
Summary
Background
The aim of this study is to investigate the feasibility of using indirect laryngoscopy for the diagnosis of difficult intubations in patients who are undergoing microlaryngeal surgery.
Methods
In the pre-anesthetic examination the thyromental distance, sternomental distance, interincisor distance, neck circumference, modified Mallampati scores, and Wilson risk scores were measured. An otolaryngologist conducted an indirect laryngoscopic assessment. Direct laryngoscopic profiles were classified according to their Cormack–Lehane scores.
Results
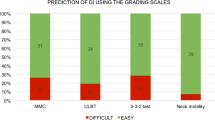
Forty patients underwent microlaryngeal surgery. Their mean ages, neck circumferences, Cormack–Lehane scores of the patients who had intubation difficulties were statistically significantly higher than those who did not have intubation difficulties (p < 0.05). The significant differences between the indirect laryngoscopic assessment distributions of patients who either had or did not have intubation difficulty were assessed (p < 0.05).
Conclusions
Indirect laryngoscopic assessment is a simple and valuable technique that can be used for the diagnosis of difficult intubation in patients who are undergoing microlaryngeal surgery.
Zusammenfassung
Grundlagen
Ziel dieser Studie war es, zu untersuchen, inwiefern die Verwendung der indirekten Laryngoskopie für die Diagnostik von schwierigen Intubationen bei Patienten, die sich einer Mikrolaryngoskopie unterziehen, geeignet ist.
Methodik
Im Laufe der voranästhetischen Untersuchung wurden die thyromentale Distanz, die sternomentale Distanz, der Schneidezahnabstand, der Genickumfang und die angepassten Mallampati-Scores sowie die Wilson-Risiko-Scores gemessen. Ein Otolaryngologe hat eine indirekte Laryngoskopie durchgeführt. Direkte laryngoskopische Profile wurden anhand ihres Cormack-Lehane-Scores eingestuft.
Ergebnisse
Vierzig Patienten haben sich einer Mikrolaryngoskopie unterzogen. Das Durchschnittsalter, der durchschnittliche Genickumfang und die Cormack-Lehane-Scores der Patienten, die Intubationsschwierigkeiten hatten, waren statistisch betrachtet erheblich höher als die der Patienten, die keine solche Schwierigkeiten hatten (p < 0,05). Die signifikanten Unterschiede zwischen den Ergebnisverteilungen der indirekten laryngoskopischen Untersuchung für Patienten, die jeweils Intubationsschwierigkeiten hatten bzw. nicht hatten, wurden ausgewertet (p < 0,05).
Schlussfolgerungen
Die indirekte laryngoskopische Untersuchung stellt ein einfaches und wertvolles Verfahren dar, das für die Diagnostik der Intubationsschwierigkeiten bei Patienten, die sich einer Mikrolaryngoskopie unterziehen, verwendet werden kann.
Similar content being viewed by others


References
Lundstrom LH, Vester-Andersen M, Møller AM, Charuluxananan S, L’hermite J, Wetterslev J, Danish Anaesthesia Database. Poor prognostic value of the modified Mallampati score: a meta-analysis involving 177 088 patients. Br J Anaesth. 2011;107(5):659–67.
Hagberg CA, Artime CA. Airway management in the adult. In: Miller RD, editor. Miller’s anesthesia. Philadelphia: Elsevier; 2015. pp. 1647–83.
Patel B, Khandekar R, Diwan R, Shah A. Validation of modified Mallampati test with addition of thyromental distance and sternomental distance to predict difficult endotracheal intubation in adults. Indian J Anaesth. 2014;58(2):171–5.
Yamamoto K, Tsubokawa T, Shibata K, Ohmura S, Nitta S, Kobayashi T. Predicting difficult intubation with indirect laryngoscopy. Anesthesiology. 1997;86(2):316–21.
Budde AO, Desciak M, Reddy V, Falcucci OA, Vaida SJ, Pott LM. The prediction of difficult intubation in obese patients using mirror indirect laryngoscopy: a prospective pilot study. J Anaesthesiol Clin Pharmacol. 2013;29(2):183–6.
Ul Haq MI, Ullah H. Comparison of Mallampati test with lower jaw protrusion maneuver in predicting difficult laryngoscopy and intubation. J Anaesthesiol Clin Pharmacol. 2013;29(3):313–7.
Brooker CR, Hunsaker DH, Zimmerman AA. A new anesthetic system for microlaryngeal surgery. Otolaryngol Head Neck Surg. 1998;118(1):55–60.
Davies JM, Hillel AD, Maronian NC, Posner KL. The Hunsaker Mon-Jet tube with jet ventilation is effective for microlaryngeal surgery. Can J Anaesth. 2009;56(4):284–90.
Winterhalter M, Kirchhoff K, Gröschel W, Lüllwitz E, Heermann R, Hoy L, et al. The laryngeal tube for difficult airway management: a prospective investigation in patients with pharyngeal and laryngeal tumours. Eur J Anaesthesiol. 2005;22(9):678–82.
Rosenblatt W, Ianus AI, Sukhupragarn W, Fickenscher A, Sasaki C. Preoperative endoscopic airway examination (PEAE) provides superior airway information and may reduce the use of unnecessary awake intubation. Anesth Analg. 2011;112(3):602–7.
Sánchez-Morillo J, Estruch-Pérez MJ, Hernández-Cádiz MJ, Tamarit-Conejeros JM, Gómez-Diago L, Richart-Aznar M. Indirect laryngoscopy with rigid 70-degree laryngoscope as a predictor of difficult direct laryngoscopy. Acta Otorrinolaringol Esp. 2012;63(4):272–9.
Zhang X, Li W. Misguidance of peroral rigid laryngoscopy in assessment of difficult airway: two comparable cases in microlaryngeal surgery. BMJ Case Rep. 2013. doi:10.1136/bcr-2012-008423.
Kayhan Z. Entübasyon güçlüğü, tanımı, nedenleri, sınıflandırılması, önceden belirlenmesi. Anestezi Dergisi. 1998;6(3):91–6.
Prakash S, Kumar A, Bhandari S, Mullick P, Singh R, Gogia AR. Difficult laryngoscopy and intubation in the Indian population: an assessment of anatomical and clinical risk factors. Indian J Anaesth. 2013;57(6):569–75.
Gonzalez H, Minville V, Delanoue K, Mazerolles M, Concina D, Fourcade O. The importance of increased neck circumference to intubation difficulties in obese patients. Anesth Analg. 2008;106(4):1132–6.
Kim WH, Ahn HJ, Lee CJ, Shin BS, Ko JS, Choi SJ, Ryu SA. Neck circumference to thyromental distance ratio: a new predictor of difficult intubation in obese patients. Br J Anaesth. 2011;106(5):743–8.
Hassani A, Kessell G. Neck circumference and difficult intubation. Anesth Analg. 2008;107(5):1756–7.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Türkay, M., Şentürk, T., Arslan, B.Y. et al. Indirect laryngoscopic assessment for the diagnosis of difficult intubation in patients undergoing microlaryngeal surgery. Wien Med Wochenschr 166, 62–67 (2016). https://doi.org/10.1007/s10354-015-0419-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10354-015-0419-9