
Abstract
Purpose
Patients with advanced cancer may be referred for a palliative care consultation (PC) from a hospital emergency center (EC) or as inpatients. However, research about symptoms and outcomes in patients with advanced cancer who receive PC at the EC is limited.
Methods
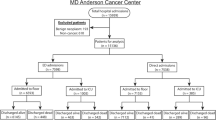
We reviewed demographic variables, frequency and intensity of symptoms (using the Edmonton Symptom Assessment Scale (ESAS)), PC interventions, time from admission to PC consultation, hospitalization duration, and discharge destination of 200 advanced cancer patients referred to PC services from the EC (“EC patients”) and 200 matched advanced cancer inpatients referred to PC services (“inpatients”) from January 1, 2010, through December 31, 2011.
Results
The median age for all patients was 56 years (range, 48–64 years); 222 (56 %) patients were female, and 243 (61 %) were white. There were no significant demographic differences between the EC patients and inpatients. The median time from admission to PC was 12 h (range, 7–23 h) for the EC patients and 24 h (24–96 h) for the inpatients (p < 0.0001). For EC patients and inpatients, symptoms at presentation for PC consultation included uncontrolled pain (83 and 45 %, respectively; p < 0.0001), nausea/vomiting/constipation (41 and 19 %, respectively; p < 0.0001), and dyspnea (29 and 19 %, respectively; p = 0.02). The medians and interquartile ranges of baseline symptom intensities for EC patients and inpatients, respectively, were as follows: pain, 7 (5–9) and 5 (2–8) (p < 0.0001); fatigue, 7 (4–8) and 6 (4–8) (p = 0.0517); and sleep, 6 (0–8) and 4 (1–7) (p = 0.1064). At follow-up, improvement was observed in pain (125/238 [53 %]), sleep (59/131 [45 %]), well-being (32/82 [39 %]), fatigue (53/139 [38 %]), anxiety (51/132 [39 %]), appetite (46/132 [35 %]), dyspnea (49/160 [31 %]), nausea (52/170 [31 %]), depression (36/123 [29 %]), and drowsiness (37/126 [29 %]). After PC consultations, discharge/admission destinations for EC patients were as follows: home, 65 (33 %); home hospice, 13 (7 %); inpatient hospice, 8 (4 %); regular hospital floor, 65 (33 %); and PC unit, 46 (23 %). The median duration of hospitalization was 92 h (range, 69–114) for hospitalized EC patients and 125 h (range, 108–142) for inpatients (p < 0.0001).
Conclusions
Referral to PC from the EC led to earlier delivery of PC with subsequent earlier control of symptoms. EC patients who received PC consultations and were hospitalized had shorter hospitalizations than PC referral in the inpatient area. More research is needed to describe the impact of PC services on symptom assessment and management and on goals and plan of care in patients with advanced illness admitted to the EC.

Similar content being viewed by others


References
Lamba S (2009) Early goal-directed palliative therapy in the emergency department: a step to move palliative care upstream. J Palliat Med 12(9):767
Chan GK (2004) End-of-life models and emergency department care. Acad Emerg Med 11(1):79–86
Lawson BJ, Burge FI, McIntyre P, Field S, Maxwell D (2009) Can the introduction of an integrated service model to an existing comprehensive palliative care service impact emergency department visits among enrolled patients? J Palliat Med 12(3):245–252
Fukui S, Yoshiuchi K, Fujita J, Sawai M, Watanabe M (2011) Japanese people’s preference for place of end-of-life care and death: a population-based nationwide survey. J Pain Symptom Manag 42(6):882–892
Gomes B, Higginson IJ, Calanzani N, Cohen J, Deliens L, Daveson BA, et al. (2012) Preferences for place of death if faced with advanced cancer: a population survey in England, Flanders, Germany, Italy, the Netherlands, Portugal and Spain. Ann Oncol 23(8):2006–2015
Barbera L, Taylor C, Dudgeon D (2010) Why do patients with cancer visit the emergency department near the end of life? Cmaj 182(6):563–568
Huang J, Boyd C, Tyldesley S, Zhang-Salomons J, Groome PA, Mackillop WJ (2002) Time spent in hospital in the last six months of life in patients who died of cancer in Ontario. J Clin Oncol 20(6):1584–1592
Earle CC, Park ER, Lai B, Weeks JC, Ayanian JZ, Block S (2003) Identifying potential indicators of the quality of end-of-life cancer care from administrative data. J Clin Oncol 21(6):1133–1138
Earle CC, Neville BA, Landrum MB, Souza JM, Weeks JC, Block SD, et al. (2005) Evaluating claims-based indicators of the intensity of end-of-life cancer care. Int J Qual Health Care 17(6):505–509
Meo N, Hwang U, Morrison RS (2011) Resident perceptions of palliative care training in the emergency department. J Palliat Med 14(5):548–555
Quest TE, Marco CA, Derse AR (2009) Hospice and palliative medicine: new subspecialty, new opportunities. Ann Emerg Med 54(1):94–102
Smith AK, Fisher J, Schonberg MA, Pallin DJ, Block SD, Forrow L, et al. (2009) Am I doing the right thing? Provider perspectives on improving palliative care in the emergency department. Ann Emerg Med 54(1):86–93
Grudzen CR, Hwang U, Cohen JA, Fischman M, Morrison RS (2012) Characteristics of emergency department patients who receive a palliative care consultation. J Palliat Med 15(4):396–399
Lamba S, Nagurka R, Walther S, Murphy P (2012) Emergency-department-initiated palliative care consults: a descriptive analysis. J Palliat Med 15(6):633–636
Norton CK, Hobson G, Kulm E (2011) Palliative and end-of-life care in the emergency department: guidelines for nurses. J Emerg Nurs 37(3):240–245
Rondeau DF, Schmidt TA (2009) Treating cancer patients who are near the end of life in the emergency department. Emerg Med Clin North Am 27(2):341–354
Yennurajalingam S, Zhang T, Bruera E (2007) The impact of the palliative care mobile team on symptom assessment and medication profiles in patients admitted to a comprehensive cancer center. Support Care Cancer 15(5):471–475
Elsayem A, Swint K, Fisch MJ, Palmer JL, Reddy S, Walker P, et al. (2004) Palliative care inpatient service in a comprehensive cancer center: clinical and financial outcomes. J Clin Oncol 22(10):2008–2014
Bruera E, Kuehn N, Miller MJ, Selmser P, Macmillan K (1991) The Edmonton Symptom Assessment System (ESAS): a simple method for the assessment of palliative care patients. J Palliat Care 7(2):6–9
Chang VT, Hwang SS, Feuerman M (2000) Validation of the Edmonton Symptom Assessment Scale. Cancer 88(9):2164–2171
Stromgren AS, Groenvold M, Petersen MA, Goldschmidt D, Pedersen L, Spile M, et al. (2004) Pain characteristics and treatment outcome for advanced cancer patients during the first week of specialized palliative care. J Pain Symptom Manag 27(2):104–113
Centeno C, Sanz A, Bruera E. Delirium in advanced cancer patients (2004). Palliat Med 18(3):184–194
de Rooij SE, Schuurmans MJ, van der Mast RC, Levi M (2005) Clinical subtypes of delirium and their relevance for daily clinical practice: a systematic review. Int J Geriatr Psychiatry 20(7):609–615
Lawlor PG, Nekolaichuk C, Gagnon B, Mancini IL, Pereira JL, Bruera ED (2000) Clinical utility, factor analysis, and further validation of the Memorial Delirium Assessment Scale in patients with advanced cancer: assessing delirium in advanced cancer. Cancer 88(12):2859–2867
Farrar JT, Young Jr JP, LaMoreaux L, Werth JL, Poole RM (2001) Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 94:149–158
Yennurajalingam S, Urbauer DL, Casper KLB, et al. (2011) Impact of a palliative care consultation team on cancer-related symptoms in advanced cancer patients referred to an outpatient supportive care clinic. J Pain Symptom Manag 41:49–56
Hui D, Shamieh O, Paiva CE, et al. (2015) Minimal clinically important differences in the Edmonton Symptom Assessment Scale in cancer patients: a prospective, multicenter study. Cancer 121:3027–3035
DeVader TE, Jeanmonod R (2012) The effect of education in hospice and palliative care on emergency medicine residents’ knowledge and referral patterns. J Palliat Med 15(5):510–515
Smith AK, McCarthy E, Weber E, Cenzer IS, Boscardin J, Fisher J, et al. (2012) Half of older Americans seen in emergency department in last month of life; most admitted to hospital, and many die there. Health Aff (Millwood) 31(6):1277–1285
Glajchen M, Lawson R, Homel P, Desandre P, Todd KH (2011) A rapid two-stage screening protocol for palliative care in the emergency department: a quality improvement initiative. J Pain Symptom Manag 42(5):657–662
Wallace EM, Cooney MC, Walsh J, Conroy M, Twomey F (2013) Why do palliative care patients present to the emergency department? Avoidable or unavoidable? Am J Hosp Palliat Care 30(3):253–256
Smith AK, Schonberg MA, Fisher J, Pallin DJ, Block SD, Forrow L, et al. (2010) Emergency department experiences of acutely symptomatic patients with terminal illness and their family caregivers. J Pain Symptom Manag 39(6):972–981
Hjermstad MJ, Kolflaath J, Lokken AO, Hanssen SB, Normann AP, Aass N (2013) Are emergency admissions in palliative cancer care always necessary? Results from a descriptive study. BMJ Open 3(5)
Lukin W, Douglas C, O’Connor A (2012) Palliative care in the emergency department: an oxymoron or just good medicine? Emerg Med Australas 24(1):102–104
Meier DE, Beresford L (2007) Fast response is key to partnering with the emergency department. J Palliat Med 10(3):641–645
Lamba S, DeSandre PL, Todd KH, et al. (2014) Improving palliative care in emergency medicine board. Integration of palliative care into emergency medicine: the Improving Palliative Care in Emergency Medicine (IPAL-EM) collaboration. J Emerg Med 46(2):264–270
Lamba S, Schmidt TA, Chan GK, et al. (2013) IPAL-EM Board. Integrating palliative care in the out-of-hospital setting: four things to jump-start an EMS-palliative care initiative. Prehosp Emerg Care 17(4):511–520
Quest T, Herr S, Lamba S, Weissman D (2013) IPAL-EM Advisory Board. Demonstrations of clinical initiatives to improve palliative care in the emergency department: a report from the IPAL-EM Initiative. Ann Emerg Med 61(6):661–667
Wu FM, Newman JM, Lasher A, Brody AA (2013) Effects of initiating palliative care consultation in the emergency department on inpatient length of stay. J Palliat Med 16(11):1362–1367
Grudzen CR, Richardson LD, Morrison M, Cho E, Morrison RS (2010) Palliative care needs of seriously ill, older adults presenting to the emergency department. Acad Emerg Med 17(11):1253–1257
Shin SH, Hui D, Chisholm GB, Kwon JH, San-Miguel MT, Allo JA, et al. (2014) Characteristics and outcomes of patients admitted to the acute palliative care unit from the emergency center. J Pain Symptom Manag 47(6):1028–1034
IOM (Institute of Medicine). Delivering high-quality cancer care. Charting a new course for a system in crisis. Institute of Medicine of the National Academies. The National Academies press. Washington DC 2013.
Acknowledgments
Dr. E. Bruera is supported in part by National Institutes of Health grants R01NR010162-01A1, R01CA122292-01, and R01CA124481-01.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Delgado-Guay, M.O., Rodriguez-Nunez, A., Shin, S.H. et al. Characteristics and outcomes of patients with advanced cancer evaluated by a palliative care team at an emergency center. A retrospective study. Support Care Cancer 24, 2287–2295 (2016). https://doi.org/10.1007/s00520-015-3034-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-015-3034-9