
Abstract
Background
Pituitary apoplexy is a rare and life-threatening complication occurring in 0.6–10.5% of all cases of pituitary adenomas. Although the association between pituitary apoplexy and visual dysfunction has been recognized for a long time, the optimal management of this problem still remains controversial. The purpose of this overview was to present the surgical experience by analyzing the literature on the management of pituitary apoplexy for better treatment of these cases.
Materials and method
To establish a new guideline for the surgical treatment of this entity, publications reported during the last century and databases containing medical literature were analyzed. In addition, an illustrative case with pituitary apoplexy presenting with complaints of sudden onset severe headache associated with nausea, vomiting, and a sudden loss of vision was described. In fact, the experience in our complicated patient prompted us to review the available literature on the management of pituitary apoplexy to date.
Conclusions
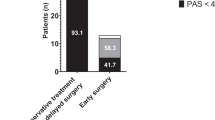
Based on an overview of 186 cases of apoplectic pituitary adenoma presenting with monocular or binocular blindness, we highlight the importance of correct diagnosis and an early, but not necessarily emergency, surgery within the first week of admission to optimize visual outcome of such patients. The illustrative case further exemplifies the value of close interaction between members of the management team for optimal outcome.



Similar content being viewed by others

References
Ayuk J, McGregor EJ, Mitchell RD, Gittoes NJL (2004) Acute management of pituitary apoplexy—surgery or conservative management? Clin Endocrinol (Oxf) 61:747–752
Bills D, Meyer F, Laws E, Davis DH, Ebersold M, Scheithauer BW, Ilstrup DM, Abboud CF (1993) A retrospective analysis of pituitary apoplexy. Neurosurgery 33:602–609
Cardosa ER, Peterson EW (1984) Pituitary apoplexy: a review. Neurosurgery 14:363–373
Elsässer Imboden PN, De Tribolet N, Lobrinus A, Gaillard RC, Portmann L, Pralong F, Gomez F (2005) Apoplexy in pituitary macroadenoma: eight patients presenting in 12 months. Medicine (Baltimore) 84:188–196
Mohr G, Hardy J (1982) Hemorrhage, necrosis, and apoplexy in pituitary adenomas. Surg Neurol 18:181–189
Onesti ST, Wisniewski T, Post KD (1990) Clinical versus subclinical pituitary apoplexy: presentation, surgical management, and outcome in 21 patients. Neurosurgery 26:980–986
Randeva HS, Schoebel J, Byrne J, Esiri M, Adams CBT, Wass JAH (1999) Classical pituitary apoplexy: clinical features, management and outcome. Clin Endocrinol (Oxf) 51:181–188
Semple P, Webb MK, de Villiers JC, Laws ER (2005) Pituitary apoplexy. Neurosurgery 56:65–73
Cohen AR, Cooper PR, Kupersmith MJ, Flamm ES, Ransohoff J (1985) Visual recovery after transsphenoidal removal of pituitary adenomas. Neurosurgery 17:446–452
Maccagnan P, Macedo CLD, Kayath MJ, Nogueira RG, Abucham J (1995) Conservative management of pituitary apoplexy: a prospective study. J Clin Endocrinol Metab 80:2190–2197
McFadzean RM, Doyle D, Rampling R, Teasdale E, Teasdale G (1991) Pituitary apoplexy and its effect on vision. Neurosurgery 29:669–675
Post MJD, David NJ, Glaser JS, Safran A (1980) Pituitary apoplexy: diagnosis by computed tomography. Radiology 134:665–670
Agrawal D, Mahapatra AK (2005) Visual outcome of blind eyes in pituitary apoplexy after transsphenoidal surgery: a series of 14 eyes. Surg Neurol 63:42–46
Chuang CC, Chang CN, Wei KC, Lao CC, Hsu PW, Huang YC, Chen YL, Lai LJ, Pai PC (2006) Surgical treatment of severe visual compromised patients after pituitary apoplexy. J Neurooncol 80:39–47
Goodman JM, Gilson M, Shapiro B (1973) Pituitary apoplexy—a cause of sudden blindness. J Indiana Sate Med Assoc 66:320–321
Henderson WR (1939) The pituitary adenomata—a follow-up study of the surgical results in 338 cases (Dr. Harvey Cushing’s series). Br J Surg 26:811–921
Kaplan B, Day AL, Quisling R, Ballinger W (1983) Hemorrhage into pituitary adenomas. Surg Neurol 20:280–287
Laws ER Jr, Trautmann JC, Hollenhorst RW (1977) Transsphenoidal decompression of the optic nerve and chiasm. Visual results in 62 patients. J Neurosurg 46:717–722
McLarty DG, Kermali W, Makene WJ (1982) Pituitary tumours and blindness: continuation of the Pre-Harvey Cushing era in developing countries. Lancet 2:810–811
Muthukumar N, Rosette D, Soundaram M, Senthilbabu S, Badrinarayanan T (2008) Blindness following pituitary apoplexy: timing of surgery and neuro-ophthalmic outcome. J Clin Neurosci 15:873–879
Parent AD (1990) Visual recovery after blindness from pituitary apoplexy. Can J Neurol Sci 17:88–91
Peter M, de Tribolet N (1995) Visual outcome after trans-sphenoidal surgery for pituitary adenomas. Br J Neurosurg 9:151–157
Robinson JL, Chir B (1972) Sudden blindness with pituitary tumors: report of three cases. J Neurosurg 36:83–85
Rovit RL, Fein JM (1972) Pituitary apoplexy: a review and reappraisal. J Neurosurg 37:280–288
Shenkin HA (1955) Relief of amblyopia in pituitary apoplexy by prompt surgical intervention. J Am Med Assoc 159:1622–1624
Suri A, Narang KS, Sharma BS, Mahapatra AK (2008) Visual outcome after surgery in patients with suprasellar tumors and preoperative blindness. J Neurosurg 108:19–25
Symon L, Mohanty S (1982) Hemorrhage in pituitary tumours. Acta Neurochir (Wien) 65:41–49
Waybright EA, Selhorst JB, Young HF, Harbison JW (1983) Tumors compressing the optic nerve: diagnosis and surgical results. Va Med 110:230–234
Brougham M, Heusner AP, Adams RD (1950) Acute degenerative changes in adenomas of the pituitary body—with special reference to pituitary apoplexy. J Neurosurg 7:421–439
Nakahara K, Oka H, Utsuki S, Iida H, Kurita M, Mochizuki T, Fujii K (2006) Pituitary apoplexy manifesting as diffuse subarachnoid hemorrhage. Neurol Med Chir (Tokyo) 46:594–597
Charalampaki P, Ayyad A, Kockro RA, Perneczky A (2009) Surgical complications after endoscopic transsphenoidal pituitary surgery. J Clin Neurosci 16:786–789
Sibal L, Ball SG, Connoly V, James RA, Kane P, Kelly WF, Kendall-Taylor P, Mathias D, Perros P, Quinton R, Vaidya B (2004) Pituitary apoplexy: a review of clinical presentation, management and outcome in 45 cases. Pituitary 7:157–163
Uihlein A, Balfour WM, Donovan PF (1957) Acute hemorrhage into pituitary adenomas. J Neurosurg 14:140–151
Locatelli M, Spagnoli D, Isalberti M, Branca V, Gaini SM, Lania A (2008) A potential catastrophic trap: an unusually presenting sellar lesion. Eur J Neurol 15:98–101
Okawara M, Yamaguchi H, Hayashi S, Matsumoto Y, Inoue Y, Okwara S (2007) A case of ruptured carotid artery aneurysm mimicking pituitary apoplexy (in Japanase). No Shinkei Geka 35:1169–1174
Romano A, Chibbaro S, Marsella M, Ippolito S, Benericetti E (2006) Carotid cavernous aneurysm presenting as pituitary apoplexy. J Clin Neurosci 13:476–479
Suzuki H, Muramatsu M, Murao K, Kawaguchi K, Shimizu T (2001) Pituitary apoplexy caused by ruptured internal carotid aneurysm. Stroke 32:567–569
Iqbal J, Kanan I, Al Homsi M (1999) Non-neoplastic cystic lesions of the sellar region presentation, diagnosis and management of eight cases and review of the literature. Acta Neurochir (Wien) 141:389–397
Griffith HB, Veerapen R (1987) A direct transnasal approach to the sphenoid sinus. Technical note. J Neurosurg 66:140–142
Jankowski R, Auque J, Simon C, Marchal JC, Hepner H, Wayoff M (1992) Endoscopic pituitary tumor surgery. Laryngoscope 102:198–202
Cavallo LM, Prevedello D, Esposito F, Laws ER Jr, Dusick JR, Messina A, Jane JA Jr, Kelly DF, Cappabianca P (2008) The role of the endoscope in the transsphenoidal management of cystic lesions of the sellar region. Neurosurg Rev 31:55–64
Jho HD, Carrau RL (1997) Endoscopic endonasal transsphenoidal surgery: experience with 50 patients. J Neurosurg 87:44–51
Pelkonen R, Kuusisto A, Salmi J, Eistola P, Raitta C, Karonen SL, Aro A (1978) Pituitary function after pituitary apoplexy. Am J Med 65:773–778
Nemergut EC, Zuo Z, Jane JA Jr, Laws ER Jr (2005) Predictors of diabetes insipidus after transsphenoidal surgery: a review of 881 patients. J Neurosurg 103:448–454
Maurer J, Hinni M, Mann W, Pfeiffer N (1999) Optic nerve decompression in trauma and tumor patients. Eur Arch Otorhinolaryngol 256:341–345
Acknowledgments
We wish to express our sincere thanks and appreciation to Dr. Mete Önde for his assistance during statistical analysis of the data.
Author information
Authors and Affiliations
Corresponding author
Additional information
This is an overview of a very large series of pituitary apoplexy patients with a single illustrative case from a single institution. The authors make valid comments about surgical intervention and are saying, in essence, that it is always worth decompressing the visual apparatus if visual loss is severe.
As always, the discussion on timing of intervention is hampered by the retrospective nature of the series, but this adds valuable information to the surgical argument.
Ultimately, the answer will not be properly made until a carefully constructed RCT has been made, but for pituitary surgeons, aploplexy with visual loss is like central lumbar disk prolapse with cauda equina loss—if it was ourselves, we would want the operation done by an expert transsphenoidal surgeon once we had been biochemically and endocrinologically stabilized.
Michael Powell
London, UK
Rights and permissions
About this article
Cite this article
Turgut, M., Özsunar, Y., Başak, S. et al. Pituitary apoplexy: an overview of 186 cases published during the last century. Acta Neurochir 152, 749–761 (2010). https://doi.org/10.1007/s00701-009-0595-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-009-0595-8