skin draining lymph node has been shown to be the first and main site of induction of a sporozoite-specific T-cell response [60]. In that study, it was shown that priming of the parasite T-cell response depends on cross-presentation of parasite antigens by immature DC [60]. Since resident CD8+ DC and migratory CD103+ DC excel in cross-presentation as aforementioned, we hypothesize that these subsets may be involved (Fig. 2). Further studies are needed to identify the DC subsets that interact with the parasite at this stage and to define the relative importance of resident versus inflammatory DC in the induction of a specific T-cell response.
While there is ample evidence that spz or other EEF interact with DC in the skin, it is not yet known whether the parasites are able to fully activate DC. To date, no molecules derived from these parasitic stages are known to interact with DC. However, it is possible that CSP and TRAP, proteins that cover the sporozoite surface [58, 61] and are continuously released when the parasite glides and traverses through cells, may act as pathogen-associated molecular patterns (PAMPs) to activate DC. These two proteins are glycosylphosphatidylinositol (GPI)-anchored, and it has been shown that Plasmodium-derived GPI could trigger TLR1- and TLR2-dependent maturation signals in DC [62, 63]. However, we do not exclude the possibility that the parasite may have evolved strategies to avoid recognition by DC and that they may not express any PAMPs at that stage. Determining whether these PAMPs exist and whether they are able to induce DC maturation is definitely one of the challenges in understanding sporozoite immunobiology.
In addition, when an infected mosquito takes a blood meal, the parasite is co-injected into the skin with mosquito saliva that contains biologically active molecules with antihemostatic and immunomodulatory properties [64]. It has also been shown that non-infectious Anopheles mosquito bites induce rapid mast-cell degranulation and histamine-dependent vasopermeabilization in the murine skin bite site, with recruitment of various leukocytes including CD11c+ cells to the draining lymph node [65]. However, it is not clear whether the immunological response induced by mosquito saliva affects parasite infectivity and DC functions. Conflicting results have been reported in mouse models, probably due to the different Plasmodium species–host strain combinations used [66–68].
The sporozoite in the blood circulation and spleen
After crossing the endothelial wall of blood capillaries or venules, spz are carried away by the blood flow. However, in less than 30 min, the parasites disappear from the blood circulation [69] where they are either retained in the liver [70] or trapped in the spleen [5].
In the spleen, resident phagocytic cells may be responsible for spz recognition and elimination. Of note, dendritic cells are likely to be involved in spz antigenic capture, processing and presentation to splenic T cells. It has previously been demonstrated that a CSP-specific MHC class I–restricted response can be detected by ELISpot in the spleen of infected mice 5 days post-i.v. injection of spz [71]. In addition, by adoptively transferring purified CSP-specific CD8+ T-cell precursors, Zavala et al. demonstrated that sporozoite-primed-specific CD8+ T cells can appear as early as 24 h after i.v. injection of irradiated spz and that the priming occurs mainly in the spleen [72, 73]. The same group also demonstrated that induction of the sporozoite-specific CD8+ T-cell response in infected mice was abrogated upon conditional depletion of CD11chigh cells in CD11c-DTR transgenic mice after diphtheria toxin treatment, further providing evidence that DC are involved in T-cell priming in vivo [74]. In that study, as the diphtheria toxin was administered 10 h prior to infection, it is likely that all organ-resident conventional DC but not pDC in both lymphoid and non-lymphoid tissues at steady state conditions were depleted [75]. More recently, it has also been demonstrated that endosomes in DC are involved in cross-presentation of the CSP in vivo [76]. It is important to note that many of these rodent studies on sporozoite biology and immunity against the pre-erythrocytic-stage parasite have been conducted using an intravenous route of infection. Compared with an intradermal route of infection that more closely mimics what happens in nature, the intravenous route effectively bypasses the skin phase and introduces a bias toward the spleen and liver.
The ability of DC to cross-present sporozoite antigens to T cells has also been suggested in in vitro studies. When bone marrow-derived DC were incubated in vitro with spz and subsequently adoptively transferred, these antigen-loaded DC were able to induce a CSP-specific CD8+ T-cell response in recipient mice [71]. However, it is not clear whether these antigen-loaded DC presented the parasite antigens directly to naïve T cells or whether they themselves were cross-presented to T cells by the endogenous DC present in the recipient mice.
In future studies, it will be interesting to determine whether DC indeed cross-present spz antigens to naïve CD8+ T cells or mediate the recruitment of inflammatory DC from the blood to the spleen for antigen presentation either in vitro or in vivo using more physiologically relevant routes of infection.
The sporozoite in the liver
Spz entering the liver are still motile and glide through several hepatocytes before invading and settling in one where they further develop inside a parasitophorous vacuole [7, 77]. Apart from hepatocytes, it has also been proposed that spz can traverse Kupffer cells without being phagocytozed and destroyed [48, 70, 78–81]. Furthermore, it may be possible that spz can squeeze through endothelial fenestrae or cross endothelial cells, Ito cells or even DC in order to access the liver parenchyma. These parasite traversal events are not likely to be immunologically silent. In a large proportion of the traversed cells, parasite traversal leads to cellular membrane disruption, thus inducing cell death and the release of pro-inflammatory signals [82]. For the minority of cells that manage to repair their disrupted membranes and survive, they may now be able to process and present spz antigens that were released into their cytoplasm by the parasite during its transit. Such cells may include DC. Alternatively, shed parasite antigens may also be picked up by liver DC in a manner that is similar to what has been observed in the dermis.
During its intrahepatocytic development, the spz differentiates and multiplies extensively to form an exoerythrocytic schizont containing as many as 30,000 merozoites upon full maturation. It is not known whether DC can sense the parasites during this later stage of liver development, phagocyte infected hepatocytes and therefore present liver-stage-associated parasitic antigens. We postulate that this may be unlikely since healthy growing parasites in the liver are not known to induce cellular recruitment [83]. This is also true for the hepatic dormant forms like the hypnozoites of P. vivax or P. cynomolgi (a simian parasite), which can persist in the liver for a long period of time without further infiltration or inflammation [84]. Thus, the growing liver-stage parasite may have developed mechanisms to subvert the initiation of local inflammatory responses as well as immune recognition. This is further supported by reports that at maturity, merozoites are not released directly into the blood stream but are packed into vesicles composed of host hepatocyte membrane [8, 9, 85], which in turn diffuse through the sinusoidal barrier to the circulation without being recognized by phagocytes or inducing inflammation and immune cell recruitment. However, local cellular recruitment has been observed around liver parasite remnants after the release of merosomes [8, 86]. These remnants may be taken up and processed by resident and/or infiltrating DC and may serve to induce immune responses against subsequent malaria infections [87, 88].
Protective immunity to the pre-erythrocytic-stage parasite and the role of DC
Immunization with radiation-attenuated spz (RAS) [89], genetically attenuated spz (GAS) or live spz under or no drug prophylaxis [90–94], but not dead spz [95], can confer sterile protection. In all three cases, spz are able to migrate to and develop partially or completely in the liver, but fail to develop into blood-stage parasites. This protection results from a multifaceted immune response directed against pre-erythrocytic antigens and involves both antibodies and T cells (in particular, CD8+ T cells) targeting the sporozoite and the infected hepatocyte, respectively [96, 97].
The RAS model has been mostly used to study the role of DC during malarial infection. It has been shown that RAS are more immunogenic than live spz, whereas heat-killed spz are unable to prime T-cell responses [60, 71] or induce protection [60, 95]. Thus, it appears that viability of the spz is critical in the induction of optimal immune priming and protective responses. It may be possible that only live spz or early liver-stage parasites express vita-PAMPs to potently stimulate DC. A similar phenomenon has previously been reported in bacterial systems [98].
Although liver DC, unlike those in the skin or skin dLNs, do not seem to be a major player in spz-specific T-cell priming, they may still contribute to immune responses induced against early liver-stage parasitic antigens. Indeed, it was recently shown that one of the four liver DC subsets [99], the cCD8α+ DC (CD11c+ NK1.1−) subset, increases in numbers after immunization with RAS. This specific liver DC subset was also able to induce liver-stage antigen-specific CD8+ T cells and confer protection after adoptive transfer [100]. Under steady state conditions, these cells are usually present at low numbers, thus it is not known whether they are resident liver DC or inflammatory DC that are recruited to the organ during infection (Fig. 2). In addition, the source of liver-stage antigens cross-presented by DC is still debated. It has been proposed that RAS-infected hepatocytes undergo apoptosis and that these apoptotic cells would in turn attract inflammatory DC [101]. However, in vitro studies have shown that the number of RAS-infected apoptotic cells is low and unlikely to be sufficient for efficient DC uptake and T-cell priming [101]. Instead, it has been proposed that DC might acquire parasitic antigens from the numerous live infected hepatocytes through trogocytosis [102] or phagocytosis of the whole infected hepatocytes. After antigen uptake, DC can then migrate to the liver draining lymph nodes and prime naïve T cells. Activated parasite-specific T cells will thus migrate back to the liver, recognized infected hepatocytes, and eliminate liver parasites [103–106].
Epidemiological studies have demonstrated that protective immunity against pre-erythrocytic and erythrocytic-stage parasites does develop in exposed populations [107]. However, acquired immunity against the pre-erythrocytic stage does not seem to be very strong or efficient at the population level since only a low proportion (5–20%) of continuously exposed individuals are resistant to reinfection over a 3-month period following clearance of the blood-stage infection [108–110]. This is in sharp contrast with the ability of RAS, GAS or live spz under drug prophylaxis to confer potent protection. This could be attributed to the fact that blood-stage infection does not develop in these immunization regimens and blood-stage infection with high parasitemia levels may impair cross-presentation [111] and induce tolerogenic DC that suppress T-cell activity [112–114]. Prevention of blood-stage infection may thus serve to maintain DC function and focus the immune response toward the pre-erythrocytic stage.
Conclusion
The malaria parasite during the first phases of its development in the mammalian host has developed strategies to subvert the host immune system. In particular, it appears that pre-erythrocytic-stage parasites have developed mechanisms to avoid DC recognition, thus preventing induction of a protective immune response. However, the use of whole parasite formulations is able to lead to development of sterile immunity, and DC appear central in these processes. A multidisciplinary approach is required to elucidate the mechanisms involved and provide the basis for identifying correlates of protection, so as to be able to design an efficient vaccine against malaria.
References
Bruce-Chwatt LJ. Paleogenesis and paleo-epidemiology of primate malaria. Bull World Health Organ. 1965;32:363–87.
Amino R, Thiberge S, Martin B, Celli S, Shorte S, Frischknecht F, Menard R. Quantitative imaging of Plasmodium transmission from mosquito to mammal. Nat Med. 2006;12:220–4.
Beier JC, Davis JR, Vaughan JA, Noden BH, Beier MS. Quantitation of Plasmodium falciparum sporozoites transmitted in vitro by experimentally infected Anopheles gambiae and Anopheles stephensi. Am J Trop Med Hyg. 1991;44:564–70.
Medica DL, Sinnis P. Quantitative dynamics of Plasmodium yoelii sporozoite transmission by infected anopheline mosquitoes. Infect Immun. 2005;73:4363–9.
Ferreira A, Enea V, Morimoto T, Nussenzweig V. Infectivity of Plasmodium berghei sporozoites measured with a DNA probe. Mol Biochem Parasitol. 1986;19:103–9.
Pradel G, Garapaty S, Frevert U. Proteoglycans mediate malaria sporozoite targeting to the liver. Mol Microbiol. 2002;45:637–51.
Mota MM, Pradel G, Vanderberg JP, Hafalla JC, Frevert U, Nussenzweig RS, Nussenzweig V, Rodriguez A. Migration of Plasmodium sporozoites through cells before infection. Science. 2001;291:141–4.
Sturm A, Amino R, Van De Sand C, Regen T, Retzlaff S, Rennenberg A, Krueger A, Pollok JM, Menard R, Heussler VT. Manipulation of host hepatocytes by the malaria parasite for delivery into liver sinusoids. Science. 2006;313:1287–90.
Baer K, Klotz C, Kappe SH, Schnieder T, Frevert U. Release of hepatic Plasmodium yoelii merozoites into the pulmonary microvasculature. PLoS Pathog. 2007;3:e171.
World Health Organization, Division of Control of Tropical Diseases. Severe and complicated malaria. Trans R Soc Trop Med Hyg. 1990;84:1–65.
Newton PN, White NJ. Malaria: new developments in treatment and prevention. Annu Rev Med. 1999;50:179–92.
Hunt RH, Fuseini G, Knowles S, Stiles-Ocran J, Verster R, Kaiser ML, Choi KS, Koekemoer LL, Coetzee M. Insecticide resistance in malaria vector mosquitoes at four localities in Ghana, West Africa. Parasit Vectors. 2011;4:107.
Price RN, Dorsey G, Ashley EA, Barnes KI, Baird JK, D’Alessandro U, Guerin PJ, Laufer MK, Naidoo I, Nosten F, et al. World Antimalarial Resistance Network (WARN) I: clinical efficacy of antimalarial therapy. Malar J. 2007;6:119.
Roestenberg M, McCall M, Hopman J, Wiersma J, Luty AJF, van Gemert GJ, Van de Vegte-Bolmer M, van Schaijk B, Teelen K, Arens T, et al. Protection against a malaria challenge by sporozoite inoculation. N Engl J Med. 2009;361:468–77.
Hoffman SL, Goh LM, Luke TC, Schneider I, Le TP, Doolan DL, Sacci JB Jr, De la Vega P, Dowler M, Paul C, et al. Protection of humans against malaria by immunization with radiation-attenuated Plasmodium falciparum sporozoites. J Infect Dis. 2002;185:1155–64.
Engwerda CR, Good MF. Interactions between malaria parasites and the host immune system. Curr Opin Immunol. 2005;17:381–7.
Stevenson MM, Riley EM. Innate immunity to malaria. Nat Rev Immunol. 2004;4:169–80.
Steinman RM, Hawiger D, Liu K, Bonifaz L, Bonnyay D, Mahnke K, Iyoda T, Ravetch J, Dhodapkar M, Inaba K, et al. Dendritic cell function in vivo during the steady state: a role in peripheral tolerance. Ann N Y Acad Sci. 2003;987:15–25.
Steinman RM, Banchereau J. Taking dendritic cells into medicine. Nature. 2007;449:419–26.
Shortman K, Naik SH. Steady-state and inflammatory dendritic-cell development. Nat Rev. 2007;7:19–30.
Merad M, Ginhoux F, Collin M. Origin, homeostasis and function of Langerhans cells and other langerin-expressing dendritic cells. Nat Rev Immunol. 2008;8:935–47.
Ginhoux F, Liu K, Helft J, Bogunovic M, Greter M, Hashimoto D, Price J, Yin N, Bromberg J, Lira SA, et al. The origin and development of nonlymphoid tissue CD103+ DCs. J Exp Med. 2009;206:3115–30.
Hashimoto D, Miller J, Merad M. Dendritic cell and macrophage heterogeneity in vivo. Immunity. 2011;35:323–35.
Dominguez PM, Ardavin C. Differentiation and function of mouse monocyte-derived dendritic cells in steady state and inflammation. Immunol Rev. 2010;234:90–104.
Gilliet M, Cao W, Liu YJ. Plasmacytoid dendritic cells: sensing nucleic acids in viral infection and autoimmune diseases. Nat Rev Immunol. 2008;8:594–606.
Collin M, Bigley V, Haniffa M, Hambleton S. Human dendritic cell deficiency: the missing ID? Nat Rev Immunol. 2011;11:575–83.
Schakel K, Mayer E, Federle C, Schmitz M, Riethmuller G, Rieber EP. A novel dendritic cell population in human blood: one-step immunomagnetic isolation by a specific mAb (M-DC8) and in vitro priming of cytotoxic T lymphocytes. Eur J Immunol. 1998;28:4084–93.
Haniffa M, Ginhoux F, Wang XN, Bigley V, Abel M, Dimmick I, Bullock S, Grisotto M, Booth T, Taub P, et al. Differential rates of replacement of human dermal dendritic cells and macrophages during hematopoietic stem cell transplantation. J Exp Med. 2009;206:371–85.
Nestle FO, Di Meglio P, Qin JZ, Nickoloff BJ. Skin immune sentinels in health and disease. Nat Rev Immunol. 2009;9:679–91.
Crozat K, Tamoutounour S, Manh TP, Fossum E, Luche H, Ardouin L, Guilliams M, Azukizawa H, Bogen B, Malissen B, et al. Expression of XCR1 defines mouse lymphoid-tissue resident and migratory dendritic cells of the CD8alpha+ type. J Immunol. 2011;187:4411–5.
Crozat K, Guiton R, Guilliams M, Henri S, Baranek T, Schwartz-Cornil I, Malissen B, Dalod M. Comparative genomics as a tool to reveal functional equivalences between human and mouse dendritic cell subsets. Immunol Rev. 2010;234:177–98.
Guilliams M, Henri S, Tamoutounour S, Ardouin L, Schwartz-Cornil I, Dalod M, Malissen B. From skin dendritic cells to a simplified classification of human and mouse dendritic cell subsets. Eur J Immunol. 2010;40:2089–94.
Helft J, Ginhoux F, Bogunovic M, Merad M. Origin and functional heterogeneity of non-lymphoid tissue dendritic cells in mice. Immunol Rev. 2010;234:55–75.
Contreras V, Urien C, Guiton R, Alexandre Y, Vu Manh TP, Andrieu T, Crozat K, Jouneau L, Bertho N, Epardaud M, et al. Existence of CD8alpha-like dendritic cells with a conserved functional specialization and a common molecular signature in distant mammalian species. J Immunol. 2010;185:3313–25.
Lindstedt M, Schiott A, Bengtsson A, Larsson K, Korsgren M, Greiff L, Borrebaeck CA. Genomic and functional delineation of dendritic cells and memory T cells derived from grass pollen-allergic patients and healthy individuals. Int Immunol. 2005;17:401–9.
Sancho D, Joffre OP, Keller AM, Rogers NC, Martinez D, Hernanz-Falcon P, Rosewell I, Reis e Sousa C. Identification of a dendritic cell receptor that couples sensing of necrosis to immunity. Nature. 2009;458:899–903.
Bachem A, Guttler S, Hartung E, Ebstein F, Schaefer M, Tannert A, Salama A, Movassaghi K, Opitz C, Mages HW, et al. Superior antigen cross-presentation and XCR1 expression define human CD11c+CD141+ cells as homologues of mouse CD8+ dendritic cells. J Exp Med. 2010;207:1273–81.
Jongbloed SL, Kassianos AJ, McDonald KJ, Clark GJ, Ju X, Angel CE, Chen CJ, Dunbar PR, Wadley RB, Jeet V, et al. Human CD141+ (BDCA-3)+ dendritic cells (DCs) represent a unique myeloid DC subset that cross-presents necrotic cell antigens. J Exp Med. 2010;207:1247–60.
Poulin LF, Salio M, Griessinger E, Anjos-Afonso F, Craciun L, Chen JL, Keller AM, Joffre O, Zelenay S, Nye E, et al. Characterization of human DNGR-1+ BDCA3+ leukocytes as putative equivalents of mouse CD8alpha+ dendritic cells. J Exp Med. 2010;207:1261–71.
del Rio ML, Rodriguez-Barbosa JI, Kremmer E, Forster R. CD103− and CD103+ bronchial lymph node dendritic cells are specialized in presenting and cross-presenting innocuous antigen to CD4+ and CD8+ T cells. J Immunol. 2007;178:6861–6.
den Haan JM, Lehar SM, Bevan MJ. CD8(+) but not CD8(−) dendritic cells cross-prime cytotoxic T cells in vivo. J Exp Med. 2000;192:1685–96.
Dudziak D, Kamphorst AO, Heidkamp GF, Buchholz VR, Trumpfheller C, Yamazaki S, Cheong C, Liu K, Lee HW, Park CG, et al. Differential antigen processing by dendritic cell subsets in vivo. Science. 2007;315:107–11.
McLachlan JB, Catron DM, Moon JJ, Jenkins MK. Dendritic cell antigen presentation drives simultaneous cytokine production by effector and regulatory T cells in inflamed skin. Immunity. 2009;30:277–88.
Wakim LM, Waithman J, van Rooijen N, Heath WR, Carbone FR. Dendritic cell-induced memory T cell activation in nonlymphoid tissues. Science. 2008;319:198–202.
Klechevsky E, Morita R, Liu M, Cao Y, Coquery S, Thompson-Snipes L, Briere F, Chaussabel D, Zurawski G, Palucka AK, et al. Functional specializations of human epidermal Langerhans cells and CD14+ dermal dendritic cells. Immunity. 2008;29:497–510.
Wykes MN, Good MF. What really happens to dendritic cells during malaria? Nat Rev Microbiol. 2008;6:864–70.
Vanderberg JP, Frevert U. Intravital microscopy demonstrating antibody-mediated immobilisation of Plasmodium berghei sporozoites injected into skin by mosquitoes. Int J Parasitol. 2004;34:991–6.
Amino R, Giovannini D, Thiberge S, Gueirard P, Boisson B, Dubremetz JF, Prevost MC, Ishino T, Yuda M, Menard R. Host cell traversal is important for progression of the malaria parasite through the dermis to the liver. Cell Host Microbe. 2008;3:88–96.
Yamauchi LM, Coppi A, Snounou G, Sinnis P. Plasmodium sporozoites trickle out of the injection site. Cell Microbiol. 2007;9:1215–22.
Gueirard P, Tavares J, Thiberge S, Bernex F, Ishino T, Milon G, Franke-Fayard B, Janse CJ, Menard R, Amino R. Development of the malaria parasite in the skin of the mammalian host. Proc Natl Acad Sci USA. 2010;107:18640–5.
Boyd MF, Matthews CB. An observation on the incubation period of Plasmodium falciparum. Am J Trop Med. 1939;19:69–71.
Kariu T, Ishino T, Yano K, Chinzei Y, Yuda M. CelTOS, a novel malarial protein that mediates transmission to mosquito and vertebrate hosts. Mol Microbiol. 2006;59:1369–79.
Spaccapelo R, Naitza S, Robson KJH, Crisanti A. Thrombospondin-related adhesive protein (TRAP) of Plasmodium berghei and parasite motility. Lancet. 1997;350:335.
Stewart MJ, Vanderberg JP. Malaria sporozoites leave behind trails of circumsporozoite protein during gliding. J Protozool. 1988;35:389–93.
Bhanot P, Schauer K, Coppens I, Nussenzweig V. A surface phospholipase is involved in the migration of Plasmodium sporozoites through cells. J Biol Chem. 2005;280:6752–60.
Preiser PR, Renia L, Singh N, Balu B, Jarra W, Voza T, Kaneko O, Blaire PL, Torii M, Landau I, et al. Antibodies against MAEBL ligand domains M1 and M2 inhibit sporozoite development in vitro. Infect Immun. 2004;72:3604–8.
Kaiser K, Camargo N, Coppens I, Morrisey JM, Vaidya AB, Kappe SH. A member of a conserved Plasmodium protein family with membrane-attack complex/perforin (MACPF)-like domains localizes to the micronemes of sporozoites. Mol Biochem Parasitol. 2004;133:15–26.
Robson KJ, Hall JR, Jennings MW, Harris TJ, Marsh K, Newbold CI, Tate VE, Weatherall DJ. A highly conserved amino-acid sequence in thrombospondin, properdin and in proteins from sporozoites and blood stages of a human malaria parasite. Nature. 1988;335:79–82.
Tapchaisri P, Chomcharn Y, Poonthong C, Asanavich A, Limsuwan S, Maleevan O, Tharavanij S, Harinasuta T. Anti-sporozoite antibodies induced by natural infection. Am J Trop Med Hyg. 1983;32:1203–8.
Chakravarty S, Cockburn IA, Kuk S, Overstreet MG, Sacci JB, Zavala F. CD8+ T lymphocytes protective against malaria liver stages are primed in skin-draining lymph nodes. Nat Med. 2007;13:1035–41.
Aikawa M, Yoshida N, Nussenzweig V, Nussenzweig RS. The protective antigen of malarial sporozoites Plasmodium berghei is a differentiation antigen. J Immunol. 1981;126:2494–5.
Zhu J, Krishnegowda G, Li G, Gowda DC. Proinflammatory responses by glycosylphosphatidylinositols (GPIs) of Plasmodium falciparum are mainly mediated through the recognition of TLR2/TLR1. Exp Parasitol. 2011;127:205–11.
Krishnegowda G, Hajjar AM, Zhu J, Douglass EJ, Uematsu S, Akira S, Woods AS, Gowda DC. Induction of proinflammatory responses in macrophages by the glycosylphosphatidylinositols of Plasmodium falciparum: cell signaling receptors, glycosylphosphatidylinositol (GPI) structural requirement, and regulation of GPI activity. J Biol Chem. 2005;280:8606–16.
Ribeiro JM, Nussenzveig RH, Tortorella G. Salivary vasodilators of Aedes triseriatus and Anopheles gambiae (Diptera: Culicidae). J Med Entomol. 1994;31:747–53.
Demeure CE, Brahimi K, Hacini F, Marchand F, Peronet R, Huerre M, St-Mezard P, Nicolas JF, Brey PT, Delespesse GJ, et al. Anopheles mosquito bites activate cutaneous mast cells leading to a local inflammatory response and lymph node hyperplasia. J Immunol. 2005;174:3932–40.
Donovan MJ, Messmore AS, Scrafford DA, Sacks DL, Kamhawi S, McDowell MA. Uninfected mosquito bites confer protection against infection with malaria parasites. Infect Immun. 2007;75:2523–633.
Kebaier C, Voza T, Vanderberg JP. Neither mosquito saliva nor immunity to saliva has a detectable effect on the infectivity of Plasmodium sporozoites injected into mice. Infect Immun. 2010;78:545–51.
Schneider BS, Mathieu C, Peronet R, Mecheri S. Anopheles stephensi saliva enhances progression of cerebral malaria in a murine model. Vector Borne Zoonotic Dis. 2011;11:423–32.
Nussenzweig RS, Vanderberg JP, Sanabria Y, Most H. Plasmodium berghei: accelerated clearance of sporozoites from blood as part of immune-mechanism in mice. Exp Parasitol. 1972;31:88–97.
Sinden RE, Smith JE. The role of the Kupffer cell in the infection of rodents by sporozoites of Plasmodium: uptake of sporozoites by perfused liver and the establishment of infection in vivo. Acta Trop. 1982;39:11–27.
Plebanski M, Hannan CM, Behboudi S, Flanagan KL, Apostolopoulos V, Sinden RE, Hill AV. Direct processing and presentation of antigen from malaria sporozoites by professional antigen-presenting cells in the induction of CD8 T-cell responses. Immunol Cell Biol. 2005;83:307–12.
Cockburn IA, Chakravarty S, Overstreet MG, Garcia-Sastre A, Zavala F. Memory CD8+ T cell responses expand when antigen presentation overcomes T cell self-regulation. J Immunol. 2008;180:64–71.
Sano G, Hafalla JC, Morrot A, Abe R, Lafaille JJ, Zavala F. Swift development of protective effector functions in naive CD8+ T cells against malaria liver stages. J Exp Med. 2001;194:173–80.
Jung S, Unutmaz D, Wong P, Sano G, De los SK, Sparwasser T, Wu S, Vuthoori S, Ko K, Zavala F, et al. In vivo depletion of CD11c+ dendritic cells abrogates priming of CD8+ T cells by exogenous cell-associated antigens. Immunity. 2002;17:211–20.
Bennett CL, Clausen BE. DC ablation in mice: promises, pitfalls, and challenges. Trends Immunol. 2007;28:525–31.
Cockburn IA, Tse SW, Radtke AJ, Srinivasan P, Chen YC, Sinnis P, Zavala F. Dendritic cells and hepatocytes use distinct pathways to process protective antigen from plasmodium in vivo. PLoS Pathog. 2011;7:e1001318.
Frevert U, Engelmann S, Zougbede S, Stange J, Ng B, Matuschewski K, Liebes L, Yee H. Intravital observation of Plasmodium berghei sporozoite infection of the liver. PLoS Biol. 2005;3:e192.
Baer K, Roosevelt M, Clarkson AB Jr, van Rooijen N, Schnieder T, Frevert U. Kupffer cells are obligatory for Plasmodium yoelii sporozoite infection of the liver. Cell Microbiol. 2007;9:397–412.
Frevert U, Usynin I, Baer K, Klotz C. Nomadic or sessile: can Kupffer cells function as portals for malaria sporozoites to the liver? Cell Microbiol. 2006;8:1537–46.
Ishino T, Yano K, Chinzei Y, Yuda M. Cell-passage activity is required for the malarial parasite to cross the liver sinusoidal cell layer. PLoS Biol. 2004;2:E4.
Verhave JP, Meis JFGM. The biology of tissue forms and other asexual stages in mammalian plasmodia. Experientia. 1984;40:1317–29.
Torgler R, Bongfen SE, Romero JC, Tardivel A, Thome M, Corradin G. Sporozoite-mediated hepatocyte wounding limits Plasmodium parasite development via MyD88-mediated NF-kappaB activation and inducible NO synthase expression. J Immunol. 2008;180:3990–9.
Garnham PCC, Bray RS. The influence of immunity upon the stages (including late exo-erythrocytic schizonts) of mammalian malaria parasites. Rev Bras Malariol Doencas Trop. 1956;8:151–60.
Shortt HE, Garnham PCC. The exoerythrocytic parasites of Plasmodium cynomolgi. Trans R Soc Trop Med Hyg. 1948;41:705–15.
Graewe S, Rankin KE, Lehmann C, Deschermeier C, Hecht L, Froehlke U, Stanway RR, Heussler V. Hostile Takeover by Plasmodium: reorganization of parasite and host cell membranes during liver stage egress. PLoS Pathog. 2011;7:e1002224.
Meis JFGM, Jap PH, Hollingdale MR, Verhave JP. Cellular response against exoerythrocytic forms of Plasmodium berghei in rats. Am J Trop Med Hyg. 1987;37:506–10.
Mazier D, Miltgen F, Nudelman S, Nussler AK, Renia L, Pied S, Goma J, Gentilini M. Pre-erythrocytic stages of plasmodia. Role of specific and non specific factors. Biol Cell. 1988;64:165–72.
Mazier D, Goma J, Pied S, Renia L, Nussler AK, Miltgen F, Mattei DM, Grau GE. Hepatic phase of Malaria. A crucial role as “go-between” with other stages. Bull World Health Organ. 1990;68:126–31.
Nussenzweig RS, Vanderberg JP, Most H, Orton CG. Protective immunity produced by injection of X-irradiated sporozoites of Plasmodium berghei. Nature. 1967;216:160–2.
Belnoue E, Costa FTM, Frankenberg T, Vigario AM, Voza T, Leroy N, Rodrigues MM, Landau I, Snounou G, Renia L. Protective T cell immunity against malaria liver stage after vaccination with live sporozoites under chloroquine treatment. J Immunol. 2004;172:2487–95.
Friesen J, Silvie O, Putrianti ED, Hafalla JC, Matuschewski K, Borrmann S. Natural immunization against malaria: causal prophylaxis with antibiotics. Sci Transl Med. 2010;2:40ra49.
Friesen J, Borrmann S, Matuschewski K. Induction of antimalaria immunity by pyrimethamine prophylaxis during exposure to sporozoites is curtailed by parasite resistance. Antimicrob Agents Chemother. 2011;55:2760–7.
Putrianti ED, Silvie O, Kordes M, Borrmann S, Matuschewski K. Vaccine-like immunity against malaria by repeated causal-prophylactic treatment of liver-stage Plasmodium parasites. J Infect Dis. 2009;199:899–903.
Faure P, Hulier E, Miltgen F, Renia L, Mazier D. Protective immunity against malaria: cellular changes in the liver vary according to the method of immunization. Parasite Immunol. 1995;17:469–77.
Spitalny GL, Nussenzweig RS. Effect of various routes of immunization and methods of parasite attenuation on the development of protection against sporozoite- induced rodent malaria. Proco Helminthol Soc Wash. 1972;39:506–14.
Belnoue E, Voza T, Costa FTM, Gruner AC, Mauduit M, Rosa DS, Depinay N, Kayibanda M, Vigario AM, Mazier D, et al. Vaccination with live Plasmodium yoelii blood stage parasites under chloroquine cover induces cross-stage immunity against malaria liver stage. J Immunol. 2008;181:8552–8.
Weiss WR, Sedegah M, Beaudoin RL, Miller LH, Good MF. CD8+ T cells (cytotoxic/suppressors) are required for protection in mice immunized with malaria sporozoites. Proc Natl Acad Sci USA. 1988;85:573–6.
Sander LE, Davis MJ, Boekschoten MV, Amsen D, Dascher CC, Ryffel B, Swanson JA, Muller M, Blander JM. Detection of prokaryotic mRNA signifies microbial viability and promotes immunity. Nature. 2011;474:385–9.
Crispe IN. Liver antigen-presenting cells. J Hepatol. 2011;54:357–65.
Jobe O, Donofrio G, Sun G, Liepinsh D, Schwenk R, Krzych U. Immunization with radiation-attenuated Plasmodium berghei sporozoites induces liver cCD8alpha+ DC that activate CD8+ T cells against liver-stage malaria. PLoS One. 2009;4:e5075.
Leiriao P, Mota MM, Rodriguez A. Apoptotic Plasmodium-infected hepatocytes provide antigens to liver dendritic cells. J Infect Dis. 2005;191:1576–81.
Renia L, Maranon C, Hosmalin A, Gruner AC, Silvie O, Snounou G. Do apoptotic Plasmodium-infected hepatocytes initiate protective immune responses? J Infect Dis. 2006;193:163–4.
Bongfen SE, Torgler R, Romero JF, Renia L, Corradin G. Plasmodium berghei-infected primary hepatocytes process and present the circumsporozoite protein to specific CD8+ T Cells in vitro. J Immunol. 2007;178:7054–63.
Renia L, Salone-Marussig M, Grillot DA, Pied S, Corradin G, Miltgen F, Del Giudice G, Mazier D. In vitro activity of CD4+ and CD8+ T lymphocytes from mice immunized with a malaria synthetic peptide. Proc Natl Acad Sci USA. 1991;88:7963–7.
Renia L, Grillot DA, Marussig M, Corradin G, Miltgen F, Lambert PH, Mazier D, Del Giudice G. Effector functions of circumsporozoite peptide-primed CD4+ T cell clones against Plasmodium yoelii liver stages. J Immunol. 1993;150:1471–8.
Weiss WR, Mellouk S, Houghten RA, Sedegah M, Kumar S, Good MF, Berzofsky JA, Miller LH, Hoffman SL. Cytotoxic T cells recognize a peptide from the circumsporozoite protein on malaria-infected hepatocytes. J Exp Med. 1990;171:763–73.
McGregor IA. Studies in the acquisition of immunity to Plasmodium falciparum infection in Africa. Trans R Soc Trop Med Hyg. 1964;58:80.
Owusu-Agyei S, Koram KA, Baird JK, Utz GC, Binka FN, Nkrumah FK, Fryauff DJ, Hoffman SL. Incidence of symptomatic and asymptomatic Plasmodium falciparum infection following curative therapy in adult residents of Northern Ghana. Am J Trop Med Hyg. 2001;65:197–203.
Sagara I, Sangare D, Dolo G, Guindo A, Sissoko M, Sogoba M, Niambele MB, Yalcoue D, Kaslow DC, Dicko A, et al. A high malaria reinfection rate in children and young adults living under a low entomological inoculation rate in a periurban area of Bamako, Mali. Am J Trop Med Hyg. 2002;66:310–3.
Sokhna CS, Faye FBK, Spiegel A, Dieng H, Trape JF. Rapid reappearance of Plasmodium falciparum after drug treatment among Senegalese adults exposed to moderate seasonal transmission. Am J Trop Med Hyg. 2001;65:167–70.
Wilson NS, Behrens GM, Lundie RJ, Smith CM, Waithman J, Young L, Forehan SP, Mount A, Steptoe RJ, Shortman KD, et al. Systemic activation of dendritic cells by Toll-like receptor ligands or malaria infection impairs cross-presentation and antiviral immunity. Nat Immunol. 2006;7:165–72.
Ocana-Morgner C, Mota MM, Rodriguez A. Malaria blood stage suppression of liver stage immunity by dendritic cells. J Exp Med. 2003;197:143–51.
Ocana-Morgner C, Wong KA, Lega F, Dotor J, Borras-Cuesta F, Rodriguez A. Role of TGF-beta and PGE2 in T cell responses during Plasmodium yoelii infection. Eur J Immunol. 2007;37:1562–74.
Ocana-Morgner C, Wong KA, Rodriguez A. Interactions between dendritic cells and CD4+ T cells during Plasmodium infection. Malar J. 2008;7:88.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Marjorie Mauduit, Peter See, Laurent Rénia and Florent Ginhoux have contributed equally to this work.
Rights and permissions
About this article
Cite this article
Mauduit, M., See, P., Peng, K. et al. Dendritic cells and the malaria pre-erythrocytic stage. Immunol Res 53, 115–126 (2012). https://doi.org/10.1007/s12026-012-8269-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12026-012-8269-7