
Abstract
Background
Improvements in operative technique and perioperative management have resulted in increasing numbers of elderly patients undergoing gastrectomy for gastric cancer (GC). We evaluated the accuracy of Estimation of Physiologic Ability and Surgical Stress (E-PASS) and modified (m)E-PASS scores in predicting postoperative complications in elderly patients with GC.
Methods
We retrospectively analyzed short-term outcomes in 413 patients who underwent gastrectomy for GC between 2005 and 2014. They were divided into two groups: Group N comprised 341 non-elderly patients <80 years of age and Group E comprised 72 elderly patients ≥80 years of age. We calculated the E-PASS and mE-PASS scores and evaluated the correlation between the comprehensive risk score (CRS) and occurrence of postoperative complications.
Results
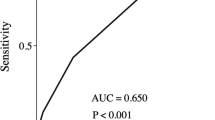
Morbidity rates were 25.5 % in Group N and 31.9 % in Group E. In Group N, the CRS values of both the E-PASS (P < 0.0001) and mE-PASS (P < 0.0001) scores were significantly higher in patients with complications than in those without complications. In Group E, although the E-PASS CRS was significantly higher in patients with complications than in patients without complications (P = 0.01), the mE-PASS CRS fixed (CRSf) score was not significantly correlated with the occurrence of postoperative complications (P = 0.08).
Conclusion
Both E-PASS and mE-PASS can be used to predict the occurrence of postoperative complications in GC patients undergoing gastrectomy. However, the E-PASS CRS is more accurate for elderly patients because variations in intraoperative parameters such as operation time, blood loss, and extent of skin incision have a strong influence on the occurrence of postoperative complications.



Similar content being viewed by others


References
Jemal A, Bray F, Center MM et al (2011) Global cancer statistics. CA Cancer J Clin 61:69–90
Saito H, Osaki T, Murakami D et al (2006) Effect of age on prognosis in patients with gastric cancer. ANZ J Surg 76:458–461
Saif MW, Makrilia N, Zalonis A et al (2010) Gastric cancer in the elderly: an overview. Eur J Surg Oncol 36:709–717
Hundahl SA, Phillips JL, Menck HR (2000) The National Cancer Data Base Report on poor survival of US gastric carcinoma patients treated with gastrectomy: fifth edition American Joint Committee on Cancer staging, proximal disease, and the “different disease” hypothesis. Cancer 88:921–932
Orsenigo E, Tomajer V, Palo SD et al (2007) Impact of age on postoperative outcomes in 1118 gastric cancer patients undergoing surgical treatment. Gastric Cancer 10:39–44
Saidi RF, Bell JL, Dudrick PS (2004) Surgical resection for gastric cancer in elderly patients: is there a difference in outcome? J Surg Res 118:15–20
Ariake K, Ueno T, Takahashi M et al (2014) E-PASS comprehensive risk score is a good predictor of postsurgical mortality from comorbid disease in elderly gastric cancer patients. J Surg Oncol 109:586–592
Copeland GP, Jones D, Walters M (1991) POSSUM: a scoring system for surgical audit. Br J Surg 78:355–360
Haga Y, Ikei S, Ogawa M (1999) Estimation of Physiologic Ability and Surgical Stress (E-PASS) as a new prediction scoring system for postoperative morbidity and mortality following elective gastrointestinal surgery. Surg Today 29:219–225
Knaus WA, Draper EA, Wagner DP et al (1985) APACHE II: a severity of disease classification system. Crit Care Med 13:818–829
Banz VM, Studer P, Inderbitzin D et al (2009) Validation of the estimation of physiologic ability and surgical stress (E-PASS) score in liver surgery. World J Surg 33:1259–1265
Hashimoto D, Takamori H, Sakamoto Y et al (2010) Is an estimation of physiologic ability and surgical stress able to predict operative morbidity after pancreaticoduodenectomy? J Hepatobiliary Pancreat Sci 17:132–138
Hashimoto D, Takamori H, Sakamoto Y et al (2010) Can the physiologic ability and surgical stress (E-PASS) scoring system predict operative morbidity after distal pancreatectomy? Surg Today 40:632–637
Yoshida N, Watanabe M, Baba Y et al (2013) Estimation of physiologic ability and surgical stress (E-PASS) can assess short-term outcome after esophagectomy for esophageal cancer. Esophagus 10:86–94
Haga Y, Ikejiri K, Wada Y et al (2011) A multicenter prospective study of surgical audit systems. Ann Surg 253:194–201
Haga Y, Wada Y, Takeuchi H et al (2012) Evaluation of modified estimation of physiologic ability and surgical stress in gastric carcinoma surgery. Gastric Cancer 15:7–14
Japanese Gastric Cancer Association (2011) Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer 14:101–112
Japanese Gastric Cancer Association (2011) Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer 14:113–123
Clavien PA, Barkun J, de Oliveira ML et al (2009) The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg 250:187–196
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Haga Y, Yagi Y, Ogawa M (1999) Less-invasive surgery for gastric cancer prolongs survival in patients over 80 years of age. Surg Today 29:842–848
Polanczyk CA, Marcantonio E, Goldman L et al (2001) Impact of age on perioperative complications and length of stay in patients undergoing noncardiac surgery. Ann Intern Med 134:637–643
Yamashita S, Haga Y, Nemoto E et al (2006) Comparison of surgical outcome using the prediction scoring system of E-PASS for thoracic surgery. Jpn J Thorac Cardiovasc Surg 54:391–395
Yamashita S, Haga Y, Nemoto E et al (2004) E-PASS (The Estimation of Physiologic Ability and Surgical Stress) scoring system helps the prediction of postoperative morbidity and mortality in thoracic surgery. Eur Surg Res 36:249–255
Tang T, Walsh SR, Fanshawe TR et al (2007) Estimation of physiologic ability and surgical stress (E-PASS) as a predictor of immediate outcome after elective abdominal aortic aneurysm surgery. Am J Surg 194:176–182
Tang TY, Walsh SR, Fanshawe TR et al (2007) Comparison of risk-scoring methods in predicting the immediate outcome after elective open abdominal aortic aneurysm surgery. Eur J Vasc Endovasc Surg 34:505–513
Hayashi T, Yoshikawa T, Aoyama T et al (2012) Severity of complications after gastrectomy in elderly patients with gastric cancer. World J Surg 36:2139–2145
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical standards
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. Informed consent or substitute for it was obtained from all patients for being included in the study.
Conflict of interest
We declare that there is no grant support and any other conflict of interest.
About this article

Cite this article
Kitano, Y., Iwatsuki, M., Kurashige, J. et al. Estimation of Physiologic Ability and Surgical Stress (E-PASS) versus modified E-PASS for prediction of postoperative complications in elderly patients who undergo gastrectomy for gastric cancer. Int J Clin Oncol 22, 80–87 (2017). https://doi.org/10.1007/s10147-016-1028-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10147-016-1028-3