
Abstract
Background
Osseous injuries are a major facet of child abuse and in most patients radiographic imaging plays a major role in diagnosis. While some injuries are typically produced as a result of excessive and inappropriate force other injuries are nonspecific in terms of their causation, but become suspicious when the history provided by the caretakers is inconsistent with the type of injury produced.
Questions/purposes
I detail the radiographic imaging of the more characteristic of the highly specific injuries, discuss the major issues that relate to some moderate- or low-specificity injuries, and describe several diseases that mimic abuse.
Methods
A review of the current and recent literature focused on the radiographic imaging of child abuse was performed by searching the National Library of Medicine database at pubmed.gov. Keywords used included: radiology, fracture, child abuse, and/or nonaccidental trauma.
Results
Injuries that are highly specific for the diagnosis of abuse include metaphyseal corner fractures, posteromedial rib fractures, and sternal, scapular, and spinous process fractures. Lesions of moderate specificity include, among other injuries, multiple fractures of various ages and epiphyseal separations. Long-bone fractures and clavicular fractures, while common, are of low specificity. In addition to the appropriate accurate diagnosis of these injuries, several diseases and syndromes may mimic abuse due to the similarity in the radiographic picture.
Conclusions
Stratification of fractures sustained in child abuse according to specificity and an understanding of the several diseases that mimic abuse are helpful in the accurate diagnosis of child abuse.
Level of Evidence
Level V, diagnostic study. See Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


Introduction
Whether mental or physical, trauma is central to all cases of child abuse. Much of that trauma results in musculoskeletal injuries, which places the orthopaedic surgeon in a primary position in the recognition and treatment of these injuries. In most patients radiographic imaging plays a major role in diagnosis. Some injuries are typically produced as a result of excessive and inappropriate force on the tender skeleton of a child. These injuries are characteristic of child abuse and include the classic metaphyseal lesion (CML) and posteromedial rib fractures. Other injuries, which are in themselves nonspecific in terms of their causation, become highly suspicious when the history provided by the caretakers is inconsistent with the type of injury produced. A toddler’s fracture of the tibia in an infant who is not yet ambulatory and therefore not “toddling” would be such an injury. Another example of such a history-injury discordance is a complex skull fracture in an infant who sustained a fall from a bed [24, 40, 49].
The most important and frequently utilized system of fracture classification as it relates to abuse was detailed by Dr. Paul Kleinman and separates various fractures into broad categories of high, moderate, and low specificity for the ultimate diagnosis of child abuse [30].
In this article, I will detail the radiographic imaging of the more characteristic highly specific injuries and discuss the major issues that relate to some moderate- or low-specificity injuries. In addition, I will discuss several mimics of abuse with which the orthopaedic surgeon should be familiar and should recognize.
Search Methods and Criteria
The database of the National Library of Medicine at http://www.pubmed.gov was used to identify articles pertaining to the radiographic diagnosis of child abuse. The initial search terms used were “fracture AND radiology AND (child abuse OR nonaccidental trauma) NOT (brain OR head)”. This search returned 300 citations. Case reports were excluded (n = 57) unless describing a specific radiographic finding (n = 1), leaving a total of 243 citations (81%). Reviews were excluded (n = 48), leaving a total of 195 citations (65%). Ninety-seven citations were then excluded as they dealt with topics not germane to a radiological musculoskeletal review such as those papers dealing with abdominal, neurologic or psychiatric or treatment issues. A total of 98 citations remained, all of which were reviewed in full by the author. From these 98 citations, 44 articles (15% of original 300) were used to form the basis of this review. Many of these citations were letters and commentaries on current major controversies centering on alternative explanations for highly suspicious fractures currently labeled as due to child abuse. Because of the importance of this discussion these citations were considered in depth and the most salient observations included here. Those excluded from the subset of 98 citations were articles that repeated prior observations, or those which on review did not present material germane or of a sufficient importance to include in this focused review. This review was augmented by scientific papers describing facets of diseases such as osteogenesis imperfecta which are important differential diagnostic possibilities as well as information from Kleinman’s authoritative text Diagnostic Imaging of Child Abuse [30] to furnish the orthopaedic surgeon with a complete and well-rounded review.
Radiographic Imaging
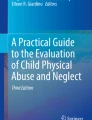
A radiographic skeletal survey for the diagnosis of child abuse includes AP views of all the bones of the appendicular skeleton, AP and lateral views of the skull, lateral views of the thoracic and lumbar spine with a separate lateral view of the cervical spine, an AP view of the chest, an AP view of the abdomen, and an AP view of the pelvis, all on separate films [3]. The entire femur should be on one film, the entire humerus on another, and so on. In some areas, a separate coned-down view centered on the joint is necessary as the joint is not necessarily viewed tangentially when the beam is centered on the midshaft of the long bone. This especially is the case at the ankle where the distal tibial physis is commonly tipped with respect to a beam centered on the midshaft of the tibia. Further coned-down views of suspicious areas may be ordered at the discretion of the interpreting radiologist. At our institution, we add bilateral oblique views of the ribs, which are invaluable for detecting frequently subtle rib fractures (Fig. 1) [23, 64]. Every effort should be made to obtain optimal images at the initial presentation. Frequently cast material, intravenous catheters, and bandages may obscure some of the detail required in a well-performed radiographic skeletal survey.

(A) A frontal chest radiograph of a 2-month-old infant shows a questionable area of rib expansion (arrowhead), not well seen against the background of lung markings. (B) In an oblique view of the same infant, focal rib expansion is more clearly seen, consistent with a healing rib fracture (arrowhead). The linear fracture line is also apparent.
“Babygram” examinations include the entire body or large parts of it imaged together on one film. This causes loss of detail at the periphery of the field of view since the beam becomes highly angulated to the anatomic part in question. Furthermore, and probably more importantly, the radiographic technique needed for different body parts depends on the density of the body part in question so that the technique used to image the thorax is very different from the technique usually used on the extremities. The extremities are therefore incorrectly exposed when included on an image of the chest and abdomen. Due to these two main factors, “babygram” examinations are not considered sufficient for diagnosis [3, 36].
CT scanning is frequently necessary to evaluate for other injuries, such as intracranial and solid organ injury, and is very efficacious for confirmation of fractures that might be subtle radiographically. This is especially so with the high detail afforded by multidetector scanners. CT images should be carefully evaluated for fractures that might not be well evident by conventional radiography. The linear lucency and the periosteal reaction and callus associated with a healing fracture may be evident. In the courtroom, three-dimensional (3D) reconstructions tend to be more highly intelligible for the layman jury member and so can be highly valuable pieces of information. Aggressive use of 3D reconstructions is recommended at the time of imaging since archiving of scan data varies between institutions and high-quality reconstructions may not be possible later on.
Bone scintigraphy is also a useful adjunct. Its main contribution is its high sensitivity, which allows diagnosis of more subtle fractures that may not be radiographically evident. Fractures at the level of the physis, however, may be obscured by the normal high uptake in the region of the growth plate.
Skeletal injuries in children have been classified into injuries that have high, moderate, and low specificity for child abuse [30]. This classification system has served well to understand and relate the multitude of skeletal injuries possible to the diagnosis of child abuse. High-specificity injuries include rib fractures, especially when those fractures are posteromedial, CMLs, and sternal, scapular, and spinous process fractures. Moderate specificity applies to the finding of multiple fractures of different ages, epiphyseal separations, vertebral body fractures and subluxations, skull fractures that ramify in multiple planes, and fractures involving the fingers. Low-specificity injuries tend to be common types of fractures that are incompatible with a given history. These include long-bone shaft, simple skull, and clavicular fractures, as well as unexplained subperiosteal new bone formation. All lesions have their highest specificity in infants (Table 1).
Posteromedial Rib Fractures
Rib fractures in children under 3 years of age have a predictive value of 95% as an indicator of abuse [6]. Posteromedial rib fractures have the highest specificity [30]. While multiple rib fractures laterally can at times be caused by nonabusive trauma, such as a severe motor vehicle accident or from metabolic causes such rickets, posteromedial rib fractures can only be caused when the chest is squeezed anteriorly and posteriorly levering the posteromedial ribs over the transverse processes (Fig. 2). This kind of pressure occurs when an adult grasps an infant around the chest causing compression. The mechanism has been reproduced by Kleinman and Schlesinger [35]. In that experiment, rabbits (euthanized as a result of a separate study) were held around the chest by the hands in a fashion similar to how an infant would be grasped with the fingers on the back near the midline and thumbs on the front. Pressure on the chest and back caused multiple posteromedial rib fractures. The same did not occur when the back was laid flat against a board and the chest compressed anteriorly [35]. This is important because it rules out posteromedial rib fractures as a result of chest compressions during cardiopulmonary resuscitation in which the child is supine and the back is supported. Due to the forces implied, the fracture always begins on the external surface of the rib rather than on its inner aspect.

(A) An AP chest radiograph of a 3-month-old infant shows a classic posteromedial rib fracture near the midline (arrow), with other healing rib fractures seen elsewhere (arrowheads). (B) An axial CT image of the same patient shows the same posteromedial fracture with irregular linear lucency (arrow). It is more clearly evident on the CT image than on the radiograph shown in (A). Other rib fractures with periosteal reaction indicating healing are also present (arrowheads and curved arrow).
By conventional radiography, an acute rib fracture can be identified by a linear lucency in the bone. The lucency varies in conspicuity depending on the angle of the fracture with respect to the beam, age of the fracture, and amount of displacement. Rib fractures are usually either nondisplaced or only minimally displaced and can be very difficult to diagnose acutely. With healing, callus develops and identifies the fracture as a small segment of fusiform widening and then tapering in the contour of the rib. Initially, the linear lucency of the fracture becomes more apparent and then fades as the fracture heals. Occasionally, only subtle linear sclerosis may be present. By CT scanning, all these phases are more easily evident, as well as the important confirmatory soft tissue changes, including pulmonary contusions, pleural effusions, and extrapleural soft tissue swelling and hemorrhage. The “hole in the rib” pattern can be explained by medullary trabecular resorption about the fracture resulting in radiographically evident radiolucency surrounding a healing fracture (Fig. 3) [33, 41].

An AP chest radiograph of a 1-month-old infant shows multiple right lateral rib fractures. Focal expansion and medullary lucency are present at the eighth rib fracture (arrow) typical of the “hole in the rib” appearance.
The ribs are curved structures and the rib necks posteromedially hide behind and next to the denser mediastinum. For these reasons, oblique views of the chest are very helpful in diagnosis of rib fractures [23]. Multidetector-row CT is also a valuable adjunct, and while it is not usually performed as a part of the ordinary skeletal survey, it is frequently obtained as a part of the larger assessment of soft tissue injuries in the thorax and abdomen of abused infants. Postmortem high-detail radiographs are effective as well (Fig. 4) [33].

A high-detail oblique view of the ribs of a 6-month-old infant shows multiple healing posteromedial rib fractures (arrowheads). The level of detail in this image is far greater than what would be present on a standard chest radiograph.
Metaphyseal Corner Fractures
Along with the posteromedial rib fracture, the CML is the most salient form of child abuse that can be visualized by imaging. Histologically, the fracture plane dissects on the metaphyseal side along the zone of provisional calcification, tearing it off, usually incompletely [32]. At the periphery, it usually extends slightly into the metaphysis proper due to the tight attachment of the periosteum at the level of the physis.
The CML can be difficult to see initially by plain film. Attention to proper technique is essential and has been discussed above. When viewed tangentially, the fracture may take the appearance of a corner fracture at the periphery where the fracture extends toward the metaphysis. The radiographic appearance is that of a small corner of metaphysis separated from the metaphyseal edge by thin linear radiolucency (Fig. 5). However, when viewed with slight cranial or caudal angulation, the true nature of the fracture is evident. The curvilinear detached zone of provisional calcification is seen as a faint curvilinear ossific density, partially detached from the metaphysis and separated from it by thin radiolucency, taking the appearance of the classic bucket handle-type fracture. The CML and the bucket handle fracture are one and the same [32].

An AP radiograph of the knee of a 4-month-old infant shows a CML at the lateral aspect of the distal femoral metaphysis (arrowhead). Note periosteal reaction (curved arrow) seen more proximally and ending at the level of the physis. Also note a healing corner fracture of the proximal tibia (arrow).
The fracture is highly specific for child abuse in infancy, ie, when a patient is nonambulatory, usually in the first year of life. Obstetric trauma during a difficult delivery is a known exception (Fig. 6) [62]. After the first year of life, the classic CML loses some of it specificity, as it can be the result of normal accidental trauma. The accepted mechanism causing this type of fracture is violent shaking of a young child, causing a whiplash-type injury at the level of the zone of provisional calcification [9, 32]. The high specificity of this type of fracture results from the fact that children who are not toddling or walking generally cannot exert this type of force by themselves to cause this type of fracture. The fracture does not result from falls, such as from a changing table, and has never been reported as a result of falls in infants in multiple studies [24, 40, 49].

An AP radiograph of the femur of a 12-day-old infant shows exuberant callus about the distal femoral bucket handle CML. This infant was a difficult footling extraction. Callus is in an advanced stage due to the young age of the patient. This amount of callus would not be present in a more recent fracture.
Epiphyseal Separations
Only designated a moderate-specificity injury, the epiphyseal separation fracture requires special mention since it is often overlooked and the images are frequently misinterpreted by those who are not comfortable with pediatric imaging.
In an epiphyseal separation, the fracture occurs through the cartilaginous physis, usually with displacement of the epiphysis. Since the epiphysis is frequently not ossified or only slightly ossified, the displacement may not be apparent to the casual observer. At the shoulder where this type of injury is frequent, there may be a subtle malalignment of the metaphysis to the glenoid. Delayed images will frequently show subperiosteal hemorrhage along the humeral shaft and then the injury will be more obvious, but at times only subtle irregularity on the metaphyseal end of the physis may be present [45].
At the hip, some cases of infantile coxa vara may be due to early epiphyseal separations at the proximal femoral physis [8, 27].
At the elbow, which is another site of epiphyseal separation, the fracture is commonly misinterpreted as a dislocation, but dislocations essentially do not occur in the infant elbow, the physis being a far more fragile item than the fibrous structures that reinforce the joint. In the majority of cases, the distal epiphysis moves medially and posteriorly with respect to the humeral metaphysis [50]. The proximal radioulnar joint remains completely concordant, but a line drawn along the radial metaphysis does not intersect with the expected location of the cartilaginous capitellum. Instead, the line lies medial to its correct location and on the lateral view it lies posterior. Confirmation of the true nature of the lesion can be obtained with ultrasound or MRI (Fig. 7) [50]. The ultrasound examination is preferable since sedation is not necessary, and in the hands of an experienced sonographer, the separation of the nonossified epiphysis from the ossified metaphysis is well seen.

(A) A lateral radiograph of the elbow of a 1-year-old child shows the capitellum (arrow) is posteriorly displaced along with the radius and ulna. The fracture plane has run through the zone of provisional calcification (arrowhead) of the distal humerus. (B) A coronal sonographic image of the distal humerus identifies the fractured and displaced zone of provisional calcification as an irregular curvilinear echogenic density (arrowheads).
Multiple Fractures and Fractures of Various Ages
The physician must bear in mind the erroneous diagnosis of abuse can be devastating for a family. Although only moderately specific for child abuse, multiple fractures and fractures in various stages of healing are an important topic, as much for the diagnosis of child abuse as for identifying what is not child abuse.
Clearly, when there are multiple fractures in an infant without a good history of trauma, a high index of suspicion is necessary. Each fracture must be evaluated closely for its type and stage of healing. The diagnosis of abuse can be made when highly specific injuries are among the injuries identified, whether soft tissue or osseous. At that point, the diagnosis of abuse becomes more secure. It is important to recognize, however, while fractures such as CMLs or posteromedial rib fractures are highly specific, low-specificity long-bone fractures are very common.
In general, the usual time course of fracture healing is as follows: 4 to 10 days for resolution of soft tissue swelling; 10 to 14 days for subperiosteal new bone formation; 14 to 21 days for immature or soft callus; loss of fracture line definition at roughly 14 to 21 days; and greater than 21 days for mature or hard callus. In infants, the process is markedly accelerated [51]. Newborns may show callus within 4 days [10], as evidenced by early callus in clavicular fractures sustained during delivery.
Location plays an important role. Intraarticular fractures do not show callus at the fracture site since there is no periosteum present [13]. The periosteum at the level of the joint capsule merges with and runs with the joint capsule rather than on the joint surface [12]. This makes sense since, at the joint level, articular cartilage is apposed to articular cartilage on the adjacent joint margin without intervening periosteum. Without the osteogenic inner layer of periosteum, callus does not occur per se. Instead, periosteal elevation and reaction can be seen more proximally in the bone away from the joint [45]. The distal humerus is a good example. A lateral condylar corner fracture will not manifest periosteal reaction at the fracture site. Instead, subperiosteal new bone formation is usually present in the diaphysis and metaphysis but ending at the capsular origin (Fig. 8).

An AP radiograph of the elbow of a 2-year-old child shows a healing supracondylar fracture (not well seen). Note how the periosteal reaction (arrowheads) ends at the capsular origin (arrow).
Variability in the extent of callus is also related to motion at the fracture site so that, in a fracture that is immediately immobilized, callus will be minimal unless the periosteum is stripped off the osseous cortical surface. Trauma in abused children tends to be repetitive without the victim coming immediately to medical attention and treatment. Callus in these cases tends to be abundant [10].
The bony mineralization should be evaluated. Callus may be markedly delayed in osteopenic patients [43] due to poor nutrition or other deficiencies of vitamin D or calcium.
Long-bone Fractures
Long-bone fractures are low-specificity lesions for child abuse. The low specificity belies their true importance as they are common in abused children. Estimated frequency varies in the medical literature. Estimates for femur fractures in children younger than 1 year due to abuse range in the medical literature from 39% to 93% [55, 66], although a recent report gives the incidence as only 11% in a Canadian population [26].
Spiral fractures have come under particularly intense scrutiny as being pathognomonic for abuse, but such is not the case. Spiral fractures and transverse fractures are equally common in abused children [57].
Dalton et al. [11] stressed the suspicious nature of femoral fractures in children younger than 3 years and emphasized the need for thorough followup investigation. In their patient population of 138 children with femoral fractures, the initial cause was abuse in only 10% of the children. After a more thorough investigation, the percentage of cases due to abuse increased to 31%. When femoral fractures sustained from a clear accidental traumatic episode or underlying medical condition were omitted, the percentage increased to 44%. Interestingly, 68 of the 138 patients (67%) were admitted to the orthopaedic service, of which 14 cases were confirmed as abuse later in the hospitalization. An additional six cases were later identified as abuse in the Child Abuse Registry [11]. Clearly, the orthopaedic surgeon should have a high suspicion of abuse when treating an infant with a femoral fracture and the surgeon should remain alert throughout the hospitalization and even thereafter.
Knowledge of the normal configuration of the bone about the metaphyses in young children is necessary for proper interpretation. The metaphysis flares smoothly as it widens to meet the physis. Immediately adjacent to and proximal to the physis, a straightened ridge of bone is present, which measures about 1 to 2 mm in length (Fig. 9). This corresponds to a subperiosteal bone collar or bone bark (ring of Lacroix) that encircles the primary spongiosa and to a variable extent the physis [58]. At its epiphyseal end is the groove of Ranvier, which is responsible for ossification of the bone bark and contributes to the funnelization mechanism that allows for widening of the metaphysis to meet the width of the epiphysis [58]. This specific morphology produces an abrupt vertical interruption to the normal slope of the metaphysis as it enlarges to conform to the epiphysis at the end of long bones. The collar can be well seen usually at the distal radial metaphyses. As the collar extends around the unossified physis, a small spur may result and cause confusion [31]. A spur should produce no periosteal reaction and no linear lucency extending into the physis beneath the zone of provisional calcification (Fig. 10). Oblique coned views may be very helpful.

An AP radiograph of the wrist of a 2-year-old boy shows a focal straightened metaphyseal collar that interrupts the smooth flaring of the metaphysis (arrows).

(A) An AP radiograph of the knee of a 3-month-old infant shows a normal metaphyseal spur with the metaphyseal collar extending along the physis (arrowhead). Note the spur is not being undercut by linear lucency and it continues smoothly onto the metaphyses. (B) An AP radiograph of the knee of a 2-month-old infant shows a CML at the distal femur. Note the excrescence medial to the physis (arrow) is not smooth and linear lucency separates it from the edge of the metaphysis. A corner fracture seen more as a bucket handle-type injury is less well seen at the proximal tibia (arrowhead).
At the medial metaphysis of the distal femur, focal cortical irregularity is common, frequently with a small excrescence at the medial aspect of the distal femoral metaphysis. A lateral view can show it has a peculiar triangular appearance [34] and sometimes fragmented appearance. The same finding can be observed at the medial proximal tibial metaphysis. It could be related to the normally bowlegged varus of toddler’s legs and asymmetric weightbearing or stress (Fig. 11).

A lateral view of the knee of a 15-month-old child shows the triangular-shaped fragmented appearance of the posterior aspect of the femur (arrow).
The medial proximal tibial and humeral metaphyses are sites of highly active bone turnover. At these “cutaway” zones, the metaphysis flares dramatically to meet the epiphysis and an active dynamic process of bone resorption and formation is responsible for this bone modeling to occur [38]. The pronounced concavity at the cutaway zone can have the appearance of a small beak where the metaphysis meets the subperiosteal collar [31] (Fig. 12).

A magnified frontal view of the proximal humerus of a 1-month-old infant shows the concave medial surface of the proximal humerus ends in a small beak. A normal notch is seen along the surface (arrow) and is a normal finding at this cutaway zone.
It is frequently most helpful to obtain followup radiographs. In most cases, the fracture line becomes more evident with periosteal reaction. Care is again mandated since, especially in cases where the extremity was quickly immobilized during treatment, the degree of callus may be minimal. Furthermore, in areas where the fracture is intraarticular, subperiosteal reaction will not be present [13].
Subperiosteal new bone formation is physiologic and normal in infants 1 to 5 months old. It is smooth and most commonly is seen along the diaphysis of the humerus, femur, and tibia. It is usually but not exclusively bilateral and is related to the rapid growth of infants.
Although physiologic subperiosteal new bone formation occurs up to 5 months old, a progression is usually observed in its appearance. Immature subperiosteal new bone is a thin hazy area of increased density separated from the cortex by a thin lucency. This type predominates in younger infants 1 to 4 months old. Subperiosteal new bone formation at 4 to 5 months is actively being incorporated into the bone and, similar to normal fracture callus, will progressively calcify and fill in, and it is this appearance that predominates later on. When subperiosteal new bone formation is seen, it should be closely examined for focality and bilaterality, as well as its appearance relative to the patient’s age. Physiologic subperiosteal new bone formation should not be greater than 2 mm in thickness [37].
Skull fractures can be difficult. Differentiation of fractures from vascular grooves and accessory sutures can be confusing. In these cases, a CT scan of the head with 3D reconstructions is invaluable, as the path of the vascular groove as a tubular lucency running obliquely through the skull or on the surface of the skull is obvious and decisive (Fig. 13). A short linear lucency running through the parietal bone and ending on a suture is frequently an accessory suture, especially if bilateral. Interdigitation across a linear lucency that ends at a suture, especially when short, is very good evidence that the lucency is indeed a normal accessory suture.

(A) A lateral radiograph of the skull of a 3-month-old infant shows a thin linear lucency (arrowhead) at the posterior parietal bone. (B) A 3D reconstruction of the skull in the same patient identifies the linear lucency as a vascular groove along the surface of the skull (arrowheads). This was confirmed using electronic crossreferencing.
Mimics of Abuse
Rickets
Rickets is a very common cause of osteopenia and may be recognized by its effect on the physis. The physis is frayed and the white line of the zone of provisional calcification is lost. In severe cases, the physis is cupped. With better nutrition, the zone of provisional calcification recovers, but physeal irregularity remains for a period of time.
Osteopenia is commonly present in premature children and other hospitalized children. Premature children can sustain multiple fractures including classic CMLs. Chronic renal or liver disease can also cause deficient bone mineral density and rickets. These patients may also sustain lesions that would ordinarily be suspicious of abuse. Injuries in these patients require a detailed clinical and social history to differentiate injuries sustained as a result of normal daily care from abuse.
Fractures in the hospital are not uncommon and difficulty arises when, soon after discharge, the patient returns to the emergency room with fractures, frequently located in the long bones. Chronically ill patients while in the hospital may not be handled as often as they are at home and accidents inevitably are common. However, chronically ill patients are also at increased risk for abuse [39]. Dating the fracture as accurately as possible is very important. A fracture showing advanced callus is not likely to have been sustained at home if the patient has been home less than 2 weeks. However, soft tissue swelling seen at the site of a fracture with no evidence of subperiosteal new bone formation is more suspicious, depending on the time since discharge. In any case, a posteromedial rib fracture should not occur as it is associated with a very specific mechanism unlikely to be duplicated as a result of daily care.
When faced with a case with multiple fractures, an effort should be made to roughly date each fracture. An assiduous search should be made for those higher-specificity fractures such as CMLs. If posteromedial rib fractures are suspected but not conclusively seen on plain film, multidetector-row CT can be very helpful and diagnostic.
Osteogenesis Imperfecta
Osteogenesis imperfecta (OI) is a rare disease writ large when the differential diagnosis of child abuse is considered. The cardinal feature of OI is increased bone fragility and, as such, must be considered when considering an infant with multiple fractures.
OI is classified according to the classification of Sillence et al. [59, 60], which for many years included only four types divided on both clinical and radiographic grounds. The Sillence classification describes a spectrum of disease rather than a strict system based on objective scientific identities. Type 1 is the most mild and patients have normal stature with little or no deformity. Type 2 is lethal in the perinatal period with beaded ribs, compressed deformed long bones, and minimal skull mineralization. Type 3 is of moderate severity with deformity generally present at birth. Type 4 is of mild to moderate severity with variable short stature and deformity. While with Types 2 and 3 the diagnosis is rarely in doubt, Types 1 and 4 engender considerable difficulties since both can be quite mild with little or no deformity present in infancy.
Types 1 to 4 are all caused by mutations in either the COL1A1 or COL1A2 gene, which encode for formation of the procollagen alpha-1 or alpha-2 chain. Two alpha-1 and one alpha-2 chains form the triple helix of collagen 1, which is the major contributor to the normal collagen matrix in bone.
Biochemical or mutation analysis is capable of identifying approximately 90% to 95% of patients with Types 1 to 4. The number is steadily increasing. However, recent descriptions of several new types of OI have changed the landscape.
Type 5 is typified by grossly hypertrophic callus about fractures and curious ossification of the interosseous membrane in the forearm [19]. It is usually moderate in severity, although some variability can be observed. It is not a mutation in collagen 1 and is not identifiable by either mutation or biochemical testing aimed at collagen 1.
Type 6 is moderate in severity and indistinguishable from Type 4 clinically [20]. It is not identifiable by mutation or collagen biochemical analysis. On microscopy of biopsied bone, it is indicated by a characteristic mineralization defect in bone.
Two new types classified as Types 7 and 8 are caused by abnormal posttranslational modification of the collagen molecule and are not identifiable by the traditional OI mutation or biochemical analysis. Both of these types manifest severe phenotypes with severe bone fragility. Metaphyseal changes and bulbous “popcorn” epiphyses, in which irregular dense calcifications are present, have been described [5]. Given the severity of these types, they should not cause confusion when considered with respect of child abuse.
The complexity and variability present in OI make differentiation from abuse very challenging and both mutation and biochemical collagen analysis are frequently performed. Since the tests are only about 90% to 95% sensitive, the results can be unsatisfying and lead to confusion when trying to differentiate abuse from OI. However, several important points may be made.
While rib fractures can occur, it is generally in the more severe types. Fractures are usually lateral and are uncommon posteromedially. Posteromedial rib fractures even in a child with OI should be taken very seriously and, except in moderate to severe cases of OI, or in the face of severe osteopenia are highly suspicious for abuse because of the typical mechanism needed to produce those fractures. In severe OI, no mechanism is needed to explain a fracture, but in mild cases the mechanism of injury reigns supreme and must be considered.
CMLs are also highly suspicious. In epiphyseal cartilage, collagen 2 predominates. At the physeal level, collagen 1 is not present [48] and is produced in the metaphyses [56]. As such, the most fragile portion of the bones of a patient afflicted with OI is not the physes but the midshaft, where fractures are more frequent. CML-type injuries are extraordinarily rare in OI and are even more rare, if they occur at all, in children younger than 1 year [4]. For a CML to occur, in the face of trauma, the physis and zone of provisional calcification need to have greater weakness when compared to the diaphyses and this is not usually the case in OI. There have been no reports in the literature describing an infant with OI sustaining a true CML.
Even beyond the limits of biochemical and mutational testing, it is clear there are certain types of fractures that remain highly specific for abuse and are extremely suspicious when encountered in an infant. It should be recognized OI is, in the end, a rare disease and it is rarer still to be one of the 5% to 10% of patients with negative biochemical and mutational testing. Therefore, while OI is not ruled out as the result of negative laboratory analysis, any fracture must be considered very carefully if the patient is an infant and an appropriate history is not provided.
OI has also been called brittle bone disease in the common parlance. A separate term, temporary brittle bone disease (TBBD), refers to a report by Colin Paterson, a Scottish physician, of infants with suspicious fractures who, by his account, were not abused. According to Paterson, TBBD affects children under 6 months of age who sustain fractures during the course of normal handling and care and later no longer fracture [53, 54]. Paterson became a feature of many court cases in the United Kingdom and other countries in which the defense of TBBD was advanced, many times successfully. He emphasized the fractures occurred without a history of trauma or visible evidence of trauma, such as bruising, and without attendant internal injuries and the caregivers all denied wrongdoing [46]. His theory has been severely criticized on each of his points [1, 44]. Many abused children lack bruising, and while bruising is a helpful indicator of trauma, fractures occur frequently in the absence of bruising at any age. In addition, although associated injuries such as solid organ injury and retinal hemorrhages are common, it is by no means the rule. Finally, abusers tend to deny any culpability, some even after being found guilty in a court of law and in the face of overwhelming evidence. Because of his single-minded testimony at trial in support of this diagnosis, which included a lack of appropriate review of the records, among other inadequacies, Paterson was forbidden to act as an expert witness in the United Kingdom [15]. Later, in 2004, he was “struck out,” meaning his medical licensure was lifted [14]. In the United States, the TBBD defense cannot be used in many states’ courts of law and has been discredited.
Dr. Marvin Miller, an adherent of the TBBD concept, has advanced a possible theory that proposes a temporary state of increased bony fragility related to decreased fetal movement [46, 47]. His theory has been criticized for methodologic errors, including an incomplete description of the injuries, a subjective history of decreased fetal movement, and a long delay between bone mineral density measurements and the time of trauma [25]. In addition, his use of bone mineral density measurements is flawed in itself, as bone mineral density measurement is unreliable in young infants [16, 44]. The most recent normative values do not include values for those younger than 5 years [17, 44].
Recent Controversy
Most recently, Keller and Barnes [28] questioned whether neonatal rickets, mild in nature and related to decreased vitamin D in breast-feeding mothers, can be blamed for fractures occurring early in life. This contention has been criticized by Slovis and Chapman [61] on several counts, including a lack of observable findings of rickets that would include fraying and cupping of the physis on the published images from the original article. Indeed, one of the images of the distal ulna is claimed to show cupping consistent with rickets, but cupping of the distal ulna is a normal variant not associated with rickets as the sole finding [18]. Keller and Barnes [29] have since responded in kind, noting there are, by their account, other findings of rickets on the published images, among other assertions. At this point, the implication of these reports and replies is still unclear, but several points may be made. First, the theory of neonatal rickets as an explanation of CML-type injuries, if true, should only apply in those infants younger than 6 months since, over that age, most children have nutritional sources other than breast milk. Second, it should not apply in those infants younger than 6 months who are not breast fed. Third, a posteromedial rib fracture remains highly specific for abuse. Finally, each radiograph must be assiduously examined for even mild signs of rickets, which would include cupping and fraying of the metaphyses, a frayed bulbous appearance of the anterior ends of the ribs (rachitic rosary), and undermineralization of the bony structures. Note is made, in the majority, newborn bones are generally more sclerotic in appearance, with thick cortices and small medullary cavities, when compared to the bones of toddlers and children.
Miscellaneous Mimics
Mimics of abuse include conditions causing decreased sensation, including spinal dysraphism and congenital insensitivity to pain. In the former case, the diagnosis is usually known, but rarely an infant may present with a lower extremity fracture related to an undiagnosed diastematomyelia or other myelodysplasia. In congenital insensitivity to pain, multiple fractures may occur related to abnormal pain sensation. This rare syndrome can have both dominant and recessive inheritance, and injuries may mirror those seen in abuse [42, 63]. A diligent neurologic examination and clinical history that uncovers the patient’s lack of pain sensation should provide adequate differentiation from abuse.
Congenital syphilis causes fragmentation of the metaphyses and subperiosteal new bone formation along the diaphyses in newborns [22]. Both findings can simulate those seen in abuse. Clues to the correct diagnosis are the presence of Wimberger’s sign, seen as metaphyseal lucency in the medial subphyseal portion of the proximal tibia. It is usually bilateral and the defect spares the most recently formed few millimeters of the bone bark [52] and so should not be misconstrued as a true CML. Other radiographic abnormalities include trophic irregular metaphyseal lucent bands and focal lytic lesions, which represent syphilitic gummas, clearly not present in abuse.
Scurvy [7], vitamin A intoxication, Caffey’s disease, leukemia, and treatment with prostaglandin E all cause subperiosteal new bone formation [65], both diffusely and focally, and, to that limited extent, can be confused with abuse, but in each case, the related signs, symptoms, and radiographic changes provide easy differentiation from abuse. However, both copper deficiency and Menke’s kinky hair syndrome, itself an abnormality of copper metabolism, can be difficult to differentiate from abuse. Radiographic findings include osteopenia, subperiosteal new bone formation, and metaphyseal spurs with fractures indistinguishable from CMLs [21]. Patients may seize and usually manifest psychomotor retardation, although both may not be present in infancy. Wormian bones seen on skull radiographs are usually present and patients usually have sparse depigmented coarse hair [2]. The neurologic features and sparseness of the hair are the main clues to the correct diagnosis. Copper deficiency was advanced by Paterson with reference to TBBD, but no direct clinical or biologic proof was ever submitted [54]. Copper deficiency and Menke’s kinky hair syndrome can be confused with child abuse, but neither bears a sufficient resemblance to the unproven and oft-criticized diagnosis TBBD.
Discussion
This review was undertaken to describe the current knowledge regarding the radiographic diagnosis of child abuse. The literature review incorporates many articles from the literature combined with information taken from Dr. Paul Kleinman’s authoritative text on abuse to provide the orthopaedic surgeon with the correct information to recognize child abuse [30]. In addition to diagnosing what is child abuse, this review also addresses several disease and normal variants, which, while can be mistaken for abuse, are not in fact abuse. These include normal variant metaphyseal fragmentation commonly seen about the knee, as well as rickets, OI, syphilis, and Menke’s kinky hair syndrome, each of which may be difficult to differentiate from abuse.
Although the entity described as TBBD has been discredited, the controversy regarding nutritional rickets, specifically in breast-fed infants, is an active ongoing debate. The views of Keller and Barnes [28, 29], although largely criticized in the pediatric radiology literature, have not been scientifically disproven. The literature is very limited in the description of normative levels of vitamin D in nursing mothers and their infants, and further investigation is needed. Until then, a close examination of the radiographs is all the more necessary to indicate even mild signs of rickets. However, if no indication of rickets is seen, the films and the injuries recorded on those films should be taken at face value, and if indicative of abuse, whether it be by the finding of a classic MCL, posteromedial rib fracture, or an injury that does not agree with the given history, child abuse should be diagnosed and acted upon.
When suspicion of child abuse is raised, the radiographic investigation focuses on a carefully performed skeletal survey, including frontal images performed of each of the long bones on a separate image, single frontal images of each hand and foot, frontal views of the chest and abdomen, frontal and lateral views of the skull, and lateral views of the spinal column. Oblique views of the ribs are recommended and are very helpful. Each radiograph should be analyzed for findings of abuse, including those fractures that are highly specific for abuse, such as posteromedial rib fractures, CMLs, and scapular, sternal, and spinous process fractures. However, any fracture requires interpretation with respect to the history provided, and even low-specificity injuries, such as long-bone fractures, become very suspicious when a good history is not provided. Further views may be necessary, especially with small fields of view. Followup images and CT scanning are very useful adjuncts.
References
Ablin DS, Sane SM. Non-accidental injury: confusion with temporary brittle bone disease and mild osteogenesis imperfecta. Pediatr Radiol. 1997;27:111–113.
Adams PC, Strand RD, Bresnan MJ, Lucky AW. Kinky hair syndrome: serial study of radiological findings with emphasis on the similarity to the battered child syndrome. Radiology. 1974;112:401–407.
American College of Radiology. ACR practice guideline for skeletal surveys in children. Available at: http://www.acr.org/SecondaryMainMenuCategories/quality_safety/guidelines/pediatric/skeletal_surveys.aspx. Accessed September 11, 2009.
Astley R. Metaphyseal fractures in osteogenesis imperfecta. Br J Radiol. 1979;52:441–443.
Baldridge D, Schwarze U, Morello R, Lennington J, Bertin TK, Pace JM, Pepin MG, Weis M, Eyre DR, Walsh J, Lambert D, Green A, Robinson H, Michelson M, Houge G, Lindman C, Martin J, Ward J, Lemyre E, Mitchell JJ, Krakow D, Rimoin DL, Cohn DH, Byers PH, Lee B. CRTAP and LEPRE1 mutations in recessive osteogenesis imperfecta. Hum Mutat. 2008;29:1435–1442.
Barsness KA, Cha ES, Bensard DD, Calkins CM, Partrick DA, Karrer FM, Strain JD. The positive predictive value of rib fractures as an indicator of nonaccidental trauma in children. J Trauma. 2003;54:1107–1110.
Berant M, Jacobs J. A “pseudo” battered child. Clin Pediatr (Phila). 1966;5:230–237.
Blockley N. Observations on infantile coxa vara. J Bone Joint Surg Br. 1969;51:106–111.
Caffey J. On the theory and practice of shaking infants: its potential residual effects of permanent brain damage and mental retardation. Am J Dis Child. 1972;124:161–169.
Chapman S. The radiological dating of injuries. Arch Dis Child. 1992;67:1063–1065.
Dalton HJ, Slovis T, Helfer RE, Comstock J, Scheurer S, Riolo S. Undiagnosed abuse in children younger than 3 years with femoral fracture. Am J Dis Child. 1990;144:875–878.
Davies DV. Anatomy and physiology of diarthrodial joints. Ann Rheum Dis. 1945;5:29–35.
Dwek JR. The periosteum: what is it, where is it, and what mimics it in its absence? Skeletal Radiol. 2010;39:319–323.
Dyer O. GMC strikes off proponent of temporary brittle bone disease. BMJ. 2004;328:604.
Fisher J. Forensics Under Fire: Are Bad Science and Dueling Experts Corrupting Criminal Justice? New Brunswick, NJ: Rutgers University Press; 2008.
Gafni RI, Baron J. Overdiagnosis of osteoporosis in children due to misinterpretation of dual-energy x-ray absorptiometry (DEXA). J Pediatr. 2004;144:253–257.
Gilsanz V, Perez FJ, Campbell PP, Dorey FJ, Lee DC, Wren TA. Quantitative CT reference values for vertebral trabecular bone density in children and young adults. Radiology. 2009;250:222–227.
Glaser K. Double contour, cupping and spurring in roentgenograms of long bones in infants. Am J Roentgenol Radium Ther. 1949;61:482–492.
Glorieux FH, Rauch F, Plotkin H, Ward L, Travers R, Roughley P, Lalic L, Glorieux DF, Fassier F, Bishop NJ. Type V osteogenesis imperfecta: a new form of brittle bone disease. J Bone Miner Res. 2000;15:1650–1658.
Glorieux FH, Ward LM, Rauch F, Lalic L, Roughley PJ, Travers R. Osteogenesis imperfecta type VI: a form of brittle bone disease with a mineralization defect. J Bone Miner Res. 2002;17:30–38.
Grunebaum M, Horodniceanu C, Steinherz R. The radiographic manifestations of bone changes in copper deficiency. Pediatr Radiol. 1980;9:101–104.
Haicioglu O, Asik-Akman S, Yaprak I, Astarcioglu G, Imamoglu T, Reisoglu A. Physiological periostitis in a 2.5-month-old baby. Turk J Pediatr. 2009;51:305–307.
Hansen KK, Prince JS, Nixon GW. Oblique chest views as a routine part of skeletal surveys performed for possible physical abuse—is this practice worthwhile? Child Abuse Negl. 2008;32:155–159.
Helfer RE, Slovis TL, Black M. Injuries resulting when small children fall out of bed. Pediatrics. 1977;60:533–535.
Hicks R. Relating to methodological shortcomings and the concept of temporary brittle bone disease. Calcif Tissue Int. 2001;68:316–319.
Hui C, Joughin E, Goldstein S, Cooper N, Harder J, Kiefer G, Parsons D, Howard J. Femoral fractures in children younger than three years: the role of nonaccidental injury. J Pediatr Orthop. 2008;28:297–302.
Jones JC, Feldman KW, Bruckner JD. Child abuse in infants with proximal physeal injuries of the femur. Pediatr Emerg Care. 2004;20:157–161.
Keller KA, Barnes PD. Rickets vs. abuse: a national and international epidemic. Pediatr Radiol. 2008;38:1210–1216.
Keller KA, Barnes PD. Reply regarding rickets vs. abuse: the evidence. Pediatr Radiol. 2009;39:1130-1132.
Kleinman PK. Skeletal trauma: General considerations. In: Kleinman PK, ed. Diagnostic Imaging of Child Abuse. 2nd ed. St Louis, MO: Mosby Inc; 1998:9–10.
Kleinman PK, Belanger PL, Karellas A, Spevak MR. Normal metaphyseal radiologic variants not to be confused with findings of infant abuse. AJR Am J Roentgenol. 1991;156:781–783.
Kleinman PK, Marks SC, Blackbourne B. The metaphyseal lesion in abused infants: a radiologic-histopathologic study. AJR Am J Roentgenol. 1986;146:895–905.
Kleinman PK, Marks SC, Jr., Nimkin K, Rayder SM, Kessler SC. Rib fractures in 31 abused infants: postmortem radiologic-histopathologic study. Radiology. 1996;200:807–810.
Kleinman PK, Sarwar ZU, Newton AW, Perez-Rossello JM, Rebello G, Herliczek TW. Metaphyseal fragmentation with physiologic bowing: a finding not to be confused with the classic metaphyseal lesion. AJR Am J Roentgenol. 2009;192:1266–1268.
Kleinman PK, Schlesinger AE. Mechanical factors associated with posterior rib fractures: laboratory and case studies. Pediatr Radiol. 1997;27:87–91.
Kocher MS, Kasser JR. Orthopaedic aspects of child abuse. J Am Acad Orthop Surg. 2000;8:10–20.
Kwon DS, Spevak MR, Fletcher K, Kleinman PK. Physiologic subperiosteal new bone formation: prevalence, distribution, and thickness in neonates and infants. AJR Am J Roentgenol. 2002;179:985–988.
Laor T, Chun GF, Dardzinski BJ, Bean JA, Witte DP. Posterior distal femoral and proximal tibial metaphyseal stripes at MR imaging in children and young adults. Radiology. 2002;224:669–674.
Loder RT, Feinberg JR. Orthopaedic injuries in children with nonaccidental trauma: demographics and incidence from the 2000 kids’ inpatient database. J Pediatr Orthop. 2007;27:421–426.
Lyons TJ, Oates RK. Falling out of bed: a relatively benign occurrence. Pediatrics. 1993;92:125–127.
Magid N, Glass T. A “hole in a rib” as a sign of child abuse. Pediatr Radiol. 1990;20:334–336.
Makari GS, Carroll JE, Burton EM. Hereditary sensory neuropathy manifesting as possible child abuse. Pediatrics. 1994;93:842–844.
McCann RM, Colleary G, Geddis C, Clarke SA, Jordan GR, Dickson GR, Marsh D. Effect of osteoporosis on bone mineral density and fracture repair in a rat femoral fracture model. J Orthop Res. 2008;26:384–393.
Mendelson KL. Critical review of “temporary brittle bone disease.” Pediatr Radiol. 2005;35:1036–1040.
Merten DF, Kirks DR, Ruderman RJ. Occult humeral epiphyseal fracture in battered infants. Pediatr Radiol. 1981;10:151–154.
Miller ME. The lesson of temporary brittle bone disease: all bones are not created equal. Bone. 2003;33:466–474.
Miller ME, Hangartner TN. Temporary brittle bone disease: association with decreased fetal movement and osteopenia. Calcif Tissue Int. 1999;64:137–143.
Mizoguchi I, Nakamura M, Takahashi I, Kagayama M, Mitani H. An immunohistochemical study of localization of Type I and Type II collagens in mandibular condylar cartilage compared with tibial growth plate. Histochemistry. 1990;93:593–599.
Nimityongskul P, Anderson LD. The likelihood of injuries when children fall out of bed. J Pediatr Orthop. 1987;7:184–186.
Nimkin K, Kleinman PK, Teeger S, Spevak MR. Distal humeral physeal injuries in child abuse: MR imaging and ultrasonography findings. Pediatr Radiol. 1995;25:562–565.
O’Connor JF, Cohen J. Dating fractures. In: Kleinman PK, ed. Diagnostic Imaging of Child Abuse. 2nd ed. St Louis, MO: Mosby Inc; 1998:176.
Oestreich AE, Ahmad BS. The periphysis and its effect on the metaphysis. II. Application to rickets and other abnormalities. Skeletal Radiol. 1993;22:115–119.
Paterson CR. Osteogenesis imperfecta and other bone disorders in the differential diagnosis of unexplained fractures. J R Soc Med. 1990;83:72–74.
Paterson CR, Burns J, McAllion SJ. Osteogenesis imperfecta: the distinction from child abuse and the recognition of a variant form. Am J Med Genet. 1993;45:187–192.
Rex C, Kay PR. Features of femoral fractures in nonaccidental injury. J Pediatr Orthop. 2000;20:411–413.
Sandberg M, Vuorio E. Localization of Types I, II, and III collagen mRNAs in developing human skeletal tissues by in situ hybridization. J Cell Biol. 1987;104:1077–1084.
Scherl SA, Miller L, Lively N, Russinoff S, Sullivan CM, Tornetta P III. Accidental and nonaccidental femur fractures in children. Clin Orthop Relat Res. 2000; 376:96–105.
Shapiro F, Holtrop ME, Glimcher MJ. Organization and cellular biology of the perichondrial ossification groove of Ranvier: a morphological study in rabbits. J Bone Joint Surg Am. 1977;59:703–723.
Sillence DO, Rimoin DL. Classification of osteogenesis imperfect. Lancet. 1978;1:1041–1042.
Sillence DO, Senn A, Danks DM. Genetic heterogeneity in osteogenesis imperfecta. J Med Genet. 1979;16:101–116.
Slovis TL, Chapman S. Evaluating the data concerning vitamin D insufficiency/deficiency and child abuse. Pediatr Radiol. 2008;38:1221–1224.
Snedecor ST, Wilson HB. Some obstetrical injuries to the long bones. J Bone Joint Surg Am. 1949;31:378–384.
Spencer JA, Grieve DK. Congenital indifference to pain mistaken for non-accidental injury. Br J Radiol. 1990;63:308–310.
Swinson S, Tapp M, Brindley R, Chapman S, Offiah A, Johnson K. An audit of skeletal surveys for suspected non-accidental injury following publication of the British Society of Paediatric Radiology guidelines. Clin Radiol. 2008;63:651–656.
Ved N, Haller JO. Periosteal reaction with normal-appearing underlying bone: a child abuse mimicker. Emerg Radiol. 2002;9:278–282.
Wellington P, Bennet GC. Fractures of the femur in childhood. Injury. 1987;18:103–104.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
The author certifies that he has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Dwek, J.R. The Radiographic Approach to Child Abuse. Clin Orthop Relat Res 469, 776–789 (2011). https://doi.org/10.1007/s11999-010-1414-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-010-1414-5