
ABSTRACT
BACKGROUND
Churches may provide a familiar and accessible setting for chronic disease self-management education and social support for Latinos with diabetes.
OBJECTIVE
We assessed the impact of a multi-faceted church-based diabetes self-management intervention on diabetes outcomes among Latino adults.
DESIGN
This was a community-based, randomized controlled, pilot study.
SUBJECTS
One-hundred adults with self-reported diabetes from a Midwestern, urban, low-income Mexican-American neighborhood were included in the study.
INTERVENTIONS
Intervention participants were enrolled in a church-based diabetes self-management program that included eight weekly group classes led by trained lay leaders. Enhanced usual care participants attended one 90-minute lecture on diabetes self-management at a local church.
OUTCOME MEASURES
The primary outcome was change in glycosylated hemoglobin (A1C). Secondary outcomes included changes in low-density lipoproteins (LDL), blood pressure, weight, and diabetes self-care practices.
KEY RESULTS
Participants’ mean age was 54 ± 12 years, 81 % were female, 98 % were Latino, and 51 % were uninsured. At 3 months, study participants in both arms decreased their A1C from baseline (−0.32 %, 95 % confidence interval [CI]: -0.62, -0.02 %). The difference in change in A1C, LDL, blood pressure and weight from baseline to 3-month and 6-month follow-up was not statistically significant between the intervention and enhanced usual care groups. Intervention participants reported fewer days of consuming high fat foods in the previous week (−1.34, 95 % CI: -2.22, -0.46) and more days of participating in exercise (1.58, 95 % CI: 0.24, 2.92) compared to enhanced usual care from baseline to 6 months.
CONCLUSIONS
A pilot church-based diabetes self-management intervention did not reduce A1C, but resulted in decreased high fat food consumption and increased participation in exercise among low-income Latino adults with diabetes. Future church-based interventions may need to strengthen linkages to the healthcare system and provide continued support to participants to impact clinical outcomes.
Similar content being viewed by others


Latinos are almost twice as likely to have diabetes, less likely to achieve optimal glycemic control, at higher risk for developing complications, and have higher diabetes-related mortality compared to non-Hispanic whites.1–3 Diabetes self-management education is a critical component of care for all individuals with diabetes.4–6 While faith-based organizations are a promising setting in which to deliver diabetes self-management education (DSME) for African Americans with type 2 diabetes, few faith-based DSME interventions have taken place in Latino communities.7–10 Considering that more than two-thirds of Latinos identify themselves as Catholic and the majority of Latinos attend a church service at least once a month, church-based education programs in Latino communities can have a broad reach.10–12 While some DSME interventions targeting Latino patients have taken place in churches,13–15 few have worked collaboratively with church leaders in Latino communities to identify social and cultural issues related to diabetes management, actively engaged church leadership in the design of the intervention, and integrated church resources into the program, approaches that have been shown to improve patients’ diabetes outcomes in faith-based interventions.7
We used a community-based participatory research (CPBR) approach to partner with community leaders and members to design a church-based diabetes self-management intervention for Latinos.12,16–18 We trained lay leaders to lead the intervention classes since several studies have noted strong evidence for peer-led group self-management programs in improving self-management and clinical outcomes.13,19–27 To our knowledge, ours is the first study to evaluate the feasibility, acceptability, and clinical impact of a church-based diabetes self-management intervention among Latinos with diabetes.
METHODS
Our study was based in the South Lawndale neighborhood of Chicago, also known as Little Village, where more than 75 % of the population is of Mexican descent. We used a CBPR approach to partner with two Catholic churches, a Catholic social service agency, healthcare leaders, and community members for this study.16–18 The community partners formed the Little Village Community Advisory Board (CAB). We conducted a randomized, controlled, community-based intervention trial to test the impact of the church-based intervention on diabetes outcomes compared to enhanced usual care. Participants provided written informed consent before participating in the study and were followed for 6 months. The University of Chicago Institutional Review Board approved all study procedures, and this trial was registered at clinicaltrials.gov identifier NCT01288300.
Eligible participants were adults 18 years or older who were either English or Spanish speaking and self-reported receiving a diagnosis of diabetes by a physician. We excluded participants who were pregnant, only reported a diagnosis of gestational diabetes, were actively being treated for cancer, were on hemodialysis, were unable to attend the classes or follow-up appointments (e.g., due to extended travel), or were unable to provide informed consent.
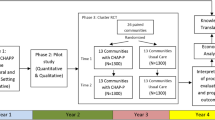
Participants were recruited from May 2011 to June 2012 at church-based events, such as health fairs, church services, adult educational classes, and other community events. Figure 1 describes participant screening and enrollment. Fifty-four percent of all eligible females agreed to participate versus 32 % of eligible males (p = 0.003). Attrition rates at 3 months (20 %) and 6 months (18 %) were not independently associated with randomization arm, age, gender, educational attainment, household income, primary language spoken, health literacy, insurance status or baseline A1C. After obtaining informed consent, trained bilingual research assistants collected baseline interview data in the participant’s preferred language (English or Spanish) and measured participants’ blood pressure, weight, height, and waist circumference. The research assistant randomized participants 1:1 to either the church-based intervention arm or enhanced usual care. Participants had blood samples drawn by venipuncture at baseline, 3 months, and 6 months post-randomization. A local Catholic social service agency and resource center, Taller de José, provided patient navigation services to participants. The intervention and enhanced usual care group participants received assistance from the patient navigators in finding a primary care provider if they did not already have one.

Study recruitment, enrollment and loss to follow-up flow diagram.
INTERVENTION: PICTURE GOOD HEALTH
Our church-based diabetes self-management intervention, “Picture Good Health/Imagínate una Buena Salud,” was designed by the academic team and the Little Village CAB.12,28 The curriculum consisted of eight weekly 90-minute group classes that took place at our two partnering churches and were led by two trained lay leaders. The curriculum was based on self-determination theory that emphasizes the importance of intrinsic motivation that underlies behavior change.29,30 The weekly classes incorporated information about diabetes and topics on nutrition and physical activity. Participants learned a cognitive approach to beha"Qvioral problem solving that included goal setting, anticipating likely obstacles, identifying behavioral alternatives, and stimulus control.31 While previous diabetes education interventions have ranged from 6 to 12 weeks, we found that an 8-week intervention would be acceptable to this community and would allow time to cover the content and skill areas also identified in our preliminary focus groups.15,24,28,32,33 Participants learned healthy preparation of traditional Mexican recipes and exercises they could do at home without special equipment. One aspect of a faith-based approach may include integrating religious scripture into the educational content. However, a review of African-American DSME church-based interventions found no difference in the health outcomes reported by interventions that included religious content and those that did not.7 In consultation with our church leaders and CAB, we decided not to include religious scripture in the educational content. Instead, our program promoted conversation around faith and spirituality by beginning each class with a prayer that aimed to provide a safe environment to speak on the role of faith in participants’ lives. Lay leaders were trained on how to facilitate conversations about faith and spirituality in the group classes.34 Previous studies have found that in church-based interventions, participants will insert spiritual strategies into the intervention even when religious content is not a part of the curriculum.7,35 Similarly, we found that participants often spoke about faith, God, and the role of spirituality in the group sessions. The curriculum also included a photovoice exercise, which is a CBPR method that engages community members through the use of photographs and storytelling.16,36 Participants were also informed of church-sponsored exercise programs they could attend.
The scientific team, CAB, and church leaders identified lay leaders from the church community to lead the classes. Lay leaders were not obligated to have formal medical training, but were required to be bilingual in written and spoken English and Spanish and have an interest in teaching about health. Similar to other studies, we did not specifically recruit lay leaders who had diabetes;21,25,33,37 however, all our lay leaders either had diabetes or had family members with diabetes. Lay leaders were invited to attend three 3-hour trainings that included training on program content and process, with emphasis on acquisition of coaching skills through modeling, role play, and feedback. The training was grounded in Social Cognitive Theory, the Transtheoretical Model, Self-Determination Theory, and principles of motivational interviewing.30,31,38,39 We trained our class leaders to support patient autonomy by acknowledging patients’ choices, to enhance self-efficacy through modeling and rehearsal of target behaviors, and to establish supportive and collaborative relationships.19,29,40,41 The training was led by the PI (AAB), project directors (CAL, AB), CAB members, a behavioral health specialist (MTQ), and a certified diabetes educator.42 In the training, lay leaders taught mock lessons, facilitated group discussions, and demonstrated their skill in coaching and patient-centered communication. Only lay leaders who demonstrated proficiency in these areas were invited to become class leaders. Members of the academic team observed class leaders during the first 8-week class and then periodically to ensure intervention fidelity using standard processes including checklists and direct observation.43,44 Class leaders received yearly booster sessions to review their skills and address any gaps in knowledge. All lay leaders completed human subjects training.
ENHANCED USUAL CARE ARM
Participants in the enhanced usual care arm were invited to a 90-minute lecture on diabetes self-management by a bilingual chronic disease health educator during the study period. At the end of the 6-month study period, participants in the enhanced usual care arm were invited to a less intensive 8-week group education class for equity purposes.12
OUTCOME MEASURES
The primary outcome measure was serum A1C which was collected by venipuncture. Direct LDL was also measured through the venipuncture sample. Blood pressure was reported as the average of the second and third readings.
All survey measures were collected through interviews at baseline and 6-month follow-up. Each interview took 30 to 45 min to complete. We assessed basic demographic information, such as participant age, gender, race/ethnicity, country of origin, time in the United States, employment status, household income, educational attainment, marital status, and language spoken at home. To understand participants’ access to healthcare, we asked them to report their type of health insurance, having a usual source of care, and having seen a physician in the past three months. To assess current health and healthcare, participants reported number of years with diabetes, self-reported complications of diabetes, comorbidities, self-reported health status, medications currently taking, smoking status, and recent physician or emergency room visits and hospitalizations. As secondary outcomes, we measured diabetes self-management using the Summary of Diabetes Self-Care Activities (SDSCA) scale,45 diabetes knowledge 46 and diabetes self-empowerment.47 As a part of the SDSCA, participants were asked: “On how many of the last 7 days did you eat high fat foods such as red meat or full-fat dairy products?” and “On how many of the last 7 days did you participate in a specific exercise session (such as swimming, walking, biking) other than what you do around the house or as part of your work?”
To assess feasibility and acceptability of the intervention, we assessed attendance in the intervention classes and participants gave feedback on the classes and the class leaders.
ANALYSIS
We compared participant characteristics in the intervention and enhanced usual care arm with the Student t test for continuous variables and the Pearson χ 2 test for categorical variables at baseline. To evaluate the intervention effect, we used linear mixed models that adjusted for repeated measures using terms for time (3 and 6 months), treatment arm, and time-by-treatment arm interaction. All participants with available follow-up measures were analyzed within their assigned group based on intent to treat principles. We used SAS version 9.2 (SAS Institute, Cary, NC) for all analyses and p < 0.05 was considered significant. A target sample size of 50 participants in each arm assumed a 0.57 % ± 1.0 % difference in decrease in A1C between the two arms with a power of 0.80. A decrease of 0.5 % is a clinically significant change per treatment guidelines and algorithms by the American Diabetes Association and the European Association for the Study of Diabetes in development of novel therapies for diabetes.48
RESULTS
Baseline Characteristics
The mean age of participants was 54 ± 12 years and 81 % of participants were female (Table 1). Ninety-eight percent of the participants were Latino, mostly of Mexican descent. Of the 100 participants, 76 % reported being affiliated with our two partnering churches, 22 % were affiliated with other churches, and 2 % did not report their affiliation. Only 3 % reported being in excellent or very good health. Forty-one percent of participants had an A1C less than or equal to 7.0 %.
Intervention participants had their post-intervention measures collected on average 42 ± standard deviation of 49 days after completing the 8-week intervention. The exit survey was completed at 123 ± 81 days and clinical measures were collected 151 ± 72 days from the end of the 8-week class. Enhanced usual care participants had their 3-month post-randomization measures collected 103 ± 21 days from baseline and 6-month post-randomization clinical measures were collected 215 ± 48 days from baseline.
Participants’ follow-up rates were 80 % at 3 months and 82 % at 6 months. Of the 50 intervention participants, 37 participants (74 %) attended at least one class; 29 participants (58 %) attended at least five of the eight classes. Thirty-five (70 %) out of 50 enhanced usual care participants attended the lecture.
Changes in Clinical Outcomes at 3- and 6-Month Follow-Up
At 3 months, study participants in both arms decreased their A1C from baseline (−0.32 %, 95 % confidence interval [CI]: -0.62, -0.02 %). The difference in change in A1C from baseline to follow-up at 6 months was not statistically significant between the two groups. (Table 2) The change in LDL, blood pressure, and weight from baseline to 3- and 6-month follow-up was not statistically significant between the intervention and enhanced usual care groups. Due to the small sample size, we were unable to calculate the adjusted change in weight across arms. In unadjusted analyses, there was no significant change in weight across arms at 3-month or 6-month follow-up. Only 20 % of enhanced usual care participants attended the 8-week class after the study period; these participants had no significant change in A1C from baseline to their post-study measure collected after going through the 8-week class. Within the intervention group, when attendance was assessed as a continuous variable, no significant differences in glycemic control were found.
Changes in Diabetes Self-Empowerment, Knowledge, Self-Rated Health, and Self-Care by Arm
Both groups improved their diabetes self-empowerment. (Table 3) There was no change in diabetes knowledge or self-reported health status within or across groups. The intervention group reported eating high fat foods on fewer days in the past week (−1.34 days, 95 % CI: −2.22, −0.46) and participating in a specific exercise program (such as swimming, walking, biking) more days (1.58 days, 95 % CI: 0.24, 2.92) compared to the enhanced usual care arm from baseline to 6 months.
Patient Navigation Services
Six participants in the intervention arm and two in enhanced usual care received assistance from the patient navigators.
Participant Satisfaction
Figure 2 describes participant satisfaction with the church-based intervention.

Participant satisfaction with church-based diabetes self-management intervention (n = 33)*.
DISCUSSION
Using a CBPR approach, we designed a church-based, culturally tailored, diabetes self-management intervention for Latinos and examined its impact on diabetes outcomes using a rigorous randomized trial design. While there were no differences in glycemic control, blood pressure, LDL, or weight across study arms at follow-up, participants in the church-based self-management intervention demonstrated significant improvements in diet and exercise compared to those in enhanced usual care at 6 months.
In our study, intervention participants were less likely to eat high-fat foods and more likely to participate in exercise at follow-up compared to participants who received a lecture on diabetes. Previous studies testing diabetes self-management interventions have had mixed results in impacting diabetes self-care activities.49,50 Considering that Latinos tend to struggle with lifestyle changes due to competing demands and lack of resources for lifestyle change, our study demonstrated the possibility of a church-based diabetes self-management intervention helping participants overcome their struggles in making behavior change.12,51 Even though these outcomes are self-reported, these findings are increasingly relevant since recent studies, including LOOK AHEAD, note that improvements in diet and exercise translate to improvements in many patient-centered outcomes, such as functional status and quality of life.52
Previous studies have found that Mexican Americans with diabetes believe faith plays an important role in their diabetes self-management and enables them to cope with their feelings about the disease.34,53 Underscoring this sentiment, more than 90 % of our intervention participants noted the importance of starting the class with the prayer. We believe that convening community members in a safe, trusted setting with people with whom they share a common language, culture and faith may have allowed participants to more openly share their struggles with diabetes and receive support. Our intervention also used photovoice to facilitate sharing. The use of this low-literacy exercise allowed participants to learn that many people shared similar challenges in managing their diabetes.
Our study found no differences in glycemic control across the study arms, echoing previous diabetes self-management intervention studies that have shown either short-term changes that were not sustained or no changes in clinical outcomes.33,49,50,54,55 While we did find that all participants had improvements in A1C at 3 months, this improvement was not sustained at 6 months. Participants may not have maintained the skills they gained after the weekly contact ended. A church-based diabetes self-management intervention may require a more intensive intervention, such as more or longer weekly group sessions and continued contact with participants to support maintenance of skills acquired during the intervention.15,22 Church-based diabetes self-management interventions may also need to provide feedback on patients’ progress to their primary care providers in order to impact metabolic outcomes.9 Since our study recruited participants from the community, not from hospitals or clinics where patients are already engaged in the healthcare system, our participants may have benefitted from stronger linkages to medical care. Future studies may need longer-term follow-up and a larger sample size to detect differences in clinical outcomes.
While some studies have demonstrated no improvements in diabetes outcomes using a lay leader approach,33,49,50,54–56 several other studies have noted that trained peers can effectively lead self-management education interventions in community settings and improve clinical outcomes.13,19,20,22–24,26,27,57–60 Studies with Mexican Americans with diabetes utilizing peer-led diabetes self-management interventions have found improvements in glucose control.22,23,25–27 There is still a need for ongoing work to understand what training is required and the qualities that enable a person to become an effective peer leader in Latino communities.20,22,37,61,62 In our intervention, we included key elements of peer-led group self-management classes that have been noted to be successful in previous interventions and utilized efficacious behavioral approaches, such as social cognitive theory, empowerment, and motivational interviewing.19 While our peer leader training had a strong behavioral approach, we may need to provide lay leaders with more frequent feedback on teaching performance, opportunities to practice motivational interviewing skills outside of the classroom, further skill building on how to foster patient autonomy and enhance patient self-efficacy, and multiple refresher training sessions to fully equip our lay leaders in promoting behavior change and impacting patients’ clinical outcomes.19
Limitations
Our study has some limitations. Our findings may not be generalized to all Latino populations since we mainly recruited from one urban, Mexican American neighborhood in a Midwestern city. Self-report could be heavily influenced by social desirability bias such that more participants could have reported making changes in their behavior than actually did. Participants from the same church may have been randomized to different arms, thus leading to the potential for contamination. A 6-month follow-up period may not have been enough time for behavioral changes to have an effect on outcomes. While the participants’ follow-up rates of 80 % at 3 months and 82 % at 6 months are high for studies in low-income immigrant populations, it is possible that attrition introduced bias. Many participants had a normal or at-target baseline A1C, which may have limited our ability to further decrease their A1C.15,33 Our study was also underpowered to detect small differences in change in A1C. The difference in attention received by participants in the two arms may have potentially biased the results of the study. Lastly, it is difficult to ascertain which aspects of the intervention, such as the use of lay leaders, the social support gained from the group education, or the photovoice activities, may have had the strongest impact on self-care.
A pilot church-based diabetes self-management intervention did not reduce A1C, but resulted in decreased high fat food consumption and increased participation in exercise among low-income Latino adults with diabetes. This study underscores the need for collaborative designs of community-based interventions and rigorous evaluations that can offer solutions to improve health behavior among Latinos with diabetes.
REFERENCES
Centers for Disease Control and Prevention. Diabetes Report Card 2012. Atlanta: Centers for Disease Control and Prevention, US Department of Health and Human Services; 2012.
Saydah S, Cowie C, Eberhardt MS, De Rekeneire N, Narayan KM. Race and ethnic differences in glycemic control among adults with diagnosed diabetes in the United States. Ethnic Dis. 2007;17(3):529–35.
Spanakis EK, Golden SH. Race/ethnic difference in diabetes and diabetic complications. Curr Diab Rep. 2013;13(6):814–23.
Strine TW, Okoro CA, Chapman DP, Beckles GL, Balluz L, Mokdad AH. The impact of formal diabetes education on the preventive health practices and behaviors of persons with type 2 diabetes. Prev Med. 2005;41(1):79–84.
Cauch-Dudek KVJ, Sigmond M, Shah BR. Disparities in attendance at diabetes self-management education programs after diagnosis in Ontario Canada: a cohort study. BMC Public Health. 2013;13:85. doi:10.1186/1471-2458-1113-1185.
Peyrot M, Rubin RR, Funnell MM, Siminerio LM. Access to diabetes self-management education: results of national surveys of patients, educators, and physicians. Diab Educ. 2009;35(2):246–8. 252-246, 258-263.
Newlin K, Dyess SM, Allard E, Chase S, Melkus GD. A methodological review of faith-based health promotion literature: advancing the science to expand delivery of diabetes education to Black Americans. J Relig Health. 2012;51(4):1075–97.
Norris SL, Nichols PJ, Caspersen CJ, et al. Increasing diabetes self-management education in community settings. a systematic review. Am J Prev Med. 2002;22(4 Suppl):39–66.
Baig AA, Mangione CM, Sorrell-Thompson AL, Miranda JM. A randomized community-based intervention trial comparing faith community nurse referrals to telephone-assisted physician appointments for health fair participants with elevated blood pressure. J Gen Intern Med. 2010;25(7):701–9.
Zahuranec DB, Morgenstern LB, Garcia NM, et al. Stroke health and risk education (SHARE) pilot project: feasibility and need for church-based stroke health promotion in a bi-ethnic community. Stroke. 2008;39(5):1583–5.
Pew Hispanic Center and Pew Forum on Relgion & Public Life. Changing Faiths: Latinos and the Transformation of American Religion. 2007. http://pewhispanic.org/reports/report.php?ReportID=75. Accessed March 3, 2015.
Baig AA, Locklin CA, Wilkes AE, et al. Integrating diabetes self-management interventions for mexican-americans into the catholic church setting. J Relig Health. 2014;53(1):105–18.
Glazier RH, Bajcar J, Kennie NR, Willson K. A systematic review of interventions to improve diabetes care in socially disadvantaged populations. Diabetes Care. 2006;29(7):1675–88.
Lorig K, Ritter PL, Villa F, Piette JD. Spanish diabetes self-management with and without automated telephone reinforcement: two randomized trials. Diabetes Care. 2008;31(3):408–14.
Brown SA, Garcia AA, Kouzekanani K, Hanis CL. Culturally competent diabetes self-management education for Mexican Americans the starr county border health initiative. Diabetes Care. 2002;25(2):259–68.
Israel BA, Eng E, Schulz AJ, Parker EA, eds. Methods in community-based participatory research for health. San Francisco: Jossey-Bass; 2005:31–51.
Jones L, Wells K. Strategies for academic and clinician engagement in community-participatory partnered research. JAMA. 2007;297(4):407–10.
Wells K, Jones L. “Research” in community-partnered, participatory research. JAMA. 2009;302(3):320–1.
Heisler M. Different models to mobilize peer support to improve diabetes self-management and clinical outcomes: evidence, logistics, evaluation considerations and needs for future research. Fam Pract. 2010;27(Suppl 1):i23–32.
Funnell MM. Peer-based behavioural strategies to improve chronic disease self-management and clinical outcomes: evidence, logistics, evaluation considerations and needs for future research. Fam Pract. 2010;27(Suppl 1):i17–22.
Tang TS, Nwankwo R, Whiten Y, Oney C. Outcomes of a church-based diabetes prevention program delivered by peers: a feasibility study. Diab Educ. 2014;40(2):223–30.
Tang TS, Funnell M, Sinco B, et al. Comparative effectiveness of peer leaders and community health workers in diabetes self-management support: results of a randomized controlled trial. Diabetes Care. 2014;37(6):1525–34.
Philis-Tsimikas A, Fortmann A, Lleva-Ocana L, Walker C, Gallo LC. Peer-led diabetes education programs in high-risk Mexican Americans improve glycemic control compared with standard approaches: a Project Dulce promotora randomized trial. Diabetes Care. 2011;34(9):1926–31.
Gilmer TP, Philis-Tsimikas A, Walker C. Outcomes of project dulce: a culturally specific diabetes management program. Ann Pharmacother. 2005;39(5):817–22.
Prezio EA, Cheng D, Balasubramanian BA, Shuval K, Kendzor DE, Culica D. Community Diabetes Education (CoDE) for uninsured Mexican Americans: a randomized controlled trial of a culturally tailored diabetes education and management program led by a community health worker. Diabetes Res Clin Pract. 2013;100(1):19–28.
Rothschild SK, Martin MA, Swider SM, et al. Mexican American trial of community health workers: a randomized controlled trial of a community health worker intervention for Mexican Americans with type 2 diabetes mellitus. Am J Public Health. 2014;104(8):1540–8.
Spencer MS, Rosland AM, Kieffer EC, et al. Effectiveness of a community health worker intervention among African American and Latino adults with type 2 diabetes: a randomized controlled trial. Am J Public Health. 2011;101(12):2253–60.
Baig AA, Locklin CA, Wilkes AE, et al. “One can learn from other people’s experiences”: Latino adults’ preferences for peer-based diabetes interventions. Diab Educ. 2012;38(5):733–41.
Anderson RM. Patient empowerment and the traditional medical model. A case of irreconcilable differences? Diabetes Care. 1995;18(3):412–5.
Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55(1):68–78.
Bandura A. Health promotion by social cognitive means. Health Educ Behav. 2004;31(2):143–64.
Anderson RM, Funnell MM, Butler PM, Arnold MS, Fitzgerald JT, Feste CC. Patient empowerment. results of a randomized controlled trial. Diabetes Care. 1995;18(7):943–9.
Lorig K, Ritter PL, Villa FJ, Armas J. Community-based peer-led diabetes self-management: a randomized trial. Diabetes Educ. 2009;35(4):641–51.
Hunt LM, Arar NH, Akana LL. Herbs, prayer, and insulin. use of medical and alternative treatments by a group of Mexican American diabetes patients. J Fam Pract. 2000;49(3):216–23.
Yanek LR, Becker DM, Moy TF, Gittelsohn J, Koffman DM. Project Joy: faith based cardiovascular health promotion for African American women. Public Health Rep (Washington, DC : 1974). 2001;116(Suppl 1):68–81.
Wang CBM. Photovoice: concept, methodology, and use for participatory needs assessment. Health Educ Behav. 1997;24(3):369–87.
Tang TS, Nwankwo R, Whiten Y, Oney C. Training peers to deliver a church-based diabetes prevention program. Diabetes Educ. 2012;38(4):519–25.
Velicer WFDC, Rossi JS, Prochaska JO. Relapse situations and self-efficacy: an integrative model. Addict Behav. 1990;15(3):271–83.
Miller WR, Rose GS. Toward a theory of motivational interviewing. Am Psychol. 2009;64(6):527–37.
Peyrot M, Rubin RR. Behavioral and psychosocial interventions in diabetes: a conceptual review. Diabetes Care. 2007;30(10):2433–40.
Funnell MM, Anderson RM, Arnold MS, et al. Empowerment: an idea whose time has come in diabetes education. Diabetes Educ. 1991;17(1):37–41.
Deakin T, McShane CE, Cade JE, Williams RD. Group based training for self-management strategies in people with type 2 diabetes mellitus. The Cochrane database of systematic reviews. 2005(2):Cd003417.
Horner S, Rew L, Torres R. Enhancing intervention fidelity: a means of strengthening study impact. J Spec Pediatr Nurs. 2006;11(2):80–9.
Bellg AJ, Borrelli B, Resnick B, et al. Enhancing treatment fidelity in health behavior change studies: best practices and recommendations from the NIH Behavior Change Consortium. Health Psychol : Off J Div Health Psychol, Am Psychol Assoc. 2004;23(5):443–51.
Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care activities measure: results from 7 studies and a revised scale. Diabetes Care. 2000;23(7):943–50.
Garcia AA, Villagomez ET, Brown SA, Kouzekanani K, Hanis CL. The starr county diabetes education study: development of the Spanish-language diabetes knowledge questionnaire. Diabetes Care. 2001;24(1):16–21.
Anderson RM, Fitzgerald JT, Gruppen LD, Funnell MM, Oh MS. The diabetes empowerment scale-short form (DES-SF). Diabetes Care. 2003;26(5):1641–2.
Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the study of diabetes. Diabetes Care. 2009;32(1):193–203.
Frosch DL, Uy V, Ochoa S, Mangione CM. Evaluation of a behavior support intervention for patients with poorly controlled diabetes. Arch Intern Med. 2011;171(22):2011–7.
Rosal MC, Ockene IS, Restrepo A, et al. Randomized trial of a literacy-sensitive, culturally tailored diabetes self-management intervention for low-income latinos: latinos en control. Diabetes Care. 2011;34(4):838–44.
Kieffer EC, Willis SK, Odoms-Young AM, et al. Reducing disparities in diabetes among African-American and Latino residents of Detroit: the essential role of community planning focus groups. Ethnic Dis. 2004;14(3 Suppl 1):S27–37.
Wing RR, Bolin P, Brancati FL, et al. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med. 2013;369(2):145–54.
Caban A, Walker EA. A systematic review of research on culturally relevant issues for Hispanics with diabetes. Diabetes Educ. 2006;32(4):584–95.
Samuel-Hodge CD, Keyserling TC, Park S, Johnston LF, Gizlice Z, Bangdiwala SI. A randomized trial of a church-based diabetes self-management program for African Americans with type 2 diabetes. Diabetes Educ. 2009;35(3):439–54.
Toobert DJ, Strycker L, King D, Barrera M Jr, Osuna D, Glasgow R. Long-term outcomes from a multiple-risk-factor diabetes trial for Latinas: ¡Viva Bien! Behav Med Pract Policy Res. 2011;1(3):416–26.
Barrera M Jr, Toobert D, Strycker L. Relative contributions of naturalistic and constructed support: two studies of women with type 2 diabetes. J Behav Med. 2014;37(1):59–69.
Norris SL, Chowdhury FM, Van Le K, et al. Effectiveness of community health workers in the care of persons with diabetes. Diab Med : J British Diab Assoc. 2006;23(5):544–56.
Viswanathan M, Kraschnewski J, Nishikawa B, et al. Outcomes of community health worker interventions. Evidence report/technology assessment. 2009(181):1–144, A141-142, B141-114, passim.
Two Feathers J, Kieffer EC, Palmisano G, et al. Racial and Ethnic Approaches to Community Health (REACH) Detroit partnership: improving diabetes-related outcomes among African American and Latino adults. Am J Public Health. 2005;95(9):1552–60.
Cherrington A, Ayala GX, Amick H, Allison J, Corbie-Smith G, Scarinci I. Implementing the community health worker model within diabetes management: challenges and lessons learned from programs across the United States. Diabetes Educ. 2008;34(5):824–33.
Tang TS, Funnell MM, Gillard M, Nwankwo R, Heisler M. The development of a pilot training program for peer leaders in diabetes: process and content. Diabetes Educ. 2011;37(1):67–77.
Tang TS, Funnell MM, Gillard M, Nwankwo R, Heisler M. Training peers to provide ongoing diabetes self-management support (DSMS): results from a pilot study. Patient Educ Couns. 2011;85(2):160–8.
Acknowledgements
We would like to thank our partnering churches and Esperanza Health Centers for donating their space and personnel for our study. We would like to thank the research assistants who made this study possible: Maria Acevedo, Jason Espinoza, Patricia Fernandez Piñeros, Maritza Gómez, Alexis Lopez, Ana Luisa Piña, Denise Salinas, Matthew Stutz, Fernando Vázquez, and Helio Zapata. We are also indebted to our class leaders Javier Ávila, María Medina, Claudia Velazquez, and Samuel Villaseñor and to the Taller de José compañeros for accompanying and providing patient navigation services to our participants. This research was supported by grants from University of Chicago Clinical and Translational Science Award (UL1RR024999), the National Institute of Diabetes and Digestive and Kidney Diseases Diabetes Research and Training Center (P60 DK20595) and the Chicago Center for Diabetes Translation Research (P30 DK092949). Dr. Baig is supported by a NIDDK Mentored Patient-Oriented Career Development Award (K23 DK087903-01A1). Dr. Chin is supported by a NIDDK Midcareer Investigator Award in Patient-Oriented Research (K24 DK071933). The local Walgreens provided a discount on photograph development for the intervention classes. Bayer provided some free boxes of test strips for participants. This paper was presented at the annual meeting of the Society of General Internal Medicine on 27 April 2013.
Conflict of Interest
The authors declare no conflicts of interest.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
This trial was registered at clinicaltrials.gov identifier NCT01288300.
The members of the Little Village Community Advisory Board are John C. Acevedo, MSW, Loyola University Chicago; Sr. Kathleen Brazda, CSJ, MA, Taller de José; Dolores Castañeda, BS, St. Agnes of Bohemia Parish; Daniel Fulwiler, MPH, MA, Esperanza Health Centers; Laura Garcia, PharmD, Walgreens Co.; Lisa Monnot, MNM, Taller de José; Andrea Muñoz, MS, St. Agnes of Bohemia Parish; Frances E. Nance, Lawndale Christian Health Center; Donna Oborski, BSN, FCN, Advocate Health Care and Our Lady of Tepeyac Parish; Azucena Urbina, Lawndale Christian Health Center; and Asenet Vallejo, Esperanza Health Centers.
Rights and permissions
About this article

Cite this article
Baig, A.A., Benitez, A., Locklin, C.A. et al. Picture Good Health: A Church-Based Self-Management Intervention Among Latino Adults with Diabetes. J GEN INTERN MED 30, 1481–1490 (2015). https://doi.org/10.1007/s11606-015-3339-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-015-3339-x