
Abstract
COVID-19 outbreak has had multidimensional effects on human lives. The impacts are expected to be more severe on poor households, especially in resource-constraint economies such as Ghana. The Country has a higher poverty rate [24.2%] and this is likely to upsurge in the coming years due to this pandemic. We aimed to document the pandemic-related health and socioeconomic hazards in Ghana.
A content analysis of relevant literature, and a qualitative survey using a socioecological lens were conducted. Based on the Ghana Living Standard Survey report (GLSS 7), twenty interviewees were recruited from 3 most poverty-stricken regions in the country to verify the findings of the content review. The findings indicate a significant health burden and a large-scale socioeconomic negative outcome among the Ghanaian poor households. The disproportionate health access by the poor and the rural inhabitants has and will continue to exacerbate. The social hazards are mainly circumscribed relating to poor economic conditions due to job losses, lack of access to income/savings, food insecurity, and lack of welfare support. At the national level, the economy is particularly vulnerable due to low levels of economic diversification. The ultimate manifestation of the pandemic impacts are higher risk of morbidity and mortality rates, and deteriorating wellbeing and livelihoods. These highlights are beneficial to policymakers, development partners, and human rights advocates to make collaborative efforts in helping the poor households during and the post-pandemic periods.
Similar content being viewed by others


Introduction
The outbreak of the novel coronavirus (COVID-19) has brought about dire consequences to lives and livelihoods. These impacts are disproportionately distributed across geographical locations and the sociodemographic strata, with the poor, the older adults and rural residents being the most affected (Asante & Mills, 2020; Gyasi, 2020; Hammiduzzaman & Islam, 2020). After the early detection of coronavirus disease in Wuhan, it took 67 days for the virus to spread to 100,000 people, 11 days for this figure to double, and just 4 days for additional 100,000 cases to be recorded (WHO, 2020a, 2020b).
The steady spread of the virus and its ravaging impacts around the world continue to put fear, panic, and anxiety in people (Ahorsu et al., 2020). This phenomenon has required governments to prioritise the management of this health crisis to ensure public safety. Again, several economic recovery policies have been initiated to salvage the ailing economies. Thus, several strategies have been adopted across societies in responding to the spread of COVID-19. Central of most of these strategies is to safeguard public health as well as mitigating the adverse economic impact (Deloitte, 2020). Typical among the COVID-19 containment measures are lockdowns, contact tracing, isolations, quarantine, social distancing, and border closures.
Like many other countries, Ghana has almost adopted all the aforementioned COVID-19 restraint measures in the fight against the disease. Considered one of the fastest developing countries in West Africa with about 56.1% of her 30 million population crowded in major metropolitan cities, the government imposed a partial lockdown on major urban areas on March 30, 2020 (Gyasi, 2020). Residents in urban areas were advised to remain at home while strict social distancing protocols were introduced nationwide (Amewu et al., 2020). By April, 2020, all schools and universities had been closed and all shops and businesses, with the exception of a few (pharmacy services, hospitals, grocery shops) classified under essential services and commodity providers were still in operation under strict guidelines (Asante & Mills, 2020; Shammi et al., 2020). To ensure compliance, the government deployed the security forces (e.g., the army, police forces) to safeguard the social distancing and the other COVID-19 mitigating mechanisms. Moreover, border restrictive measures such as suspension of all visas on-arrival were implemented (Asante & Mills, 2020, Sibiri, Zankawah, and Prah, 2020).
While necessary, these decisions have led to a plethora of health, social and economic impacts on the public. For instance, the three weeks lockdown of the economically vibrant metropolitan centres, and the nationwide social distancing imposition without adequate social support packages has brought about significant adverse effects on low-income earners with poor living conditions (Addo, 2020; Asante & Mills, 2020). In several instances, these restrictions have disproportionately increased inequality by taking a greater toll on the already underprivileged or lower socio-economic groups (Gyasi, 2020). Surprisingly, there is limited data on the impact of COVID-19 on poor households in Ghana. Importantly, the available studies (e.g., Addo, 2020; Amewu et al., 2020; Asante & Mills, 2020; Gyasi, 2020) have primarily relied on secondary data (media reports, WHO reports, national COVID-19 reports) to draw conclusions. However, these data sources do not capture the unique experiences of the very poor in rural settings. At best, these datasets reflects the general national situation.
Against this backdrop, through thematic interviews, we analyse the socioeconomic crisis and health impacts of the COVID-19 pandemic in resource-limited economy, Ghana. This paper seeks to understand how the pandemic has affected the low-income and daily wage earners from the perspective of this population.
Literature review
At present, 24.2% of Ghanaians are living in poverty with 8.2% of the poor population considered as extremely poor (Cooke, Hague and McKay, 2016). The poverty rate and the proportion of extreme poor are higher in rural agricultural communities than in urban centres. The proportion of employed population below $1.90 purchasing power parity a day is 13%, while unemployment rate remains 4.33% (Cooke, Hague and McKay, 2016; GSS, 2018). Health care access and health outcomes in the country have always mirrored the socioeconomic divide where persons with higher socioeconomic statuses tend to experience better access to health services with good health outcomes than those belonging to lower wealth quintiles (Gyasi, 2020). In 2018, Hamiduzzaman and colleagues established the association between poor living conditions due to uneven access to economic resources and poor health outcomes among the low-income households (Hamiduzzaman et al., 2018). Therefore, health care access and the corresponding health outcomes are contingent on socioeconomic and environmental factors (Marmot 2005; Adler et al., 2016; Marmot & Allen, 2014).
With the onset and accelerating spread of the coronavirus pandemic, the poorer Ghanaians remain the most susceptible to the health and socioeconomic brunt of this pandemic. The low-income earners are seen to be more prone to COVID-19 infections because they are crowded in highly dense populated slum communities in urban centres and/or similar poor environments in rural areas (Paul, Chatterjee, and Bairagi, 2020). These people have received less formal education compared with the high and middle-income earners. As a result, they have lower capacity to access and appreciate health information regarding this pandemic. With little to no savings from their previous earnings prior to the COVID-19 restrictions, they are more inclined to sidestep the pandemic protocols in search of their daily bread. Moreover, the recent reopening of the economy has placed the poor working class perilously in the jaws of the COVID-19 pandemic. The migrant workers and the vulnerable, typically engaged in head porting and truck pushing activities (Asante & Helbrecht, 2020a, 2020b) have returned to work in the same poor working and crowded conditions without any effective transmission suppression mechanisms in place.
To this end, we analyse the socioeconomic crisis and health impacts of the COVID-19 pandemic in Ghana. How the pandemic has affected the low-income and daily wage earners have been highlighted in succeeding sections. Further, we make evidence-based projections into the future (Post-COVID years) and discusses policy strategies and stimulus packages capable of absorbing both the current and looming shocks of the COVID-19 crisis.
Materials and methods
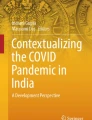
The present study adopted a two-stage technique involving a content analysis of relevant literature and qualitative interviews on health and socioeconomic impacts of the COVID-19 pandemic in Ghana. A number of published documents were extracted from various databases (such as web of science, PubMed, Google scholar, science direct), and official government and World Health organization’s websites. The articles generated from the databases and the selection procedures are presented in Fig. 1.

Flow diagram of search results and selection
Eligibility criteria
Articles were included for analysis if they met the following criteria: (1) a study reporting on the impact of COVID-19 outbreak on social and economic lives; (2) a comparative analysis of COVID-19’s impacts between rural and urban locales; (3) research undertaken to report on coping mechanisms of poor households or project COVID-19’s effects on the livelihoods of poor households in Ghana, and (4) reports on COVID-19 and health care provision and health seeking patterns. Studies were discarded if the full text was not available. If multiple accounts from the same analysis were found, the reports were either merged if they recounted different findings or secondary studies were excluded if the observations were similar to the primary result. Moreover, several relevant and possible pieces of information based on the country’s situational analysis of COVID-19’s impacts available on the print and electronic media were considered. The inductive qualitative interviews were administered to 20 participants based on an interview guide designed from critical literature review.
According Roland and colleagues (2016), in qualitative interviews, “ determination of sample size is contextual and partially dependent upon the scientific paradigm under which investigation is taking place. For example, qualitative research which is oriented towards positivism, will require larger samples than in-depth qualitative interviews”. Sandelowski (1995) suggested a sample size of 10 participants to be adequate in qualitative interviews to achieve data saturation among a homogenous population. Creswell and Miller (2000) recommends 15–30 samples in grounded theory qualitative studies to achieve data saturation. Given the greater similarities among our study participants, 20 responses were just enough for the study objective.
The final extracted documents were examined to identify major themes (Table 2) related to the current research objective. The qualitative interviews were designed to offer in-depth insights into the findings of the content analysis. However, it is worth noting that it was not the intent of this study to systematically analyse research reports on the COVID-19 pandemic in Ghana as such kind of analysis would be too early and pre-emptive because research on this domain is still at the development stage. Instead, we attempted to explore and report on the impact or experiences of the poor and the vulnerable amid the COVID-19 outbreak in Ghana. Hence, random selection of literature rather than rigorous systematic approach was employed for literature search. Again, sample selection for qualitative interviews was purposive.
Qualitative sample selection
Given the study’s focus on the impact of the pandemic on the poor households and the vulnerable population, our interviewees were mainly recruited from the three poorest regions in Ghana (Upper West, Upper East, and the Savannah regions). According to Ghana Living Standards Survey round seven (GSS, 2018; Ghana Statistical Service, 2015), poverty has several dimensions and is characterized by low income, malnutrition, ill-health, illiteracy, and insecurity, among others. The impact of the different factors could combine to keep households, and sometimes whole communities, in abject poverty (GSS, 2018; Ghana Statistical Service, 2015). In quantitative terms, 8.2% of Ghanaians, representing about 2.4 million, are extremely poor and a larger proportion of these figures are in the northern parts of the country. Specifically, the Upper west, the upper east and the Savanna regions in the north are reported to have poverty incidence rates higher than the national average (24.2%), with Upper west region having the highest. However, the Savanna Region, formerly part of the Northern region harbors the largest number of poor persons (GSS, 2018; Ghana Statistical Service, 2015).
With this backdrop, our study participants were purposively drawn from these three regions. See Table 1 for details and sample characteristics.
Selection criteria
The extant literature has shown that Ghana has higher poverty concentrations in rural localities compared to urban centres (GSS, 2018; Ghana Statistical Service, 2015). Against this evidence, rurality was a critical factor in our sampling technique with about 70% of our respondents purposively selected from rural locales. Second, monetary poverty analysis requires a baseline index to classify people into either poor or extremely poor. To this end, we employed the consumption per adult equivalent using standard Forster Greer and Thorbecke (FGT) poverty indices (GSS, 2018; Ghana Statistical Service, 2015). Like in many economies, Ghana has adopted two poverty lines; an upper limit below which a person is deemed unable to meet all their food and non-food needs, and a lower poverty line below which an individual is considered unable even to meet their food needs (Aboagye-Attah, 2019; Cooke, Hague, and McKay, 2016). The upper poverty line is set at 1314 GHS per adult per year for 2013, and households below it are simply referred to throughout this paper as living in poverty. The lower poverty line is set at 792 GHS per adult per year, and households below it are referred to throughout as living in extreme poverty (Ghana Statistical Service, 2018; Cooke, Hague, and McKay, 2016). Therefore, all participants were rated on this index through self-reporting annual income levels. Only those who met this criterion were included in the interview section. A verbal consent was sought from all the study participants.
Results
Our literature search generated 43 papers and 7 news items and official reports as shown in Fig. 1. The selection process for content analysis generated 13 documents (see Table 2). Several other news and media reports were screened in addition to these documents for the purposes of analysis. After thematic coding of the data with recourse to content analysis of the secondary data, two broad themes including health hazads and socioeconomic impacts were evident in our data (See Table 2).
Based on the themes from the content analysis, we explored the impacts of COVID-19 on poor households through in-depth interviews.
Socioeconomic impact of COVID-19
On economic impacts of COVID-19, most of the study participants mentioned loss of income (16 respondents) and job losses (12 respondents) as main challenges they were facing on the economic front. The older respondents complained about lost of family financial support in a form of remittances from abroad or local monthly mobile money transfers from relatives in urban centers. Almost all the study respondents mentioned food price increases, commodity shortages, provision of daily needs and social restrictions (inability to attend neibourhood gathering and funerals) as major social challenges. Nine (9) participants indicated incidence of marital problems due to inability to meet family needs. Increase in social vices was mentioned by 6 of the study interviewees.
Health hazards
The health challenges shared by the study respondents bordered on fear and panic, misinformation leading to feeling of hopelessness and anxiety, accessibility of health support, inadequate health facilities and infrastructural readiness, life losses, and affordability of intensive health care units (ICUs). Eighteen (18) of our respondents shared concerns about their inability to afford ICUs should any of their relatives contract the virus. About 12 participants indicated their fear of visiting health centers though, they feel the need to seek medical attention to manage their chronic conditions. Stigmatization featured prominently in the concerns shared by 7 of our respondents which according to them has led to suicide attempts. Two participants can no longer afford their routine medication due to lost of income. Almost all participants were experiencing some levels insecurity, anxiety or psychological distress.
Discussion
Each of the themes investigated in this study is explored in detail below with an illustration by a single quotation that typifies the experiences shared by our respondents. Each quotation is from a separate source, and together the quotations highlight a snapshot of the experiences of a range of poor and vulnerable populations across the study area.
Socioeconomic perspective of COVID-19 in Ghana
The findings on social and economic effects of COVID-19 on poor households largely, mirrors the national socioeconomic challenges. However, the challenges exacerbate for poor households. Ghana’s economy is primarily tied to exports of raw mineral resources and materials, bilateral loans, foreign direct investments (FDIs), and foreign remittances (Adams, Cuecuecha, and page, 2008). With almost two-thirds of the world economy experienced various form of COVID-19 restrictions, the international supply chains are disrupted, commodity prices are in turmoil, and demand is adversely affected due to industrial shutdowns (Amewu et al., 2020).
Again, the country’s high levels of indebtedness (national debt to GDP ratio 76.67% in 2020) has had a consequential effect on revenue mobilization in the international market to tackle the socioeconomic impacts of the pandemic. Remittances from migrant workers abroad have since reduced drastically, leaving dependant families, especially in rural areas to battle for sustenance (Youth Business International, 2020). As of the time of this article, the country’s nationals working abroad was hovering around 3 million, who remit their relatives either monthly or fortnightly (GSS, 2018). Travel bans as well as economic inactivity and lockdowns in host countries implies that these workers are losing out on wages. Also, prices of oil have tumbled, rendering many migrant workers in the Gulf States redundant. Over the years, oil prices have often been used to gauge inward remittances. Records available indicate a lagged effect of falling prices of crude oil on remittances into developing countries(Adams, Cuecuecha, and page, 2008). Moreover, the limited diversified nature of the economy makes it more vulnerable to pandemic shocks.
Available records indicate that the social restriction strategies, particularly the three-week lockdown, have caused a national GDP to tumble 27.9% (US$ 1.3 billion) relative to baseline GDP within the three-week referenced period (Amewu et al., 2020). During the 2020 fiscal year, the Ministry of Finance reviewed its projected GDP growth downwards from 6.8% to 1.5% (MoF 2020 as cited in Amewu et al., 2020).
The rippling effects of these shocks on the individual households and citizens are manifold. The informal sector workers comprising smallholder farmers, small scale businesses, petty traders, and daily wage earners (head porterage/ “Kayayei”, truck pushers, transport drivers and conductors, shoe menders, street hawkers) constitute more than 60% of the country’s labour force (GSS, 2018). A larger percentage of this groups have lost their income sources to the Pandemic restrictive measures. This has plunged many into a state of hopelessness and many relationships have severed. Typically, small scale entrepreneurs and market traders in Ghana rely on imported goods from neighbouring countries such as Nigeria or Asia (China, Vietnam, India) and Europe (Asante & Mills, 2020).
The disruption of the global supply chains with the ensuing shortages in supplies only not caused exponential price hikes in the local market but also, have swept away business capital of many. The price increases meant that consumers could buy fewer items or had to commit more resources for the same items. Additionally, most shop owners had to close their businesses due to poor daily sales because of the restrictive measures or inability to restock the shops (Asante &Helbrecht, 2020b). Relative to this, an interviewee had this to share:
I do not have any regular source of income. I solely rely on selling on the street to feed my family as a divorced woman. If I do not go to sell on any given day, my children will go to bed on empty stomachs. The disease (COVID-19) restrictions has almost taken our livelihood away. Even though, we are now allowed to go back and sell. But I have lost the money I was trading with to the restriction peak periods. I am being engulfed with debts now. I do not really know what lies ahead for my family
This turn of events has rendered the daily wage earners whose livelihood directly or indirectly hinges on the operations of the market traders and business entrepreneurs hopeless. For instance, the imposition of a three week lockdown in major metropolitan centres (Accra and Kumasi) meant that head porters, drivers and truck pushers were automatically out of business as their activities are mostly contingent on that of market traders and other small scale businesses. A study has reported 19.8% household income losses for the poorest and 29.8% for the wealthiest households (Sena Amewu et al., 2020). This suggests that about 3.8 million Ghanaians could be pushed into extreme financial distress. Further, most vulnerable households, such as rural farmers will remain affected way into post-COVID periods. The studies of Amewu and colleagues (2020) have reported that more than 75% of rural farm households are expected to be pushed below the poverty line due to the pandemic shocks. To this end, the World Bank and WHO have had cause to advise national leaders on the plight of the poor in this pandemic era. For example, an excerpt from the World Bank states – “the sudden and large-scale loss of low paid work has driven a mass exodus of migrant workers from cities to rural areas, spiking fear that many of them will fall back into poverty”(World Bank, 2020a; p.8).
Ghanaians largely depend on the local agricultural produce for their food staples. The pandemic restrictions have disrupted the value chain of perishable food items, leading to a production shut down in several agrarian communities. Again, the closure of agricultural input markets and the corresponding shortage of seeds, fertilizers, and weedicides is going to have a dire and long-lasting impact on upcoming planting seasons and even potential collapse of some sectors. This will only not bring about food insecurity and malnutrition but also will squeeze the life out of the poor farmers in rural areas whose livelihoods are tied to farming income. Presently, about 75% of the poor households do not have sufficient food items, 91% are financially handicapped to provide needed food and 70% are unable to offer a balanced diet for their children (Need Assessment Report, 2020). In this regard, most of the population considered vulnerable are confronted with limited livelihood options because of the disruption to the food value chain where most of these people depend for their daily or seasonal work. Shammi et al. (2020) have identified food and nutritional deficiency among the very poor due to loss of livelihood. This, together with limited access to food items, will engulf low-income households with indebtedness and negative coping mechanisms. We, therefore, submit that unless the fundamental needs of the ultra-poor are safeguarded, Ghana stands to bear higher toll on socioeconomic crisis and mental stress for many years to come.
In line with the observations thus far, there is an ongoing concern about nutrition quality as income losses and relative price hikes potentially affect fruits, vegetables, and animal-source foods. Most low-income households patronize calorie-dense foods rather than expensive and perishable vegetables because of price affordability. Clearly, the export revenue losses, redundancy in the informal sector, coupled with decreased flow of remittances, have affected the public's purchasing power in general but hitting hard on the low-income households. Therefore, the poor living conditions of this population, together with existing discrimination in accessing resources, will significantly deteriorate their health status (Hamiduzzaman et al., 2018).
Health hazards of COVID-19
Health services delivery in Ghana is done through four main categories of the health care system – the public, private-for-profit, private-not-for-profit, and traditional systems (MOH, 1997, Asewah and Abekah-Nkrumah, 2008). The Ministry of Health serves as a pivot around which the health system revolves. Administratively, it has a top-down organizational structure from the central headquarters in the national capital (Accra) to the regions, districts, and sub-districts. Services are provided via a network of facilities, with health centres and district hospitals providing primary health care services, regional hospitals providing secondary health care, and two teaching hospitals at the apex providing tertiary services (Abor, Abekah-Nkrumah, and Abor, 2008). The teaching hospitals are also charged with the responsibility of teaching and research – offering training to physicians and other health professionals and medical and public health research (Govindaraj et al., 1996; Abor, Abekah-Nkrumah, and Abor, 2008).
Over the years, Ghana's health care system has been grappling with challenges ranging from inadequate infrastructure, inadequate human resources, and inadequate medical supplies and budgetary allocations (Ofori-Atta, Read and Lund, 2010). The pandemic has further strained the health facilities to the detriment of the poor and vulnerable in the country. Also, the insufficient supply of personal protective equipment to health professionals puts physicians and nurses and other allied health workers at risk of COVID-19 contraction and cross-infections. Available report indicates that the country has lost more than five experienced medical officers who were at the forefront of the fight against the pandemic to the novel coronal virus (Ghanaian Green, 2020; Times, 2020). A survey conducted by an NGO (Needs Assessment Working group) indicated that there has been an increase strain on the health care workers and the system due to the shortage of service providers and resources. Most vulnerable communities reported insufficient information on COVID-19 symptoms and procedures to be followed. Even though, 61% of the citizens know where to contact when experiencing COVID-19 symptoms, about 45% of the population complained about inaccessibility of health facilities while 83% reported experiencing mental stress (Need Assessment Survey, 2020).
Meanwhile, the World Bank (2020a; p.8) has announced that the pandemic is yet to hit hard on low-income earners, especially the unskilled employees in the hospitality, retail trade, and transportation industries who have limited to no access to health care or social safety nets. Most of these people work under stressful and poor conditions in Ghana without any comprehensive health insurance coverage. They live in densely populated poor socioeconomic areas with limited to no literacy on personal health practices. The nature of their jobs put them in the poorest wealth quintile such that a day off from work would mean no wage bill to provide for their families. Further, some of these people ignorantly believe that they are immuned against the coronavirus because of the prevailing tropical weather condition and their dietary (local staples) consumption patterns. Hence, they are more susceptible to trading the COVID-19 protocols for their daily bread, except when they are severely sick (Hamiduzzaman et al., 2017). This has resulted to an unimaginable mental stress among this category of people who live by the daily wage bill. A 45 year old farmer stated:
Contracting coronavirus is least of my worries. Even if I do, all I need to do is to add more ginger and lemon in my diet. Akpeteshie (local gin) will kill that virus from my throat within a second after drinking it. My major concern is my farming business. These restrictions and disruptions have left me serious trauma. My BP (blood pressure) has started rising because I cannot see clear into the future
Mamum and Griffiths (2020) have reported an increasing rate of anxiety, depression, and suicides since the global outbreak of the corona pandemic. This phenomenon is caused by the COVID-19 containment measures, e.g. social isolation, quarantine, lockdowns, intimidation from COVID-19 protocol enforcers, and abusive relationships. The lack of clarity and feeling of insecurity relative to health safety, coupled with volumes of inconsistent information from the conventional and social media outlets about the pandemic, is psychologically inflicting people with fear, anger, loneliness, nervousness, helplessness, and trauma (Mamun & Ullah, 2020). Worryingly, this tense atmosphere leads to suicidal behaviours (ideation, attempts, and actual suicides), especially in low-income communities (Hamiduzzaman & Islam, 2020; Mamun &Griffits, 2020). For instance, a middle-aged man took his life in March due to a suspicion of corona infection and the social stigma anticipated from the members of his village (Somoy News, 2020). Similarly, in February, a person committed suicide in India to prevent COVID transmission (Goyal et al., 2020). Characteristic of most developing countries, poor and rural Ghanaians are less educated and have no access to mental health support services (Mamun &Griffits, 2020). Therefore, high levels of anxiety caused by information distortion and warped understanding of the spread of the disease have instigated pockets of prejudicial behaviours leading to suicidal behaviours.
Demographically, the elderly population has been identified as more prone to COVID-19 infections with higher mortality rates due to weakened immune systems (Gyasi, 2020). It is even gloomy for those living with comorbidities such as chronic respiratory diseases, diabetes, and cardiovascular ailments (Kang et al, 2020). Mortality rates of 15% and 0.2% is reported for the 80 years and above and under 20 years respectively from COVID-19 (Worldometer, 2020a). Hence, age is a critical variable posing a significant risk for COVID-19 mortality and has resulted in serious emotional and psychological distress among the Ghanaian elderly (Gyasi, 2020). Additionally, this vulnerable elderly population is being imperilled with ageism in the discourse and thoughts of the public. They are normally confronted with domestic molestations and age discrimination even in health access and utilization (Gyasi, 2020). An excerpt from a 70 year old retiree indicates:
I think they do not care that much about us (older people). They think we are dying anyways. Not even the hospitals or the policymakers show genuine concern. Listening to the media makes me feel like I would be gone in a second if I am not lucky to contract this virus. There is no hope for us. We are being emotionally and psychologically bruised every now and then.
Disturbingly, the public health system is not coordinated enough in one hand, and not well resourced on the other to deal effectively with the multidimensional COVID-19 health hazards. This deficiency has manifested in health education, monitoring, crowd controlling, and adequacy of care facilities (Hamiduzzaman & Islam, 2020; WHO, 2020b). The virus testing rate has remained low, people are defiling the masking protocol, and social gatherings are springing up without COVID transmission suppression mechanisms in place since the government reopened businesses in May. However, WHO’s (2020a, 2020b) analysis classifies 14% of total COVID cases as severe, out of which 5% normally require acute care. Over the years, government’s GDP allocations to the health sector has been woefully inadequate, just enough for procurement of primary care resources. This implies patients must make upfront payments for acute care services and facilities such as intensive care units (ICUs), specialists’ consultations, ventilators, and oxygen cylinders (Hamiduzzaman &Islam, 2020). A relatively small number of these facilities which are mostly found in cities, have the capacity to isolate coronavirus carriers and offer them with acute care and respiratory support (WHO, 2020b).
Moreover, skilled human resource is critical in the fight against this pandemic. Unfortunately, the government’s overarching attention has been on buying ventilators and other PPEs without recruitment of more health care technicians or training the existing professionals to effectively use these technologies. Again, the expensive nature of intensive care services and the out-of-pocket billing associated with their utilization effectively places acute care services out of the reach of the ultra-poor and rural communities. Therefore, people with lower socioeconomic statuses are more vulnerable to contracting and dying from the pandemic due to their living conditions and compromised health.
Like many developing countries, the impact of COVID-19 on the health and well-being of Ghanaians has been severe and not farfetched. COVID response measures implemented so far have interfered with economic activities pushing the livelihood of millions of low-income earners to a standstill. Death related to food shortages and job losses, especially among the daily wage earners, is anticipated to overtake the virus and other non-communicable diseases casualties on the mortality chart in future (Islam et al. 2020). The widespread disease with no verified vaccine or medication in sight continues to put people in fear, panic, and anxiety (Ahorsu et al. 2020). Inappropriate use of methyl alcohols, sanitizers, and disinfectants is rife among the rural communities due to lower levels of education. Besides, the fear of infection, quarantine and the stigma of social isolation has resulted in reported suicide attempts (Duan & Zhu, 2020).
Conclusion and sociological position: Way forward
In this article, we tried to highlight the health as well as the socioeconomic crisis due to the COVID-19 in Ghana. Accordingly, the unequal access to resources and opportunities in the resource-poor Ghana has been shown to have a more severe interlinkage implication on the poor and the vulnerable in the pandemic period. The poor and the vulnerable are more prone to coronavirus infections because of poor living conditions, weak immune systems due to malnutrition, lower education levels, and overcrowded nature of their slum and rural accommodations. The urban-biased establishment of COVID control centres as well as upfront payments charged for critical health services such as intensive care unit (ICU), Oxygen cylinders, and ventilators automatically make them inaccessible to the low-income earners and their families. Moreover, it has been established that, the imposition of lockdowns and social distancing mechanisms without adequate provision for the needs of the poor has led to an increase in mental problems. The feeling of helplessness, anxiety, hopelessness, and stigmatization has led a rise in suicide behaviours where a casualty has been reported. Most daily wage earners are now defiling the COVID protocols in search of daily bread, putting their lives and the gains on the pandemic fight at risk.
At the national level, the pandemic has hit hard on the key pillars of the economy which is manifested in three main avenues; first, a decline in domestic economic activities after the lockdown; second is the drop in exports of raw materials, which constitute over 80% of the country’s exports, registering an all-time fall by 83% year-on -year in April 2020 (Dzigbede & Pathak, 2020). Lastly, there has been a nosedive in remittances from Ghanaians living mostly in oil-rich Middle Eastern countries due to the pandemic and the corresponding decline in oil prices. There has been a rippling effect of the national economic downturn on the social and economic lives of the citizens. Several job losses have been recorded leading to consumption decline. Financial distress emanating from income losses without any social safety nets has severed many social relationships. Moreover, domestic violence and child abuse is on the rise and this turn of events can be attributed to psychological fallouts from the pandemic.
However, risk of community transmission, the capacity of the health system, proper biomedical waste management, social protection mechanisms, governance coordination and transparency and preparation for possible natural disasters have already been identified in similar studies (Hammiduzzaman & Islam, 2020; Shammi et al., 2020) and must be given premium attention.
Despite the government initiatives in response to this global pandemic, the analyses and expositions in this study give credence to the fact that much more needs to be done. There is an urgent need for proper coordination and strategic planning to prepare the health care system do deal effectively with any future pandemic. Social distancing has proven to be a deterrent, but lockdowns has demonstrated its corrosive impact on the national economy, leaving the poor and the vulnerable at the mercy of trauma, mental stress, hunger, anguish, and hopelessness.
Data availability statement
The data used for the analysis is embedded in the manuscript.
References
Aboagye-Attah, K. (2019). Socioeconomic correlates of poverty in Ghana using Ghana Living Standards Survey round 6 and 7 (Master’s thesis, Norwegian University of Life Sciences, Ås).
Abor, P. A., Abekah-Nkrumah, G., & Abor, J. (2008). An examination of hospital governance in Ghana. Leadership in Health Services.
Adams, R. H. Jr., Cuecuecha, A., & Page, J. (2008). The impact of remittances on poverty and inequality in Ghana. World Bank Policy Research Working Paper, (4732).
Addo, L. (2020). Of the COVID-19 in Ghana-Preparedness, Demographics and Comorbidity.
Adler, N. E., Glymour, M. M., & Fielding, J. (2016). Addressing social determinants of health and health inequalities. JAMA, 316(16), 1641–1642.
Ahorsu, D. K., Imani, V., Lin, C. Y., Timpka, T., Broström, A., Updegraff, J. A., et al. (2020). Associations -between fear of COVID-19, mental health, and preventive behaviours across pregnant women and husbands: an actor-partner interdependence modelling. International Journal of Mental Health and Addiction, 1–15.
Amewu, S., Asante, S., Pauw, K., & Thurlow, J. (2020). The economic costs of COVID-19 in sub-Saharan Africa: Insights from a simulation exercise for Ghana. The European Journal of Development Research, 32(5), 1353–1378.
Asadul Islam, Michael Vlassopoulos, Abu Siddique, Debayan Pakrashi, Md. Firoz Ahmed, Tabassum Rahman (2020) The Health and Wellbeing Impacts of COVID-19 Among Rural Households in Bangladesh and India.
Asante, L. A., & Helbrecht, I. (2020a). Urban governance and its implications for the micro-geographies of market trading in Ghana: A case of the Kotokuraba market project in cape coast. GeoJournal, 85(5), 1203–1225.
Asante, L. A., & Helbrecht, I. (2020b). Urban regeneration and politically induced displacement in a secondary African city: A case of the Kotokuraba market project, cape coast, Ghana. Geoforum, 115, 21–33.
Asante, L. A., & Mills, R. O. (2020). Exploring the Socio-Economic impact of COVID-19 Pandemic in marketplaces in Urban Ghana. Africa Spectrum, 55(2), 170–181.
Cooke, E., Hague, S., & McKay, A. (2016). The Ghana poverty and inequality report: Using the 6th Ghana living standards survey. University of Sussex.
Creswell, J. W., & Miller, D. L. (2000). Determining validity in qualitative inquiry. Theory into practice, 39(3), 124–130.
Needs Assessment Working Group. (2020). COVID-19: Bangladesh Multi-Sectorial Anticipatory impact and needs analysis. https://reliefweb.int/sites/reliefweb.int/files/resources/covid_nawg_anticipatory_impacts_and_needs_analysis.pdf.
Deloitte Access Economic (2020). The social impacts of COVID-19; Reset or restart: taking advantage of a crisis for social change. https://www2.deloitte.com/au/en/pages/economics/articles/social-impacts-of-covid-19.html.
Duan, L., & Zhu, G. (2020). Psychological interventions for people affected by the COVID-19 epidemic. The Lancet Psychiatry, 7(4), 300–302.
Dzigbede, K. D., & Pathak, R. (2020). COVID-19 economic shocks and fiscal policy options for Ghana. Journal of Public Budgeting, Accounting & Financial Management.
Ghana Health Service. (2020). Situation update confirmed Covid-19 cases in Ghana as at 25 April 2020, 22:00hrs. COVID-19: Ghana’s outbreak response management updates., Ghana Health Service and Ministry of Health. https://ghanahealthservice.org/covid19/.
Ghana Statistical Service. (2015). Ghana poverty mapping report.
Ghana Statistical Service. (2018). Ghana Living Standards Survey Round 7 (GLSS 7), Poverty trends in Ghana 2005–2017.
Govindaraj, R., Obuobi, A. A. D., Enyimayew, N. K. A., Antwi, P., & Ofosu-Amaah, S. (1996). Hospital autonomy in Ghana: the experience of Korle Bu and Komfo Anokye Teaching hospitals. Boston, MA.
Goyal, K., Chauhan, P., Chhikara, K., Gupta, P., & Singh, M. P. (2020). Fear of COVID 2019: First suicidal case in India. Asian Journal of Psychiatry, 49, e101989.
Green, A. (2020). A tribute to some of the doctors who died from COVID-19. The Lancet, 396(10264), 1720–1729.
GSS (Ghana Statistical Service). (2018). Ghana Living Standards Survey Round 6 (GLSS 6): Poverty Trends in Ghana 2005–2017.
Gyasi, R. M. (2020). Fighting COVID-19: Fear and internal conflict among older adults in Ghana. Journal of Gerontological Social Work, 63(6–7), 688–690.
Hamiduzzaman, M. (2018). The world is not mine: Factors and issues of rural elderly women’s access to modern healthcare services in Bangladesh (Doctoral dissertation). Flinders University.
Hamiduzzaman, M., De Bellis, A., Abigail, W., & Kalaitzidis, E. (2017). The social determinants of healthcare access for rural elderly women-a systematic review of quantitative studies. The Open Public Health Journal, 10(1).
Hamiduzzaman, M., De Bellis, A., Abigail, W., & Kalaitzidis, E. (2018). Elderly women in rural Bangladesh: Healthcare access and ageing trends. South Asia Research, 38(2), 113–129.
Hamiduzzaman, M., & Islam, M. R. (2020). Save life or livelihood: Responses to COVID-19 among South-Asian poor communities. Local Development & Society, 1–13.
Hamiduzzaman, M., De Bellis, A., Abigail, W., & Kalaitzidis, E. (2018). Social determinants of rural elderly women’s healthcare access: A systematic review of qualitative literature. The Indian Journal of Social Work, 79(4), 469–496.
Haque, A. (2020). The COVID-19 pandemic and the public health challenges in Bangladesh: a commentary. Journal of Health Research., 34, 563.
Islam, M. S., Ferdous, M. Z., & Potenza, M. N. (2020). Panic and generalized anxiety during the COVID-19 pandemic among Bangladeshi people: An online pilot survey early in the outbreak. Journal of affective disorders, 276, 30–37.
Kang, C., Yang, S., Yuan, J., Xu, L., Zhao, X., & Yang, J. (2020). Patients with chronic illness urgently need integrated physical and psychological care during the COVID-19 outbreak. Asian Journal of Psychiatry, 51, 102081. https://doi.org/10.1016/j.ajp.2020.102081.
Mamun, M. A., & Griffiths, M. D. (2020). First COVID-19 suicide case in Bangladesh due to fear of COVID-19 and xenophobia: Possible suicide prevention strategies. Asian Journal of Psychiatry, 51, 102073.
Mamun, M. A., & Ullah, I. (2020). COVID-19 suicides in Pakistan, dying off not COVID-19 fear but poverty? The forthcoming economic challenges for a developing country. Brain, Behavior, and Immunity, 87, 163–166.
Marmot, M. (2005). Social determinants of health inequalities. The Lancet, 365(9464), 1099–1104.
Marmot, M., & Allen, J. J. (2014). Social determinants of health equity.
Somoy News. (2020). Youth suicide in Gaibandha due to doubt of corona. Retrieved from https://m.somoynews.tv/pages/details/204558.
Ofori-Atta, A., Read, U. M., & Lund, C. (2010). A situation analysis of mental health services and legislation in Ghana: challenges for transformation. African Journal of Psychiatry, 13(2).
Paul, A., Chatterjee, S., & Bairagi, N. (2020). Prediction on Covid-19 epidemic for different countries: Focusing on South Asia under various precautionary measures. medRxiv. doi:10.1101/ 2020.04.08.20055095.
Rapid Assessment Findings on COVID 19 Effects on Urban Health (2020) https://reliefweb.int/sites/reliefweb.int/files/resources/Rapid-Assessment-Report-on-COVID-19-effects-on-Urban-Health.pdf [Accessed 24 September, 2020].
Roland, N., Frenay, M., & Boudrenghien, G. (2016). Towards a better understanding of academic persistence among fresh-men: A Qualitative approach. Journal of Education and Training Studies, 4(12), 175-188
Sandelowski, M. (1995). Sample size in qualitative research. Research in nursing & health, 18(2), 179–183.
Shammi, M., Bodrud-Doza, M., Islam, A. R. M. T., & Rahman, M. M. (2020). COVID-19 pandemic, socioeconomic crisis and human stress in resource-limited settings: A case from Bangladesh. Heliyon, 6, e04063.
Sibiri, H., Zankawah, S. M., & Prah, D. (2020). Coronavirus diseases 2019 (COVID-19) response: Highlights of Ghana’s scientific and technological innovativeness and breakthroughs. Ethics, Medicine and Public Health, 14, 100537.
Ghanaian Times (2020). Ghana: 4 Medical Officers Die of COVID-19 ... More Than150 Battling for Their Lives https://allafrica.com/stories/202007060840.html.
WHO. (2020a). Coronavirus disease 2019 (COVID-19) situation report – 51. World Health Organisation.
WHO, (2020b). WHO bulletin novel coronavirus (2019-NCoV) situation report – 22. World Health Organisation, Geneva. Retrieved from https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200211-sitrep-22-ncov.pdf?sfvrsn=fb6d49b1_2.
World Bank (2020b, June 02). HealthStats. Washington. Retrieved from https://data.worldbank.org/topic/health.
World Health Organization [WHO]. Coronavirus disease (COVID-19): Situation report - 168. [updated 2020 July 6; cited 2020 July 12]. Available at: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200706-covid-19-sitrep-168.pdf?sfvrsn57fed5c0b_2.
Worldometer. (2020a). Age, sex, existing conditions of COVID-19 cases and deaths. The World Health Organization, Geneva. Retrieved April, 25, 2020, from https://www.worldometers.info/coronavirus/coronavirus-age-sex-demographics/.
Worldometer. (2020b). Countries where COVID-19 has spread. The World Health Organization, Geneva. Retrieved April, 25, 2020, from https://www.worldometers.info/coronavirus/countries-where-coronavirus-has-spread/.
Youth Business International. (2020). Supporting small businesses to ensure the future of Ghana https://www.youthbusiness.org/resource/supporting-small-businesses-ghana-mahadhe-hasan-interview.
Zabir, A. A., Mahmud, A., Islam, M. A., Antor, S. C., Yasmin, F., & Dasgupta, A. (2020). COVID-19 and food supply in Bangladesh: A review. Available at SSRN 3595967.
Funding
This study did not receive any funding.
Author information
Authors and Affiliations
Contributions
DA: writing, original draft preparation; investigation; writing, review and editing; conceptualization; methodology; software; and formal analysis. MAT: supervision, writing—review and editing. ASKS: data gathering; formal analysis; review and editing. SG: investigation; writing, review and editing; conceptualization. AB: investigation; writing, review and editing; conceptualization.
Corresponding author
Ethics declarations
Conflict of interest
Authors declare no known conflict of interests.
Ethical approval
This study did not require ethics review.
Consent for participant
Verbal Consent was sought from all participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Asante, D., Twumasi, M.A., Sakyi, A.S.K. et al. A socio-geographic perspective of health and economic impacts of COVID-19 on poor households in ghana. GeoJournal 87, 4113–4125 (2022). https://doi.org/10.1007/s10708-021-10487-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10708-021-10487-2