
Abstract
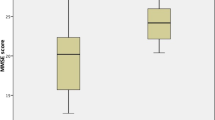
The influence of carotid stenosis and its surgical treatment on brain function is still poorly defined. We therefore performed a study to assess psychometric and quantified EEG findings after carotid endarterectomy (CEA). Sixty-nine non-demented patients (aged 72 ± 7 years) with severe carotid stenosis (≥70 %) eligible for CEA were studied. Forty patients (group A) had unilateral stenosis, and 29 patients (group B) had bilateral stenosis. Before and 5 months after CEA all the patients were evaluated by the Trail Making Test A, the Symbol Digit Test, and spectral EEG analysis. At baseline, compared to group A, group B patients performed slowly the Trail Making Test A (Z: 1.45 ± 1.4 vs. 0.76 ± 1.3; p < 0.05), but not the Symbol Digit Test (Z: 0.83 ± 1.38 vs. 0.64 ± 1.26; p = 0.59). Altogether, the patients with at least one abnormal psychometric test were 29 % (group A: 26 %; group B: 33 %, p = 0.56). The EEG did not differ significantly between patients of group A compared to group B. After CEA, psychometric tests improved (mean Z score from 0.73 ± 1.12 to 0.45 ± 1.15, p < 0.05). The improvement was similar in group A and B. The EEG mean dominant frequency improved only in group B patients and it was related to the improvement in psychometric tests (r = 0.43, p = 0.05). Low psychometric performance was detectable in about 1/ 3 of non-demented patients with severe carotid stenosis. CEA improved mental performance and, in patients with severe bilateral stenosis, accelerated the EEG frequency.


Similar content being viewed by others

References
Amodio P, Marchetti P, Del Piccolo F, de Tourtchaninoff M, Varghese P, Zuliani C, Campo C, Gatta A, Guérit JM (1999) Spectral versus visual EEG analysis in mild hepatic encephalopathy. Clin Neurophysiol 110(8):1334–1344
Amodio P, Helmut W, Del Piccolo F, Mapelli D, Montagnese S, Pellegrini A, Gatta A, Umiltà C (2002) Variability of trailmaking tests, symbol digit test and line trait test in normal people. A normative study taking into account age-dependent decline and sociobiological variables. Aging Clin Exp Res 14:117–131
Benke T, Neussl D, Aichner F (1991) Neuropsychological deficits in asymptomatic carotid artery stenosis. Acta Neurol Scand 83:378–381
Brott TG, Halperin JL, Abbara S et al (2011) 2011 ASA/ACCF /AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS guideline on the management of patients with extracranial carotid and vertebral artery disease: executive summary. Circulation 124:489–532
Casey JE, Ferguson GG, Kimura D, Hachinski VC (1989) Neuropsychological improvement versus practice effect following unilateral carotid endarterectomy in patients without stroke. J Clin Exp Neuropsychol 11:461–470
De Leo D, Serraiotto L, Pellegrini C, Magni G, Franceschi L, Deriu GP (1987) Outcome from carotid endarterectomy. Neuropsychological performances, depressive symptoms and quality of life: 8-month follow-up . Int J Psychiatry Med 17:317–325
Folstein MF, Folstein SE, McHugh PR (1975) “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198
Forette F, Seux ML, Staessen JA, Thijs L, Birkenhager WH, Babarskiene MR et al (1998) Prevention of dementia in randomised double-blind placebo-controlled systolic hypertension in Europe (Syst-Eur) trial. Lancet 352:1347–1351
Greenlief CL, Margolis RB, Erker GJ (1985) Application of the trail making test in differentiating neuropsychological impairment of elderly persons. Percept Mot Skills 61:1283–1289
Hart RP, Kwentus JA, Wade JB, Hamer RM (1987) Digit symbol performance in mild dementia and depression. J Consult Clin Psychol 55:236–238
Hemmingsen R, Mejsholm B, Vorstrup S, Lester J, Engell HC (1986) Boysen G (1986) Carotid surgery, cognitive function, and cerebral blood flow in patients with transient ischemic attacks. Ann Neurol 20:13–19
Kawamura S, Sayama I, Yasui N, Uemura K (1994) Haemodynamic and metabolic changes following extra-intracranial bypass surgery. Acta Neurochir 126:135–139
Kelly MP, Garron DC, Javid H (1980) Carotid artery disease, carotid endarterectomy, and behavior. Arch Neurol 37:743–748
King GD, Gideon DA, Haynes CD, Dempsey RL, Jenkins CW (1977) Intellectual and personality changes associated with carotid endarterectomy. J Clin Psychol 33:215–220
Klem GH, Luders HO, Jasper HH, Elger C (1999) The ten-twenty electrode system of the International federation. The International Federation of Clinical Neurophysiology. Electroencephalogr Clin Neurophysiol Suppl 52:3–6
Leininger BE, Gramling SE, Farrell AD, Kreutzer JS, Peck EA (1990) Neuropsychological deficits in symptomatic minor head injury patients after concussion and mild concussion. J Neurol Neurosurg Psychiatry 53:293–296
Lezak MD (1995) Neuropsychological assessment. Oxford University Press, New York Oxford, pp 376–384
Lunn S, Crawley F, Harrison MJ, Brown MM, Newman SP (1999) Impact of carotid endarterectomy upon cognitive functioning. A systematic review of the literature. Cerebrovasc Dis 9:74–81
Madkour O, Elwan O, Hamdy H, Elwan H, Abbas A, Taher M, Abdel-Kader A (1993) Transient ischemic attacks: electrophysiological conventional and topographic EEG) and radiological (CCT) evaluation. J Neurol Sci 119(1):8–17
Madl C, Grimm G, Kramer L, Koppensteiner R, Hirschl M, Yeganehfar W, Hirschl MM, Ugurluoglu A, Schneider B, Ehringer H (1994) Cognitive brain function in non-demented patients with low-grade and high-grade carotid artery stenosis. Eur J Clin Investig 24:559–564
Montagnese S, Schiff S, Realdi A, Inverso G, Pellegrini A, Iannizzi P, Manara R, Mapelli D, Amodio P, Semplicini A (2013) Abnormal cerebral electrogenesis is associated with impaired cognitive performance in hypertensive patients. J Hum Hypertens 27:463–464
Pascoli D, Guérit JM, Montagnese S, De Tourtchaninoff M, Minelli T, Pellegrini A, Del Piccolo F, Gatta A, Amodio P (2006) Analysis of EEG tracings in frequency and time domain in hepatic encephalopathy. Comput Methods Programs Biomed 81(3):203–212
Paulman RG, Koss E, MacInnes WD (1996) Neuropsychological evaluation of dementia. In: Weiner MF (ed) The dementias: diagnosis, management and research. American Psychiatric Press, Inc, Washington, pp 211–232
Powers WJ (1991) Cerebral hemodynamics in ischemic cerebrovascular disease. Ann Neurol 29:231–240
Powers WJ, Press GA, Grubb RL Jr, Gado M, Raichle ME (1987) The effect of hemodynamically significant carotid artery disease on the hemodynamic status of the cerebral circulation. Ann Intern Med 106:27–34
Quero JC, Hartmann IJ, Meulstee J, Hop WC, Schalm SW (1996) The diagnosis of subclinical hepatic encephalopathy in patients with cirrhosis using neuropsychological tests and automated electroencephalogram analysis. Hepatology 24:556–560
Reitan RM (1958) Validity of the trail making test as an indicator of organic brain damage. Percept Mot Skills 8:271–276
Russell EW (1972) A WAIS factor analysis with brain damaged subjects using criterion measures. J Consult Clin Psychol 39:133–139
Semplicini A, Maresca A, Simonella C, Chierichetti F, Pauletto P, Meneghetti G, Ferlin G, Pessina AC (2000) Cerebral perfusion in hypertensives with carotid artery stenosis: a comparative study of lacidipine and hydrochlorothiazide. Blood Press 9:34–39
Skoog I (1998) Status of risk factors for vascular dementia. Neuroepidemiology 17:2–9
Sztriha LK, Nemeth D, Sefcsik T, Vecsei L (2009) Carotid stenosis and the cognitive function. J Neurol Sci 283:36–40
Ucles P, Almarcegui C, Lorente S, Romero F, Marco M (1997) Evaluation of cerebral function after carotid endarterectomy. J Clin Neurophysiol 14:242–249
Weiner MF (1996) Diagnosis of dementia. In: Weiner MF (ed) The dementias: diagnosis, management and research. American Psychiatric Press, Inc., Washington, pp 1–42
Author information
Authors and Affiliations
Corresponding author
Additional information
Piero Amodio and Paolo Pauletto Joint Seniorship
Appendix
Appendix
Methods
Details about spectral analysis
The interval of the EEG analysed had length of 60 s, subdivided in 30 epochs of 2 s, Each epoch, below denoted by {x(n)}n = 0,1, …M-1, results in a number of samples equal to M = 512 when the sampling frequency Fs is equal to 256 Hz. Spectral estimation was performed by using: the periodogram method, numerically implemented by FFT. For each subject, the final spectral estimate was obtained by averaging 30 spectra, each estimated from a 2 s epoch. Inorder to estimate the spectrum by the periodogram method the DFT {X(k)}k = 0, …M-1 of each epoch {x(n)}n = 1, …M-1
is first computed by employing a FFT algorithm. Then, the spectrum is obtained as
the first M/ 2 samples of which represent (under certain mild assumptions concerning the bandwidth of the original analog signal and the sampling frequency) samples of the spectrum at frequency points equally-spaced between 0 and Fs/2.
The Mean Dominant Frequency MDF, representing the barycentre of the spectrum, results from the following
Relative Power on four bands, representing the energy of the signal in the frequency range defined by the band :
where fmax = 25.5 Hz, fl = 1 Hz fh = 4 Hz for the delta band; fl = 4 Hz fh = 8 Hz for the theta band; fl = 8 Hz fh = 13 Hz for the alpha band and fl = 13 Hz fh = 17 for the beta 1 band, and fl = 17 Hz fh = 25.5 Hz for the beta 2 band.
Rights and permissions
About this article

Cite this article
Valenti, P., Ortelli, P., Zanon, A. et al. Psychometric and EEG changes after carotid endarterectomy. Metab Brain Dis 30, 99–105 (2015). https://doi.org/10.1007/s11011-014-9589-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11011-014-9589-1