
Abstract
Background
Implantable cardioverter defibrillators (ICDs) have become an important part of the management of patients with congestive heart failure. At the time of ICD implantation, ventricular fibrillation (VF) is induced to assess adequate energy required for defibrillation. There are multiple parameters which influence the defibrillation safety margin (DSM); however, these factors are not well-established when ICDs are implanted for the primary prevention of sudden cardiac death (SCD) in patients with severe systolic dysfunction. We evaluated multiple clinical and echocardiographic parameters as predictors of adequate DSM in patients referred for ICD implantation for the primary prevention of SCD.
Methods
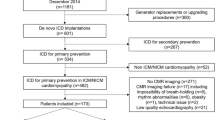
We prospectively enrolled 41 patients for ICD implantation with clinical indications for the primary prevention of SCD. Two blinded independent readers evaluated the prespecified echocardiographic parameters. These included left ventricular (LV) mass, indices of right ventricular and LV systolic and diastolic functions, and LV geometric dimensions. Basic clinical demographics, including age, gender, comorbidities, and etiology of cardiomyopathy, were also evaluated. DSM was established using our standard protocol for defibrillation testing which includes VF with successful first shock terminating VF at a value at least 10 J below the maximum output of the implanted device. High defibrillation thresholds (DFT) were defined as >21 J.
Results
The mean age is 61.8 ± 14.7 years, with men comprising the majority of the patients (73 %). The only clinical variables which predicted the high DFT were age (in years) (54.5 ± 17.5 vs. 65.7 ± 11.3, p = 0.044), QRS duration (in milliseconds) (116.0 ± 29.5 vs. 110.5 ± 21.8, p = 0.03), LV mass (in grams) (241.0 ± 77.9 vs. 181.9 ± 52.3, p = 0.006), and LV mass index (in grams per square meter) (111.1 ± 38.2 vs. 86.4 ± 21.1, p = 0.02). On multivariate logistic regression analysis, LV mass was the only independent predictor of low DFT (≤22 J) in patients with ICD implanted for the primary prevention of SCD.
Conclusion
LV mass may help predict an adequate DSM in patients who are referred for ICD implantation for the primary prevention of SCD. These results may help distinguish the patients who may require high-energy devices prior to the implantation procedure. These results may help distinguish patients requiring high-energy devices, coils, or advanced programming prior to implantation and appropriate referral to electrophysiologists.




Similar content being viewed by others


References
Epstein, A. E., DiMarco, J. P., Ellenbogen, K. A., Estes, N. A., 3rd, Freedman, R. A., Gettes, L. S., Gillinov, A. M., Gregoratos, G., Hammill, S. C., Hayes, D. L., Hlatky, M. A., Newby, L. K., Page, R. L., Schoenfeld, M. H., Silka, M. J., Stevenson, L. W., Sweeney, M. O., Smith, S. C., Jr., Jacobs, A. K., Adams, C. D., Anderson, J. L., Buller, C. E., Creager, M. A., Ettinger, S. M., Faxon, D. P., Halperin, J. L., Hiratzka, L. F., Hunt, S. A., Krumholz, H. M., Kushner, F. G., Lytle, B. W., Nishimura, R. A., Ornato, J. P., Page, R. L., Riegel, B., Tarkington, L. G., & Yancy, C. W. (2008). ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Journal of the American College of Cardiology, 51, e1–e62.
Mark, D. B., Nelson, C. L., Anstrom, K. J., Al-Khatib, S. M., Tsiatis, A. A., Cowper, P. A., Clapp-Channing, N. E., Davidson-Ray, L., Poole, J. E., Johnson, G., Anderson, J., Lee, K. L., & Bardy, G. H. (2006). Cost-effectiveness of defibrillator therapy or amiodarone in chronic stable heart failure: Results from the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT). Circulation, 114, 135–142.
Curtis, A. B., Ellenbogen, K. A., Hammill, S. C., Hayes, D. L., Reynolds, D. W., Wilber, D. J., & Cain, M. E. (2004). Clinical competency statement: Training pathways for implantation of cardioverter defibrillators and cardiac resynchronization devices. Heart Rhythm, 3, 371–375.
Gerstenfeld, E. P. (2005). Defibrillation threshold testing: Is one shock enough? Heart Rhythm, 2, 123–124.
Birnie, D., Tung, S., Simpson, C., Crystal, E., Exner, D., Ayala Paredes, F. A., Krahn, A., Parkash, R., Khaykin, Y., Philippon, F., Guerra, P., Kimber, S., Cameron, D., & Healey, J. S. (2008). Complications associated with defibrillation threshold testing: The Canadian experience. Heart Rhythm, 5, 387–390.
Marchlinski, F. E., Flores, B., Miller, J. M., Gottlieb, C. D., & Hargrove, W. C., 3rd. (1988). Relation of the intraoperative defibrillation threshold to successful postoperative defibrillation with an automatic implantable cardioverter defibrillator. The American Journal of Cardiology, 62, 393–398.
Russo, A. M., Sauer, W., Gerstenfeld, E. P., Hsia, H. H., Lin, D., Cooper, J. M., Dixit, S., Verdino, R. J., Nayak, H. M., Callans, D. J., Patel, V., & Marchlinski, F. E. (2005). Defibrillation threshold testing: Is it really necessary at the time of implantable cardioverter-defibrillator insertion? Heart Rhythm, 2, 456–461.
Mainigi, S. K., Cooper, J. M., Russo, A. M., Nayak, H. M., Lin, D., Dixit, S., Gerstenfeld, E. P., Hsia, H. H., Callans, D. J., Marchlinski, F. E., & Verdino, R. J. (2006). Elevated defibrillation thresholds in patients undergoing biventricular defibrillator implantation: Incidence and predictors. Heart Rhythm, 3, 1010–1016.
Raitt, M. H., Johnson, G., Dolack, G. L., Poole, J. E., Kudenchuk, P. J., & Bardy, G. H. (1995). Clinical predictors of the defibrillation threshold with the unipolar implantable defibrillation system. Journal of the American College of Cardiology, 25, 1576–1583.
Kopp, D. E., Blakeman, B. P., Kall, J. G., Olshansky, B., Kinder, C. A., & Wilber, D. J. (1995). Predictors of defibrillation energy requirements with nonepicardial lead systems. Pacing and Clinical Electrophysiology, 18, 253–260.
Burke, P. T., Ghanbari, H., Alexander, P. B., Shaw, M. K., Daccarett, M., & Machado, C. (2010). A protocol for patients with cardiovascular implantable devices undergoing magnetic resonance imaging (MRI): Should defibrillation threshold testing be performed post-(MRI). Journal of Interventional Cardiac Electrophysiology, 28, 59–66.
Lang, R. M., Bierig, M., Devereux, R. B., Flachskampf, F. A., Foster, E., Pellikka, P. A., Picard, M. H., Roman, M. J., Seward, J., Shanewise, J. S., Solomon, S. D., Spencer, K. T., Sutton, M. S., & Stewart, W. J. (2005). Recommendations for chamber quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. Journal of the American Society of Echocardiography, 18, 1440–1463.
Uyguanco, E. R., Berger, A., Budzikowski, A. S., Gunsburg, M., & Kassotis, J. (2008). Management of high defibrillation threshold. Expert Rev Cadiovasc Ther, 6, 1237–1248.
Chen, P. S., Wolf, P. D., & Ideker, R. E. (1991). Mechanism of cardiac defibrillation: A different point of view. Circulation, 84, 913–919.
Rodriguez, B., Eason, J. C., & Trayanova, N. A. (2006). Differences between left and right ventricular anatomy determine the type of reentrant circuits induced by an external electric shock. A rabbit heart simulation study. Progress in Biophysics and Molecular Biology, 90, 399–413.
Chapman, P. D., Sagar, K. B., Wetherbee, J. N., & Troup, P. J. (1987). Relationship of left ventricular mass to defibrillation threshold for the implantable defibrillator: A combined clinical and animal study. American Heart Journal, 114, 274–278.
Hodgson, D. M., Olsovsky, M. R., Shorofsky, S. R., Daly, B., & Gold, M. R. (2002). Clinical predictors of defibrillation thresholds with an active pectoral pulse generator lead system. PACE, 25, 408–413.
Horton, R. P., Canby, R. C., Roman, C. A., Hull, M. L., Kaye, S. A., Jessen, M. E., & Page, R. L. (1997). Determinants of nonthoracotomy biphasic defibrillation. PACE, 20, 60–64.
Lubinski, A., Lewicka-Nowak, E., Zienciuk, A., Krolak, T., Kempa, M., Pazdyga, A., & Swiatecka, G. (2005). Clinical predictors of defibrillation threshold in patients with implantable cardioverter-defibrillators. Kardiologia Polska, 62, 317–328.
Schuger, C., Ellenbogen, K. A., Faddis, M., Knight, B. P., Yong, P., & Sample, R. (2006). Defibrillation energy requirements in an ICD population receiving cardiac resynchronization therapy. Journal of Cardiovascular Electrophysiology, 17, 247–250.
Kolb, C., Tzeis, S., & Zrenner, B. (2009). Defibrillation threshold testing: Tradition or necessity? Pacing and Clinical Electrophysiology, 32, 570–572.
Strickberger, S. A., & Klein, G. J. (2004). Is defibrillation testing required for defibrillator implantation? Journal of the American College of Cardiology, 44, 88–91.
Acknowledgments
Funding was provided by the Research Department at St. John Providence Hospital, Southfield, MI, USA.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jain, S.K.A., Ghanbari, H., Hourani, R. et al. Echocardiographic parameters to predict inadequate defibrillation safety margin in patients receiving implantable cardioverter defibrillators for primary prevention. J Interv Card Electrophysiol 37, 79–85 (2013). https://doi.org/10.1007/s10840-012-9764-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-012-9764-4