
Abstract
Background
Hip resurfacing arthroplasty has some advantages, including improved metal-on-metal articulation, a lower dislocation rate and preserved femoral bone. This procedure is a surgical option for younger and more active patients with osteoarthritis and osteonecrosis of the femoral head. Although there have been some reports about the efficacy of this technique, others report serious complications caused by metal debris. Additionally, femoral neck preservation adversely decreases the head–neck ratio and results in postoperative impingement.
Methods
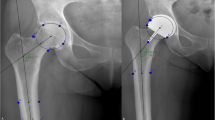
We evaluated the range of motion after hip resurfacing with various component orientations and optimal component orientations to avoid postoperative impingement using computer simulations in 10 male patients with osteonecrosis.
Results
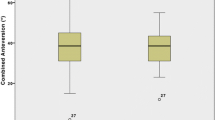
The mean ranges of motion in flexion, extension, abduction, adduction and internal rotation at 90° of flexion were 92.4° ± 13.8°, 25.7° ± 13.8°, 38.0° ± 11.1°, 29.1° ± 10.0° and 20.9° ± 11.5°, respectively. The oscillation angle in flexion and extension motion was 118.1° ± 10.3°. More than 100° of flexion was acquired in 79 of 240 simulations (32.9 %), and more than 20° extension was acquired in 142 simulations (59.2 %). Combined anteversion was significantly correlated with maximal flexion and extension angles. The component safe zone to fulfill the range of motion criteria varied among patients, and 4 of 10 patients had no safe zone.
Conclusions
Postoperative impingement occurs relatively frequently in hip resurfacing because of preservation of the femoral neck and component malpositioning. The safe zone of the acetabular component to avoid postoperative impingement is very narrow. Greater care should be taken regarding patient selection, rigorous preoperative planning and accurate component positioning.






Similar content being viewed by others

References
Vendittoli PA, Lavigne M, Girard J, Roy AG. A randomised study comparing resection of acetabular bone at resurfacing and total hip replacement. J Bone Joint Surg Br. 2006;88:997–1002.
Bengs BC, Sangiorgio SN, Ebramzadeh E. Less range of motion with resurfacing arthroplasty than with total hip arthroplasty: in vitro examination of 8 designs. Acta Orthop. 2008;79:755–62.
Kluess D, Zietz C, Lindner T, Mittelmeier W, Schmitz KP, Bader R. Limited range of motion of hip resurfacing arthroplasty due to unfavorable ratio of prosthetic head size and femoral neck diameter. Acta Orthop. 2008;79:748–54.
Quesada MJ, Marker DR, Mont MA. Metal-on-metal hip resurfacing. J Arthroplasty. 2008;23(Suppl):69–73.
Vail TP. Hip resurfacing. J Am Acad Orthop Surg. 2011;19(4):236–44.
McMinn DJ, Daniel J, Ziaee H, Pradhan C. Indications and results of hip resurfacing. Int Orthop. 2011;35:231–7.
Amstutz HC, Le Duff MJ. Eleven years of experience with metal-on-metal hybrid hip resurfacing. J Arthroplasty. 2008;23(Suppl 1):36–43.
Vendittoli PA, Ganapathi M, Nuño N, Plamondon D, Lavigne M. Factors affecting hip range of motion in surface replacement arthroplasty. Clin Biomech (Bristol, Avon). 2007;22:1004–12.
Malviya A, Lingard EA, Malik A, Bowman R, Holland JP. Hip flexion after Birmingham hip resurfacing. J Arthroplasty. 2010;25:387–91.
Gruen TA, Le Duff MJ, Wisk LE, Amstutz HC. Prevalence and clinical relevance of radiographic signs of impingement in metal-on-metal hybrid hip resurfacing. J Bone Joint Surg Am. 2011;93:1519–26.
Widmer KH, Zurfluh B. Compliant positioning of total hip components for optimal range of motion. J Orthop Res. 2004;22:815–21.
Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR. Dislocations after total hip replacement arthroplasties. J Bone Joint Surg Am. 1978;60:217–20.
Tannast M, Siebenrock KA, Anderson SE. Femoroacetabular impingement. AJR Am J Roentgenol. 2007;188:1540–52.
Murray DW. The definition and measurement of acetabular orientation. J Bone Joint Surg Br. 1993;75:228–32.
Davis ET, Olsen M, Zdero R, Waddell JP, Schemitsch EH. Femoral neck fracture following hip resurfacing. J Bone Joint Surg Br. 2008;90:1522–7.
Sakagoshi D, Kabata T, Umemoto Y, Sakamoto J, Tomita K. A mechanical analysis of femoral resurfacing implantation for osteonecrosis of the femoral head. J Arthroplasty. 2010;25:1282–9.
Yamamura M, Miki H, Nakamura N, Murai M, Yoshikawa H, Sugano N. Open-configuration MRI study of femoro-acetabular impingement. J Orthop Res. 2007;25:1582–8.
Miki H, Yamanashi W, Nishii T, Sato Y, Yoshikawa H, Sugano N. Anatomic hip range of motion after implantation during total hip arthroplasty as measured by a navigation system. J Arthroplasty. 2007;22:946–52.
Hagio K, Sugano N, Nishii T, Miki H, Otake Y, Hattori A, Suzuki N, Yonenobu K, Yoshikawa H, Ochi T. A novel system of four-dimensional motion analysis after total hip arthroplasty. J Orthop Res. 2004;22:665–70.
Incavo SJ, Thompson MT, Gold JE, Patel RV, Icenogle KD, Noble PC. Which procedure better restores intact hip range of motion. J Arthroplasty. 2011;26:391–7.
Lavigne M, Rama KR, Roy A, Vendittoli PA. Painful impingement of the hip joint after total hip resurfacing. J Arthroplasty. 2008;23:1074–9.
Le Duff MJ, Wisk LE, Amstutz HC. Range of motion after stemmed total hip arthroplasty and hip resurfacing. Bull NYU Hosp Jt Dis. 2009;67:177–81.
Langton DJ, Sprowson AP, Joyce TJ, Reed M, Carluke I, Partington P, Nargol AV. Blood metal ion concentrations after hip resurfacing arthroplasty. J Bone Joint Surg Br. 2009;91:1287–95.
Grammatopoulos G, Pandit H, Glyn-Jones S, McLardy-Smith P, Gundle R, Whitwell D, Gill HS, Murray DW. Optimal acetabular orientation for hip resurfacing. J Bone Joint Surg Br. 2010;92:1072–8.
Beaulé PE, Harvey N, Zaragoza E, Le Duff MJ, Dorey FJ. The femoral head/neck offset and hip resurfacing. J Bone Joint Surg Br. 2007;89:9–15.
Conflict of interest
All authors have no conflict of interest in relation to this study.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article
Cite this article
Kajino, Y., Kabata, T., Maeda, T. et al. Strict component positioning is necessary in hip resurfacing. J Orthop Sci 18, 290–297 (2013). https://doi.org/10.1007/s00776-012-0351-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00776-012-0351-4