
Abstract
Background
There have been no comparative studies of endoscopic submucosal dissection (ESD) and laparoscopic and endoscopic cooperative surgery (LECS) for patients with duodenal tumors regarding surgical outcomes. The aim of this study is to compare the safety and feasibility of short-term surgical outcomes of ESD and LECS for patients with low-risk tumors of the duodenum.
Methods
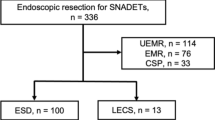
This was a single-center retrospective study of 68 consecutive patients with low-risk tumors of the duodenum who received surgical treatments. ESD (n = 50) was performed between 2000 and 2013 and LECS (n = 18) was performed between 2014 and 2017.
Results
The overall incidence of perioperative complications was significantly higher in the ESD group (28%) than in the LECS group (0%) (P = 0.014). In the ESD group, eight patients with intraoperative perforation of duodenum (16%) were repaired with metal clips. Postoperative duodenal hemorrhage occurred in three patients (6%). Postoperative duodenal stricture requiring endoscopically guided balloon dilation was observed in two patients (4%). Postoperative bile leakage was found in one patient (2%). The size of resected lesion was significantly larger in the LECS group (26.5 mm) than in the ESD group (14.5 mm) (P = 0.003). In LECS group, all 18 patients underwent curative resection; however, the curative resection rate was 52% in ESD group (P = 0.001).
Conclusion
LECS for patients with low-risk tumors of the duodenum is a safe, feasible, and ideal alternative to ESD with regard to short-term surgical outcomes.
Trial Registration
UMIN000021200 (http://www.umin.ac.jp/ctr/)


Similar content being viewed by others


References
Stauffer JA, Raimondo M, Woodward TA, Goldberg RF, Bowers SP, Asbun HJ. Laparoscopic partial sleeve duodenectomy (PSD) for nonampullary duodenal neoplasms: avoiding a whipple by separating the duodenum from the pancreatic head. Pancreas 2013;42:461–466.
Tanaka E, Kim M, Lim JS, Choi YY, Saklani A, Noh SH, Hyung WJ. Usefulness of laparoscopic side-to-side duodenojejunostomy for gastrointestinal stromal tumors located at the duodenojejunal junction. J Gastrointest Surg 2015;19:313–318.
Ichikawa D, Komatsu S, Dohi O, Naito Y, Kosuga T, Kamada K, Okamoto K, Itoh Y, Otsuji E. Laparoscopic and endoscopic co-operative surgery for non-ampullary duodenal tumors. World J Gastroenterol 2016;22:10424–10431.
Shibagaki K, Ishimura N, Kinoshita Y. Endoscopic submucosal dissection for duodenal tumors. Ann Transl Med 2017;5:188.
Klein A, Nayyar D, Bahin FF, Qi Z, Lee E, Williams SJ, Byth K, Bourke MJ. Endoscopic mucosal resection of large and giant lateral spreading lesions of the duodenum: success, adverse events, and long-term outcomes. Gastrointest Endosc 2016;84:688–696.
Kim TW, Kim GH, Park DY, Ahn S, Lim W, Lee BE, Song GA. Endoscopic resection for duodenal subepithelial tumors: a single-center experience. Surg Endosc 2017;31:1936–1946.
Ono H, Kaise M, Nonaka S, Uedo N, Hirasawa T, Koyama T, Toyonaga T, Doyama H, Kodashima S, Hirasawa K, Tanabe S, Yamamoto K, Kaneko K. Clinical Issues of Duodenal Endoscopic Treatment. Stomach and Intestine 2016;51:1585–1592. (Japanese) Available online: http://medicalfinder.jp/doi/10.11477/mf.1403200770
Hiki N, Yamamoto Y, Fukunaga T, Yamaguchi T, Nunobe S, Tokunaga M, Miki A, Ohyama S, Seto Y. Laparoscopic and endoscopic cooperative surgery for gastrointestinal stromal tumor dissection. Surg Endosc 2008;22:1729–1735.
Irino T, Nunobe S, Hiki N, Yamamoto Y, Hirasawa T, Ohashi M, Fujisaki J, Sano T, Yamaguchi T. Laparoscopic-endoscopic cooperative surgery for duodenal tumors: a unique procedure that helps ensure the safety of endoscopic submucosal dissection. Endoscopy 2015;47:349–351.
Edge SE, Byrd DR, Carducci MA, Compton CA. AJCC Cancer Staging Manual, Seventh Edition. New York: Springer 2011.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004;240:205–213.
Ojima T, Takifuji K, Nakamura M, Iwahashi M, Nakamori M, Katsuda M, Iida T, Hayata K, Yamaue H. Complications of endoscopic submucosal dissection for gastric noninvasive neoplasia: an analysis of 647 lesions. Surg Laparosc Endosc Percutan Tech 2014;24:370–374.
Ojima T, Takifuji K, Nakamura M, Nakamori M, Katsuda M, Iida T, Hayata K, Iwahashi M, Yamaue H. Endoscopic submucosal dissection for gastric tumors in various types of remnant stomach. Endoscopy 2014;46:645–649.
Ojima T, Nakamura M, Nakamori M, Takifuji K, Hayata K, Katsuda M, Takei Y, Yamaue H. Laparoscopic and endoscopic cooperative surgery is a feasible treatment procedure for intraluminal gastric gastrointestinal stromal tumors compared to endoscopic intragastric surgery. Surg Endosc 2017;https://doi.org/10.1007/s00464-017-5683-x.
Wong J, Cheung H, Lui R, Fan YW, Smith A, Siu KF. Esophagogastric anastomosis performed with a stapler: the occurrence of leakage and stricture. Surgery 1987;101:408–415.
Author information
Authors and Affiliations
Contributions
Study concept and design: Ojima and Yamaue. Acquisition of data: Ojima, Nakamori, Nakamura, and Takifuji. Analysis and interpretation of data: Ojima, Nakamori, and Nakamura. Drafting of the manuscript: Ojima, Nakamura, and Hayata. Critical revision of the manuscript for important intellectual content: Yamaue. Statistical analysis: Ojima, Hayata, Katsuda, and Yamaue. Administrative, technical, and material support: Hayata, Takifuji, and Yamaue. Study supervision: Yamaue
Corresponding author
Ethics declarations
Informed consent was obtained from all patients in accordance with the guidelines of the WMUH Ethics Committee on Human Research. The study protocol was registered at the University Hospital Medical Information Network (UMIN000021200).
Conflict of Interest
The authors declare that they have no conflicts of interests.
Electronic Supplementary Material
Rights and permissions
About this article

Cite this article
Ojima, T., Nakamori, M., Nakamura, M. et al. Laparoscopic and Endoscopic Cooperative Surgery Versus Endoscopic Submucosal Dissection for the Treatment of Low-Risk Tumors of the Duodenum. J Gastrointest Surg 22, 935–940 (2018). https://doi.org/10.1007/s11605-018-3680-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-018-3680-6