
Abstract
Background
The complete removal of adenomatous polyps is important for reducing interval cancer after colonoscopy.
Aims
To identify factors affecting the completeness of colonoscopic polypectomies and to evaluate the experience level of fellows who achieve competence compared with that of experts.
Methods
Medical records of 1,860 patients who underwent at least one polypectomy for an adenomatous polyp at Seoul National University Hospital between March 2011 and February 2013 were retrospectively reviewed. A total of 3,469 adenomatous polyps were included. The lateral and deep margins of the resected polyps were evaluated to check the resection completeness.
Results
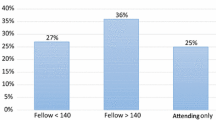
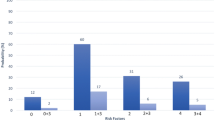
Of the 3,469 adenomatous polyps, 1,389 (40.0 %) were removed by two experts and 2,080 (60.0 %) were removed by seven fellows. In the expert-treated group, larger size [odds ratio (OR) 2.81 for ≥20 mm, 95 % confidence interval (CI) 1.64–4.84, P < 0.001] and right-sided location (OR 1.31, 95 % CI 1.05–1.63, P = 0.019) were associated with incomplete resection. In the fellow-treated group, not only polyp characteristics [right-sided location (OR 1.41, 95 % CI 1.18–1.69, P < 0.001)], but also the cumulative number of procedures was also related to resection completeness. After 300 polypectomies, the complete resection rate of the fellows was comparable to that of the experts.
Conclusions
In the fellow-treated group, the level of procedure experience was closely associated with the polypectomy outcomes. Meticulous attention is critical to ensure the completeness of polypectomies performed by trainee endoscopists during the training program.



Similar content being viewed by others

References
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29.
Park HC, Shin A, Kim BW, et al. Data on the characteristics and the survival of korean patients with colorectal cancer from the Korea central cancer registry. Ann Coloproctol. 2013;29:144–149.
Gupta AK, Melton LJ 3rd, Petersen GM, et al. Changing trends in the incidence, stage, survival, and screen-detection of colorectal cancer: a population-based study. Clin Gastroenterol Hepatol. 2005;3:150–158.
Burt RW. Colon cancer screening. Gastroenterology. 2000;119:837–853.
Zauber AG, Winawer SJ, O’Brien MJ, et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med. 2012;366:687–696.
Farrar WD, Sawhney MS, Nelson DB, Lederle FA, Bond JH. Colorectal cancers found after a complete colonoscopy. Clin Gastroenterol Hepatol. 2006;4:1259–1264.
Lieberman DA, Holub J, Eisen G, Kraemer D, Morris CD. Utilization of colonoscopy in the United States: results from a national consortium. Gastrointest Endosc. 2005;62:875–883.
Pohl H, Srivastava A, Bensen SP, et al. Incomplete polyp resection during colonoscopy-results of the complete adenoma resection (CARE) study. Gastroenterology. 2013;144:74–80.
Kahi CJ, Rex DK. Why we should CARE about polypectomy technique. Gastroenterology. 2013;144:16–18.
Kim HG, Lee SH, Jeon SR, et al. Clinical significance of the first surveillance colonoscopy after endoscopic early colorectal cancer removal. Hepatogastroenterology. 2013;60:1047–1052.
Corley DA, Jensen CD, Marks AR, et al. Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med. 2014;370:1298–1306.
Lee SH, Chung IK, Kim SJ, et al. An adequate level of training for technical competence in screening and diagnostic colonoscopy: a prospective multicenter evaluation of the learning curve. Gastrointest Endosc. 2008;67:683–689.
Spier BJ, Benson M, Pfau PR, Nelligan G, Lucey MR, Gaumnitz EA. Colonoscopy training in gastroenterology fellowships: determining competence. Gastrointest Endosc. 2010;71:319–324.
Peters SL, Hasan AG, Jacobson NB, Austin GL. Level of fellowship training increases adenoma detection rates. Clin Gastroenterol Hepatol. 2010;8:439–442.
Participants in the Paris Workshop. The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon: November 30 to December 1, 2002. Gastrointest Endosc. 2003;58:S3–43.
Kim MN, Kang JM, Yang JI, et al. Clinical features and prognosis of early colorectal cancer treated by endoscopic mucosal resection. J Gastroenterol Hepatol. 2011;26:1619–1625.
Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO Classification of Tumours of the Digestive System. 4th ed. Lyon: International Agency for Research on Cancer; 2010.
Park JJ, Cheon JH, Kwon JE, et al. Clinical outcomes and factors related to resectability and curability of EMR for early colorectal cancer. Gastrointest Endosc. 2011;74:1337–1346.
Serrano M. Mao de Ferro S, Fidalgo P, Lage P, Chaves P, Dias Pereira A. Endoscopic mucosal resection of superficial colorectal neoplasms: review of 140 procedures. Acta Med Port. 2012;25:288–296.
Quintas P, Cubiella J, Couto I, et al. Factors associated with complete endoscopic resection of an invasive adenocarcinoma in a colorectal adenoma. Rev Esp Enferm Dig. 2012;104:524–529.
Liu S, Ho SB, Krinsky ML. Quality of polyp resection during colonoscopy: are we achieving polyp clearance? Dig Dis Sci. 2012;57:1786–1791.
Woodward TA, Heckman MG, Cleveland P, De Melo S, Raimondo M, Wallace M. Predictors of complete endoscopic mucosal resection of flat and depressed gastrointestinal neoplasia of the colon. Am J Gastroenterol. 2012;107:650–654.
Training C, Sedlack RE, Shami VM, et al. Colonoscopy core curriculum. Gastrointest Endosc. 2012;76:482–490.
Metz AJ, Moss A, McLeod D, et al. A blinded comparison of the safety and efficacy of hot biopsy forceps electrocauterization and conventional snare polypectomy for diminutive colonic polypectomy in a porcine model. Gastrointest Endosc. 2013;77:484–490.
Fry LC, Lazenby AJ, Mikolaenko I, Barranco B, Rickes S, Monkemuller K. Diagnostic quality of: polyps resected by snare polypectomy: does the type of electrosurgical current used matter? Am J Gastroenterol. 2006;101:2123–2127.
Conio M, Ponchon T, Blanchi S, Filiberti R. Endoscopic mucosal resection. Am J Gastroenterol. 2006;101:653–663.
Robertson DJ, Lieberman DA, Winawer SJ, et al. Colorectal cancers soon after colonoscopy: a pooled multicohort analysis. Gut. 2014;63:949–956.
Zimmer B, Felber J, Lehmann M, Brenk-Franz K, Petersen I, Stallmach A. Impact of implementation strategies on adherence rates to colorectal cancer (CRC) guidelines after polypectomy in a university hospital. Z Gastroenterol. 2013;51:1157–1164.
Lieberman DA, Rex DK, Winawer SJ, et al. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012;143:844–857.
Parente F, Bargiggia S, Boemo C, et al. Anatomic distribution of cancers and colorectal adenomas according to age and sex and relationship between proximal and distal neoplasms in an i-FOBT-positive average-risk Italian screening cohort. Int J Colorectal Dis. 2014;29:57–64.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Ji Min Choi and Changhyun Lee have contributed equally to this work.
Rights and permissions
About this article

Cite this article
Choi, J.M., Lee, C., Park, J.H. et al. Complete Resection of Colorectal Adenomas: What Are the Important Factors in Fellow Training?. Dig Dis Sci 60, 1579–1588 (2015). https://doi.org/10.1007/s10620-014-3500-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-014-3500-0