
Abstract
Purpose
We examined the impact of advanced age on left ventricular mass regression and the change in the diastolic function after aortic valve replacement in patients with aortic stenosis.
Methods
The present study included 129 patients who underwent either surgical or transcatheter aortic valve replacement and 1-year postoperative echocardiography. The patient characteristics and echocardiographic findings were compared between patients who were <80 years of age (group Y: n = 69) and those who were ≥80 years of age (group O: n = 60).
Results
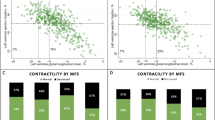
Preoperative echocardiography revealed that although the left ventricular mass was similar between the groups, the patients in group O had more severe diastolic dysfunction in comparison to those in group Y. Postoperatively, left ventricular mass regression was significantly greater (p = 0.02) and diastolic dysfunction was less prevalent in group Y (p = 0.02) in comparison to group O. The change in E/e′ was significantly correlated with the left ventricular mass regression in group Y (p = 0.02), but not in Group O (p = 0.21).
Conclusions
The patients in group O were less susceptible to improvements in myocardial remodeling and the diastolic function in comparison to those in group Y. The altered physiological response to aortic valve replacement might help to determine the appropriate timing of surgery in elderly patients.


Similar content being viewed by others


References
Kodali SK, Williams MR, Smith CR, Svensson LG, Webb JG, Makkar RR, et al. Two-year outcomes after transcatheter or surgical aortic-valve replacement. N Engl J Med. 2012;366:1686–95.
Tsukui H, Yamazaki K. Contemporary strategy for aortic valve stenosis in octogenarians. Surg Today. 2014;44:992–1003.
Sawa Y. Transcatheter aortic valve implantation. Surg Today. 2015;45:527–36.
Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, Guyton RA, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:e57–185.
Baumgartner H. Aortic stenosis: medical and surgical management. Heart. 2005;91:1483–8.
Marumoto A, Nakamura Y, Kishimoto Y, Saiki M, Nishimura M. Optimal timing of aortic valve replacement in elderly patients with severe aortic stenosis. Surg Today. 2014;44:84–93.
Schulz O, Brala D, Bensch R, Krämer J, Schulz-Menger J, Berghoefer G, et al. Aortic valve replacement in asymptomatic and symptomatic patients with preserved left ventricular ejection fraction. J Heart Valve Dis. 2012;21:576–83.
Taniguchi T, Morimoto T, Shiomi H, Ando K, Kanamori N, Murata K, et al. Initial surgical versus conservative strategies in patients with asymptomatic severe aortic stenosis. J Am Coll Cardiol. 2015;66:2827–38.
Nakamura T, Toda K, Kuratani T, Miyagawa S, Yoshikawa Y, Fukushima S, et al. Diabetes mellitus impairs left ventricular mass regression after surgical or transcatheter aortic valve replacement for severe aortic stenosis. Heart Lung Circ. 2016;25:68–74.
Villari B, Vassalli G, Monrad ES, Chiariello M, Turina M, Hess OM. Normalization of diastolic dysfunction in aortic stenosis late after valve replacement. Circulation. 1995;91:2353–8.
Elmariah S. Patterns of left ventricular remodeling in aortic stenosis: therapeutic implications. Curr Treat Options Cardiovasc Med. 2015;17:391.
Une D, Mesana L, Chan V, Maklin M, Chan R, Masters RG, et al. Clinical Impact of Changes in Left Ventricular Function After Aortic Valve Replacement: Analysis From 3112 Patients. Circulation. 2015;132:741–7.
Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16:31–41.
Maeda K, Kuratani T, Torikai K, Ichibori Y, Nakatani K, Onishi T, et al. Early outcomes in Japanese dialysis patients treated with transcatheter aortic valve implantation. Circ J. 2015;79:2713–9.
Nishi H, Toda K, Miyagawa S, Yoshikawa Y, Fukushima S, Kawamura M, Yoshioka D, Saito T, Ueno T, Kuratani T, Sawa Y. Annular dynamics after mitral valve repair with different prosthetic rings: a real-time three-dimensional transesophageal echocardiography study. Surg Today. 2016;46:1083–90.
Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J Am Soc Echocardiogr. 2009;22:1–23.
Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, et al. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol. 1986;57:450–8.
Emery WT, Jadavji I, Choy JB, Lawrance RA. Investigating the European Society of Cardiology Diastology Guidelines in a practical scenario. Eur J Echocardiogr. 2008;9:685–91.
Gavina C, Falcão-Pires I, Pinho P, Manso MC, Gonçalves A, Rocha-Gonçalves F, et al. Relevance of residual left ventricular hypertrophy after surgery for isolated aortic stenosis. Eur J Cardiothorac Surg. 2016;49:952–9.
Seo JS, Jang MK, Lee EY, Yun SC, Kim DH, Song JM, et al. Evaluation of left ventricular diastolic function after valve replacement in aortic stenosis using exercise Doppler echocardiography. Circ J. 2012;76:2792–8.
Maruyama Y. Aging and arterial-cardiac interactions in the elderly. Int J Cardiol. 2012;155:14–9.
Villari B, Vassalli G, Schneider J, Chiariello M, Hess OM. Age dependency of left ventricular diastolic function in pressure overload hypertrophy. J Am Coll Cardiol. 1997;29:181–6.
Ding WH, Lam YY, Pepper JR, Kaya MG, Li W, Chung R, et al. Early and long-term survival after aortic valve replacement in septuagenarians and octogenarians with severe aortic stenosis. Int J Cardiol. 2010;141:24–31.
Kato M, Yamamoto K. Clinical characteristics of elderly patients with aortic stenosis. J Echocardiogr. 2015;13:134–40.
Owen A, Henein MY. Challenges in the management of severe asymptomatic aortic stenosis. Eur J Cardiothorac Surg. 2011;40:848–50.
Kim SJ, Samad Z, Bloomfield GS, Douglas PS. A critical review of hemodynamic changes and left ventricular remodeling after surgical aortic valve replacement and percutaneous aortic valve replacement. Am Heart J 2014;168:150-9.e1-7.
Howell NJ, Keogh BE, Ray D, Bonser RS, Graham TR, Mascaro J, et al. Patient-prosthesis mismatch in patients with aortic stenosis undergoing isolated aortic valve replacement does not affect survival. Ann Thorac Surg. 2010;89:60–4.
Flameng W, Meuris B, Herijgers P, Herregods M-C. Prosthesis-patient mismatch is not clinically relevant in aortic valve replacement using the Carpentier-Edwards Perimount valve. Ann Thorac Surg. 2006;82:530–6.
Dayan V, Vignolo G, Soca G, Paganini JJ, Brusich D, Pibarot P. Predictors and outcomes of prosthesis-patient mismatch after aortic valve replacement. JACC Cardiov Imag 2016 [Epub ahead of print].
Fairbairn TA, Steadman CD, Mather AN, Motwani M, Blackman DJ, Plein S, et al. Assessment of valve haemodynamics, reverse ventricular remodelling and myocardial fibrosis following transcatheter aortic valve implantation compared to surgical aortic valve replacement: a cardiovascular magnetic resonance study. Heart. 2013;99:1185–91.
Crouch G, Bennetts J, Sinhal A, Tully PJ, Leong DP, Bradbrook C, et al. Early effects of transcatheter aortic valve implantation and aortic valve replacement on myocardial function and aortic valve hemodynamics: insights from cardiovascular magnetic resonance imaging. J Thorac Cardiovasc Surg. 2015;149:462–70.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest in association with the present study.
Rights and permissions
About this article

Cite this article
Nakamura, T., Toda, K., Kuratani, T. et al. The impact of age on the postoperative response of the diastolic function and left ventricular mass regression after surgical or transcatheter aortic valve replacement for severe aortic stenosis. Surg Today 47, 770–776 (2017). https://doi.org/10.1007/s00595-016-1458-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-016-1458-6