
Abstract
Purpose
The selection of a laparoscopic approach for inguinal hernias varies among surgeons. It is unclear what is being done in actual practice. The purpose of this study was to report practice patterns for treatment of inguinal hernias among Quebec surgeons, and to identify factors that may be associated with the choice of operative approach.
Methods
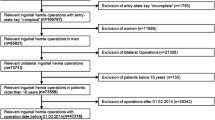
We studied a population-based cohort of patients who underwent an inguinal hernia repair between 2007 and 2011 in Quebec, Canada. A generalized linear model was used to identify predictors associated with the selection of a laparoscopic approach.
Results
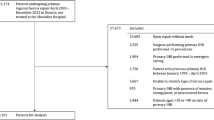
49,657 inguinal hernias were repaired by 478 surgeons. Laparoscopic inguinal hernia repair (LIHR) was used in 8 % of all cases. LIHR was used to repair 28 % of bilateral hernias, 10 % of recurrent hernias, 6 % of unilateral hernias, and 4 % of incarcerated hernias. 268 (56 %) surgeons did not perform any laparoscopic repairs, and 11 (2 %) surgeons performed more than 100 repairs. These 11 surgeons performed 61 % of all laparoscopic cases. Patient factors significantly associated with having LIHR included younger age, fewer comorbidities, bilateral hernias, and recurrent hernias.
Conclusion
An open approach is favored for all clinical scenarios, even for situations where published guidelines recommend a laparoscopic approach. Surgeons remain divided on the best technique for inguinal hernia repair: while more than half never perform LIHR, the small proportion who perform many use the technique for a large proportion of their cases. There appears to be a gap between the best practices put forth in guidelines and what surgeons are doing in actual practice. Identification of barriers to the broader uptake of LIHR may help inform the design of educational programs to train those who have the desire to offer this technique for certain cases, and have the volume to overcome the learning curve.
Similar content being viewed by others

References
Morales-Conde S, Socas M, Fingerhut A (2012) Endoscopic surgeons’ preferences for inguinal hernia repair: TEP, TAPP, or OPEN. Surg Endosc. doi:10.1007/s00464-012-2247-y
McCormack K, Wake B, Perez J, Fraser C, Cook J, McIntosh E, Vale L, Grant A (2005) Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation. Health Technol Assess 9:1–203
Mahon D, Decadt B, Rhodes M (2003) Prospective randomized trial of laparoscopic (transabdominal preperitoneal) vs open (mesh) repair for bilateral and recurrent inguinal hernia. Surg Endosc 17:1386–1390
Simons MP, Aufenacker T, Bay-Nielsen M, Bouillot JL, Campanelli G, Conze J, de Lange D, Fortelny R, Heikkinen T, Kingsnorth A, Kukleta J, Morales-Conde S, Nordin P, Schumpelick V, Smedberg S, Smietanski M, Weber G, Miserez M (2009) European Hernia Society guidelines on the treatment of inguinal hernia in adult patients. Hernia 13:343–403
Rosenberg J, Bisgaard T, Kehlet H, Wara P, Asmussen T, Juul P, Strand L, Anderson FH, Bay-Neilsen M (2011) Danish Hernia Database recommendations for the management of inguinal and femoral hernia in adults. Danish Med Bull 58:C4243
National Institute for Health and Care Excellence (2004) Technology appraisal guidance no 83: guidance on the use of laparoscopic surgery for inguinal hernia. http://www.nice.org.uk/guidance/ta83/resources/guidance-laparoscopic-surgery-for-inguinal-hernia-repair-pdf
Edwards CC 2nd, Bailey RW (2000) Laparoscopic hernia repair: the learning curve. Surg Laparosc Endosc Percutan Tech 10:149–153
Blais R (1993) Variations in surgical rates in Quebec: does access to teaching hospitals make a difference? CMAJ 148:1729–1736
Regie de l’assurance-maladie du Quebec (2004) Statistiques Annuelles. http://bibvir1.uqac.ca/archivage/1327526a2004.pdf
Charlson ME, Pompei P, Ales KL, Mackenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
Deyo RA, Cherkin DC, Ciol MA (1992) Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol 45:613–619
Quan H, Sundararajan V, Halfon P, Fong A, Burnand B, Luthi JC, Saunders LD, Beck CA, Feasby TE, Ghali WA (2005) Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care 43:1130–1139
Rosenberg J, Bay-Nielsen M (2008) Current status of laparoscopic inguinal hernia repair in Denmark. Hernia 12:583–587
Smink DS, Paquette IM, Finlayson SR (2009) Utilization of laparoscopic and open inguinal hernia repair: a population-based analysis. J Laparoendosc Adv Surg Tech A 19:745–748
Zendejas B, Ramirez T, Jones T, Kuchena A, Martinez J, Ali SM, Lohse CM, Farley DR (2012) Trends in the utilization of inguinal hernia repair techniques: a population-based study. Am J Surg 203:313–317
McCormack K, Scott NW, Go PM, Ross S, Grant AM (2003) Laparoscopic techniques versus open techniques for inguinal hernia repair. Cochrane database Syst Rev. doi:10.1002/14651858.cd001785
Statistics Canada (2011) Population and dwelling counts, for Canada, provinces and territories, 2011 and 2006 censuses. http://www12.statcan.gc.ca/census-recensement/2011/dp-pd/hlt-fst/pd-pl/Table-tableau.cfm?LANG=Eng&T=101&S=50&O=A
Trevisonno M, Kaneva P, Watanabe Y, Fried GM, Feldman LS, Lebedeva K, Vassiliou M (2014) A survey of general surgeons regarding laparoscopic inguinal hernia repair: practice patterns, barriers and educational needs. Hernia. doi:10.1007/s10029-014-1287-8
Kanonidou Z, Karystianou G (2007) Anesthesia for the elderly. Hippokratia 11:175–177
Kingsnorth A, LeBlanc K (2003) Hernias: inguinal and incisional. Lancet 362:1561–1571
Wara P, Bay-Nielsen M, Juul P, Bendix J, Kehlet H (2005) Prospective nationwide analysis of laparoscopic versus Lichtenstein repair of inguinal hernia. Br J Surg 92:1277–1281
Neumayer L, Giobbie-Hurder A, Jonasson O, Fitzgibbons R, Dunlop D, Gibbs J, Reda D, Henderson W (2004) Open mesh versus laparoscopic mesh repair of inguinal hernia. N Engl J Med 350:1819–1827
Alkhoury F, Martin JT, Contessa J, Zucherman R, Nadzam G (2010) The impact of laparoscopy on the volume of open cases in general surgery training. J Surg Educ 67:316–319
Qureshi A, Vergis A, Jimenez C, Green J, Pryor A, Schlachta CM, Okrainec A (2011) MIS training in Canada: a national survey of general surgery residents. Surg Endosc 25:3057–3065
Wilchesky M, Tamblyn RM, Huang A (2004) Validation of diagnostic codes within medical services claims. J Clin Epidemiol 57:131–141
Acknowledgments
The Steinberg-Bernstein Centre for Minimally Invasive Surgery at McGill University is supported by an unrestricted educational grant from Covidien Canada. Salary support was also provided by the Mitacs-Accelerate program for the first author.
Conflict of interest
M. Trevisonno declares conflict of interest directly related to the submitted work. Salary support was provided by an unrestricted educational grant from Covidien Canada and from the Mitacs-Accelerate program. No conflict of interest with regards to the results of this study. P. Kaneva declares conflict of interest directly related to the submitted work. Salary support was provided in part by an unrestricted educational grant from Covidien Canada. No conflict of interest with regards to the results of this study. Y. Watanabe declares conflict of interest directly related to the submitted work. Salary support was provided by an unrestricted educational grant from Covidien Canada. No conflict of interest with regards to the results of this study. G. Fried, L. Feldman, A. Andalib, M. Vassiliou declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Trevisonno, M., Kaneva, P., Watanabe, Y. et al. Current practices of laparoscopic inguinal hernia repair: a population-based analysis. Hernia 19, 725–733 (2015). https://doi.org/10.1007/s10029-015-1358-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-015-1358-5