
Abstract
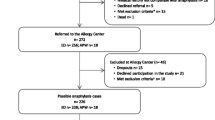
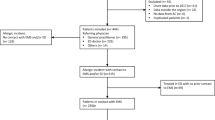
Anaphylaxis remains under-diagnosed and under-treated. A better knowledge of patterns and triggers of anaphylaxis might contribute to a better management. In this study we evaluated the demographic and clinical features of anaphylaxis in pediatric patients, as well as its triggers and therapeutic approach. From May 1st 2004 until April 30th 2006 we prospectively collected data on all patients referred for investigation of anaphylaxis to the pediatric department of the University Hospital Gasthuisberg Leuven and to two private pediatric practices. Data were stored in a MYSQL database by use of an online encrypted web form. Sixty-four cases of anaphylaxis occurred in 48 children, aged 6 months to 14.8 years. Twenty-seven episodes (42.2%) occurred at home. The symptoms were dermatologic in 62 (96.9%) episodes, respiratory in 57 (89.1%), gastrointestinal in 19 (29.7%), cardiovascular in 14 (21.8%), and neurological or behavioural in 19 (29.7%). Antihistamines were administered in 41/57 (71.9%) cases, corticosteroids in 26/57 (45.6%), beta-2-mimetics in 14/57 (24.6%), and adrenaline in 11/57 (19.3%). Out of nine cases where Epipen was available at the moment of anaphylaxis, it was administered in one case only. Food was the cause of anaphylaxis in 42/55 (76.4%) cases with identified trigger, while medication, insect stings, latex, and birch pollen triggered 5 (9.1%), 4 (7.3%), 3 (5.5%), and 1 (1.8%) case(s), respectively. Allergy to the trigger was known prior to anaphylaxis in 19/55 (34.5%) cases. In conclusion, anaphylaxis in pediatric patients generally presents with dermatologic and respiratory symptoms, while in 1/5 episodes cardiovascular symptoms occur. Food is by far the most frequent trigger. Allergy to the trigger is known in 1/3 cases only. Anaphylaxis is under-treated, even when appropriate medication is available.



Similar content being viewed by others

Abbreviations
- SPT:
-
skin prick test
References
Bock SA, Munoz-Furlong A, Sampson HA (2001) Fatalities due to anaphylactic reactions to foods. J Allergy Clin Immunol 107:191–193
Bohlke K, Davis RL, DeStefano F, Marcy SM, Braun MM, Thompson RS (2004) Epidemiology and anaphylaxis among children and adolescents enrolled in a health maintenance organisation. J Allergy Clin Immunol 113:536–542
Boros CA, Kay D, Gold MS (2000) Parent reported allergy and anaphylaxis in 4173 South Australian children. J Paediatric Child Health 36:36–40
Ceuppens JL (2005) Anafylaxie en veralgemeende vormen van acute allergische reacties: een overzicht. Tijdschr voor Geneeskunde 61:1142–1149
De Swert LF (2005) Anafylaxie bij kinderen. Tijdschr voor Geneeskunde 61:1150–1154
Dibs SD, Baker MD (1997) Anaphylaxis in children: a 5-year experience. Pediatrics 99(1):E7
Dreborg S, Foucard T (1983) Allergy to apple, carrot and potato in children with birch pollen allergy. Allergy 38:167–172
Ellis AK, Day JH (2007) Incidence and characteristics of biphasic anaphylaxis: a prospective evaluation of 103 patients. Ann Allergy Asthma Immunol 98:64–69
Gupta R, Sheikh A, Strachan P, Anderson HR (2004) Burden of allergic disease in the UK: secondary analyses of national databases. Clin Exp Allergy 34:520–526
Hebling A, Hurni T, Mueller UR, Pichler WJ (2004) Incidence of anaphylaxis with circulatory symptoms: a study over a 3-year period comprising 940,000 inhabitants of the Swiss Canton Bern. Clin Exp Allergy 34:285–290
Kochuyt AM, Van Hoeyveld EM, Stevens EA (2005) Prevalence and clinical relevance of specific immunoglobulin E to pollen caused by sting-induced specific immunoglobulin E to cross-reacting carbohydrate determinants in Hymenoptera venoms. Clin Exp Allergy 35:441–447
Krugman SD, Chiaramonte DR, Matsui EC (2006) Diagnosis and management of food-induced anaphylaxis: a national survey of pediatricians. Pediatrics 118:e554–e560
Lee JM, Greenes DS (2000) Biphasic anaphylactic reactions in pediatrics. Pediatrics 106:762–766
Lieberman P (2005) Biphasic anaphylactic reactions. Ann Allergy Asthma Immunol 95:217–226
Lieberman P, Camargo CA, Bohlke K, Jick H, Miller RL, Sheikh A, Simons FE (2006) Epidemiology of anaphylaxis: findings of the American College of Allergy, Asthma and Immunology Epidemiology of anaphylaxis working group. Ann Allergy Asthma Immunol 97:596–602
Lieberman P, Decker W, Camargo CA, O’Connor R, Oppenheimer J, Simons FE (2007) SAFE: a multidisciplinary approach to anaphylaxis education in the emergency department. Ann Allergy Asthma Immunol 98:519–523
Mehl A, Wahn U, Niggeman B (2005) Anaphylactic reactions in children—a questionnaire-based survey in Germany. Allergy 60:1440–1445
Mullins RJ (2003) Anaphylaxis: risk factors for recurrence. Clin Exp Allergy 33:1033–1040
Muraro A, Roberts G, Clark A, Eigenmann PA, Halken S, Lack G, Moneret-Vautrin M, Niggeman B, Rancé F; EAACI task force on anaphylaxis in children (2007) The management of anaphylaxis in childhood: position paper of the European academy of allergology and clinical immunology. Allergy 62:857–871
Muraro MA (2001) Diagnosis of food allergy: the oral provocation test. Pediatr Allergy Immunol 12(suppl 14):31–36
Novembre E, Cianferoni A, Bernardini R, Mugnaini L, Caffarelli C, Cavagni G, Giovane A, Vierucci A (1998) Anaphylaxis in children: clinical and allergologic features. Pediatrics Apr 101(4):E8
Osterballe O, Weeke B (1979) A new lancet for skin prick testing. Acta Paediatrica Scandinavica 34:209–212
Pichler WJ (2007) Drug hypersensitivity reactions: classification and relationship to T-cell activation. In: Pichler WJ (ed) Drug hypersensitivity. Karger, Basel pp169–189
Pumphrey R (2004) Anaphylaxis: can we tell who is at risk of a fatal reaction? Curr Opin Allergy Clin Immunol 4:285–290
Sampson HA (2004) Update on food allergy. J Allergy Clin Immunol 113:805–819
Sampson HA, Mendelson L, Rosen JP (1992) Fatal and near-fatal anaphylactic reactions to food in children and adolescents. N Eng J Med 327:380–384
Sampson HA, Munoz-Furlong A, Campbell RL, Adkinson F Jr, Bock A, Branum A, Brown SG, Camargo CA Jr, Cydulka R, Galli SJ, Gidudu J, Gruchalla RS, Harlor AD Jr, Hepner DL, Lewis LM, Lieberman PL, Metcalfe DD, O’Connor R, Muraro A, Rudman A, Schmitt C, Scherrer D, Simons FE, Thomas S, Wood JP, Decker WW (2006) Second symposium on the definition and management of anaphylaxis: summary report. J Allergy Clin Immunol 117:391–397
Simons FE (2006) Anaphylaxis, killer allergy: long-term management in the community. J Allergy Clin Immunol 367–377
Simons FE, Frew AJ, Ansotegui IJ, Bochner BS, Golden DB, Finkelman FD, Leung DY, Lotvall J, Marone G, Metcalfe DD, Müller U, Rosenwasser LJ, Sampson HA, Schwartz LB, van Hage M, Walls AF (2007) Risk assessment in anaphylaxis: current and future approaches. J Allergy Clin Immunol 120:S2–S24
Taylor SL, Hefle SL (2006) Food allergen labelling in the USA and Europe. Curr Opin Allergy Clin Immunol 6:186–190
Wood RA (2003) The natural history of food allergy. Pediatrics 111:1631–1633
Acknowledgements
We would like to thank Johannes Daniels for statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work has been partially sponsored by an unrestricted grant from UCB, Belgium.
Rights and permissions
About this article
Cite this article
De Swert, L.F.A., Bullens, D., Raes, M. et al. Anaphylaxis in referred pediatric patients: demographic and clinical features, triggers, and therapeutic approach. Eur J Pediatr 167, 1251–1261 (2008). https://doi.org/10.1007/s00431-007-0661-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-007-0661-2