
Abstract
Background
Catheter ablation procedures for atrial fibrillation (AF) often involve circumferential pulmonary vein isolation (PVI). Lack of reliable identification of conduction gaps along the ablation line necessitates additional ablation within previous lesion sets. We conducted a retrospective comparative study to determine the best PVI strategy for prevention of PV reconnections.
Methods and results
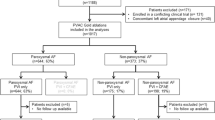
We compared the outcomes of PVI performed in two groups of patients with AF: those in whom a three-dimensional mapping system and irrigated tip radiofrequency catheter were used to electrically isolate the ipsilateral PVs (31 patients, electrical isolation group) and those in whom “pace and ablate” was performed in the PV antra until pacing at 10 mA and 2 ms no longer captured the atrial myocardium along the ablation line (31 patients, pace and ablate group). A bolus administration of 30 mg of adenosine triphosphate (ATP) revealed dormant PV reconnections more frequently in the electrical isolation group than in the pace and ablate group (28 [90 %] of 31 patients vs. 16 [52 %] of 31 patients, p = 0.0005). After re-isolation of the sites of dormant PV conduction, the post-ablation recurrence rates at 1 year were similar (26 vs. 26 %, p = 1.000).
Conclusion
Electrical PVI can usually be achieved without complete circumferential ablation. However, the isolated PVs often show dormant conduction. These findings support the hypothesis that reversible tissue injury contributes to PVI that may be acute but not necessarily durable. Similar outcomes between the two ablation strategies suggest that ATP provocation tests remain necessary to unmask dormant PV conduction.


Similar content being viewed by others


References
Ouyang, F., Bänsch, D., Ernst, S., Schaumann, A., Hachiya, H., Chen, M., et al. (2004). Complete isolation of left atrium surrounding the pulmonary veins: new insights from the double-Lasso technique in paroxysmal atrial fibrillation. Circulation, 110, 2090–2096.
Lee, G., Sanders, P., & Kalman, J. M. (2012). Catheter ablation of atrial arrhythmias: state of the art. Lancet, 380, 1509–1519.
Gerstenfeld, E. P., Callans, D. J., Dixit, S., Zado, E., & Marchlinski, F. E. (2003). Incidence and location of focal atrial fibrillation triggers in patients undergoing repeat pulmonary vein isolation: implications for ablation strategies. Journal of Cardiovascular Electrophysiology, 14, 685–690.
Ouyang, F., Antz, M., Ernst, S., Hachiya, H., Mavrakis, H., Deger, F. T., et al. (2005). Recovered pulmonary vein conduction as a dominant factor for recurrent atrial tachyarrhythmias after complete circular isolation of the pulmonary veins: lessons from double Lasso technique. Circulation, 111, 127–135.
Arentz, T., Macle, L., Kalusche, D., Hocini, M., Jais, P., Shah, D., et al. (2004). “Dormant” pulmonary vein conduction revealed by adenosine after ostial radiofrequency catheter ablation. Journal of Cardiovascular Electrophysiology, 15, 1041–1047.
Matsuo, S., Yamane, T., Date, T., Inada, K., Kanzaki, Y., Tokuda, M., et al. (2007). Reduction of AF recurrence after pulmonary vein isolation by eliminating ATP-induced transient venous re-conduction. Journal of Cardiovascular Electrophysiology, 18, 704–708.
Kumagai, K., Naito, S., Nakamura, K., Hayashi, T., Fukazawa, R., Sato, C., et al. (2010). ATP-induced dormant pulmonary veins originating from the carina region after circumferential pulmonary vein isolation of atrial fibrillation. Journal of Cardiovascular Electrophysiology, 21, 494–500.
Yamane, T., Matsuo, S., Date, T., Lellouche, N., Hioki, M., Narui, R., et al. (2011). Repeated provocation of time- and ATP-induced early pulmonary vein reconnections after pulmonary vein isolation: eliminating paroxysmal atrial fibrillation in a single procedure. Circulation: Arrhythmia and Electrophysiology, 4, 601–608.
Okumura, Y., Watanabe, I., Kofune, M., Nagashima, K., Sonoda, K., Mano, H., et al. (2013). Effect of catheter tip-tissue surface contact on three-dimensional left atrial and pulmonary vein geometries: potential anatomic distortion of 3D ultrasound, fast anatomical mapping, and merged 3D CT-derived images. Journal of Cardiovascular Electrophysiology, 24, 259–266.
Datino, T., Macle, L., Qi, X. Y., Maguy, A., Comtois, P., Chartier, D., et al. (2010). Mechanisms by which adenosine restores conduction in dormant canine pulmonary veins. Circulation, 121, 963–972.
European Heart Rhythm Association (EHRA), European Cardiac Arrhythmia Society (ECAS), American College of Cardiology (ACC), American Heart Association (AHA), Society of Thoracic Surgeons (STS), Calkins, H., et al. (2007). HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. Heart Rhythm, 4, 816–861.
Steven, D., Reddy, V. Y., Inada, K., Roberts-Thomson, K. C., Seiler, J., Stevenson, W. G., et al. (2010). Loss of pace capture on the ablation line: a new marker for complete radiofrequency lesions to achieve pulmonary vein isolation. Heart Rhythm, 7, 323–330.
Steven, D., Sultan, A., Reddy, V., Luker, J., Altenburg, M., Hoffmann, B., et al. (2013). Benefit of pulmonary vein isolation guided by loss of pace capture on the ablation line: results from a prospective 2-center randomized trial. Journal of the American College of Cardiology, 62, 44–50.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Okumura, Y., Watanabe, I., Nagashima, K. et al. The effects of standard electrical PV isolation vs. “pace and ablate” on ATP-provoked PV reconnections. J Interv Card Electrophysiol 40, 39–45 (2014). https://doi.org/10.1007/s10840-013-9869-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-013-9869-4