
Abstract
Background
Catheter ablation has become the first line of therapy in patients with symptomatic, recurrent, drug-refractory atrial fibrillation (AF). Cryoablation has been shown to be a safe and effective technique for pulmonary vein (PV) isolation. However, the arrhythmia recurrence rate is high after cryoablation procedures. Radiofrequency catheter ablation has been shown to be an effective strategy for redo procedures in these patients and to provide a favourable outcome during midterm follow-up. The aim of this study was to analyse whether the strategy also provides favourable results during long-term follow-up (5 years).
Methods
In this study 30 patients (paroxysmal AF: 22 patients, persistent AF: 8 patients) underwent a redo procedure after initially successful circumferential PV isolation with the cryoballoon technique (Arctic Front Balloon, Medtronic). The redo ablation procedures were performed using a segmental approach or a circumferential ablation strategy (CARTO; Biosense Webster, Diamond Bar, CA, USA) depending on the intraprocedural findings.
Results
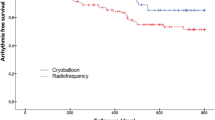
During the repeat procedure, a mean number of 2.9 reconnected PV (SD ± 1.0) were detected. In 20 patients, a segmental approach was sufficient to eliminate the residual PV conduction because only a few PV fibres were recovered (1–3 reconnected PV; group A). In the remaining 10 patients, a circumferential ablation strategy was used because of a complete recovery of the pulmonary vein – left atrial (PV-LA) conduction (group B). All reconnected PV were isolated successfully again. A third or fourth ablation procedure had to be performed in 4 (3 and 1, respectively) patients (13.3%). At 5‑year follow-up, 66.7% of all patients were free from an arrhythmia recurrence (20 out of 30). There were no major complications during long-term follow-up.
Conclusion
In patients with an initial circumferential PV isolation using the cryoballoon technique, a repeat ablation procedure can be safely and effectively performed using radiofrequency catheter ablation providing good long-term follow-up results.
Zusammenfassung
Hintergrund
Die Katheterablation hat sich in den letzten Jahren als Therapieoption bei Patienten mit rezidivierendem, symptomatischem, medikamentös-therapierefraktärem Vorhofflimmern etabliert. Die Kryoablation hat sich hierbei als sicheres und effektives Verfahren zur Pulmonalvenenisolation erwiesen. Dennoch ist die Rezidivrate nach Kryoablation hoch. Die Radiofrequenz-Ablation hat sich als effektive Strategie für Zweiteingriffe bei diesen Patienten bewährt und geht mit günstigen Resultaten im mittelfristigen Verlauf einher. Ziel dieser Studie war es zu analysieren, ob diese Strategie auch positive Ergebnisse im Langzeitverlauf über 5 Jahre zeigt.
Methodik
Insgesamt 30 Patienten (paroxysmales Vorhofflimmern: 22 Patienten, persistierendes Vorhofflimmern: 8 Patienten) mussten sich nach initial erfolgreicher Pulmonalvenenisolation mittels der Kryoballontechnik (Arctic Front; Medtronic) einer Reablation unterziehen. Die Reablation wurde in Abhängigkeit von den intraprozeduralen Befunden entweder als segmental-ostiale oder zirkumferenzielle (Carto; Biosense Websterm, Diamond Bar, CA, USA) Pulmonalvenenreisolation unter Verwendung von gekühlten Radiohochfrequenz-Energieapplikationen durchgeführt.
Ergebnisse
Während des Revisionseingriffs wurde eine Erholung der Pulmonalvenenleitung bei im Mittel 2,9 ± 1,0 Pulmonalvenen dokumentiert. Bei 20 Patienten war eine segmental-ostiale Ablationsstrategie ausreichend, da jeweils nur eine diskrete residuelle Pulmonalvenenleitung bestand (1–3 rekonnektierte PVs; Gruppe A). Bei den übrigen 10 Patienten wurde eine zirkumferenzielle Reablationsstrategie gewählt, da eine komplette Leitungserholung aller 4 Pulmonalvenen vorlag (Gruppe B). Alle Pulmonalvenen mit einem Leitungsrezidiv konnten erfolgreich reisoliert werden. Eine 3. oder 4. Ablationsprozedur wurde bei 4 (3/1) Patienten erforderlich (13,3 %). Während eines Nachbeobachtungszeitraums von 5 Jahren blieben 66,7 % der Patienten ohne Arrhythmierezidiv (20/30). Es traten keine schwerwiegenden Komplikationen im Langzeitverlauf auf.
Schlussfolgerung
Bei Patienten mit Vorhofflimmerrezidiven nach initial erfolgreicher Pulmonalvenenisolation mittels der Kryoballontechnik kann ein Revisionseingriff sicher und effektiv mittels der Radiohochfrequenz-Ablation durchgeführt werden. Hierdurch können gute Langzeitergebnisse erzielt werden.
Similar content being viewed by others

Abbreviations
- AF:
-
Atrial fibrillation
- CS:
-
Coronary sinus
- ECG:
-
Electrocardiogram
- LA:
-
Left atrium/left atrial
- PV(s):
-
Pulmonary vein(s)
- RF:
-
Energy applications = radiofrequency energy applications
- SD:
-
Standard deviation
- TEE:
-
Transesophageal echocardiography
- 3-D TEE reconstruction:
-
Three-dimensional TEE reconstruction
- TIA:
-
Transient ischemic attacks
References
Kettering K, Al-Ghobainy R, Wehrmann M, Vonthein R, Mewis C (2006) Atrial linear lesions: feasibility using cryoablation. Pacing Clin Electrophysiol 29:283–289
Oral H, Knight BP, Ozaydin M, Chugh A, Lai SW, Scharf C, Hassan S, Greenstein R, Han JD, Pelosi F, Strickberger SA, Morady F (2002) Segmental ostial ablation to isolate the pulmonary veins during atrial fibrillation: feasibility and mechanistic insights. Circulation 106(10):1256–1262
Haïssaguerre M, Shah DC, Jaïs P, Hocini M, Yamane T, Deisenhofer I, Garrigue S, Clémenty J (2000) Mapping-guided ablation of pulmonary veins to cure atrial fibrillation. Am J Cardiol 86(suppl.):9K–19K
Gerstenfeld EP, Guerra P, Sparks PB, Hattori K, Lesh MD (2001) Clinical outcome after radiofrequency catheter ablation of focal atrial fibrillation triggers. J Cardiovasc Electrophysiol 12(8):900–908
Marrouche NF, Dresing T, Cole C, Bash D, Saad E, Balaban K, Pavia SV, Schweikert R, Saliba W, Abdul-Karim A, Pisano E, Fanelli R, Tchou P, Natale A (2002) Circular mapping and ablation of the pulmonary vein for treatment of atrial fibrillation: impact of different catheter technologies. J Am Coll Cardiol 40(3):464–474
Swartz J, Pellersels G, Silvers J, Patten L, Cervantez D (1994) A catheter-based curative approach to atrial fibrillation in humans. Circulation 90(4.2):I-335
Haïssaguerre M, Jaïs P, Shah DC, Gencel L, Pradeau V, Garrigues S, Chouairi S, Hocini M, Le-Metayer P, Roudaut R, Clémenty J (1996) Right and left atrial radiofrequency catheter therapy of paroxysmal atrial fibrillation. J Cardiovasc Electrophysiol 7(12):1132–1144
Ernst S, Schluter M, Ouyang F, Khanedani A, Cappato R, Hebe J, Volkmer M, Antz M, Kuck KH (1999) Modification of the substrate for maintenance of idiopathic human atrial fibrillation: efficacy of radiofrequency ablation using nonfluoroscopic catheter guidance. Circulation 100(20):2085–2092
Jaïs P, Hocini M, Hsu LF, Sanders P, Scavee C, Weerasooriya R, Macle L, Raybaud F, Garrigue S, Shah DC, Le-Metayer P, Clémenty J, Haïssaguerre M (2004) Technique and results of linear ablation at the mitral isthmus. Circulation 110(19):2996–3002
Oral H, Chugh A, Lemola K, Cheung P, Hall B, Good E, Han J, Tamirisa K, Bogun F, Pelosi F, Morady F (2004) Noninducibility of atrial fibrillation as an end point of left atrial circumferential ablation for paroxysmal atrial fibrillation: a randomized study. Circulation 110(18):2797–2801
Avitall B, Helms RW, Koblish JB, Sieben W, Kotov AV, Gupta GN (1999) The creation of linear contiguous lesions in the atria with an expandable loop catheter. J Am Coll Cardiol 33(4):972–984
Mitchell MA, McRury ID, Haines DE (1998) Linear atrial ablations in a canine model of chronic atrial fibrillation: morphological and electrophysiological observations. Circulation 97(12):1176–1185
Schwartzman D, Kuck KH (1998) Anatomy-guided linear atrial lesions for radiofrequency catheter ablation of atrial fibrillation. Pacing Clin Electrophysiol 21(10):1959–1978
Ouyang F, Baensch D, Ernst S, Schaumann A, Hachiya H, Chen M, Chun J, Falk P, Khanedani A, Antz M, Kuck KH (2004) Complete isolation of the left atrium surrounding the pulmonary veins. New insights from the double-Lasso technique in paroxysmal atrial fibrillation. Circulation 110:2090–2096
Ouyang F, Antz M, Ernst S, Hachiya H, Mavrakis H, Deger FT, Schaumann A, Chun J, Falk P, Hennig D, Liu X, Baensch D, Kuck KH (2005) Recovered pulmonary vein conduction as a dominant factor for recurrent atrial tachyarrhythmias after complete circular isolation of the pulmonary veins. Lessons from double Lasso technique. Circulation 111:127–135
Ouyang F, Ernst S, Chun J, Baensch D, Li Y, Schaumann A, Mavrakis H, Liu X, Deger FT, Schmidt B, Xue Y, Cao J, Hennig D, Huang H, Kuck KH, Antz M (2005) Electrophysiological findings during ablation of persistent atrial fibrillation with electroanatomic mapping and double Lasso catheter technique. Circulation 112:3038–3048
Kettering K, Greil G, Fenchel M, Kramer U, Weig H, Busch M, Miller S, Sieverding L, Laszlo R, Schreieck J (2009) Catheter ablation of atrial fibrillation using the Navx-/Ensite-system and a CT-/MRI-guided approach. Clin Res Cardiol 98:285–296
Kettering K, Greil GF, Busch M, Miller S, Sieverding L, Schreieck J (2006) Catheter ablation of atrial fibrillation: ongoing atrial fibrillation inside a single pulmonary vein after successful electrical disconnection and restoration of sinus rhythm in both atria. Clin Res Cardiol 95:663–667
Kettering K, Weig H, Busch M, Laszlo R, Schreieck J (2008) Segmental pulmonary vein ablation: success rates with and without exclusion of areas adjacent to the esophagus. Pacing Clin Electrophysiol 31:652–659
Kettering K, Weig H, Busch M, Schneider K, Eick C, Weretka S, Laszlo R, Gawaz M, Schreieck S (2011) Catheter ablation of persistent atrial fibrillation: anatomically based circumferential pulmonary vein ablation in combination with a potential-guided segmental approach to achieve complete pulmonary vein isolation. J Interv Card Electrophysiol 30:63–72
Neumann T, Vogt J, Schumacher B, Dorszewski A, Kuniss M, Neuser H, Kurzidim K, Berkowitsch A, Koller M, Heintze J, Scholz U, Wetzel U, Schneider M, Horstkotte D, Hamm C, Pitschner H (2008) Circumferential pulmonary vein isolation with the cryoballoon technique. J Am Coll Cardiol 52:273–278
Lustgarten D, Keane D, Ruskin J (1999) Cryothermal ablation: mechanism of tissue injury and current experience in the treatment of tachyarrhythmias. Prog Cardiovasc Dis 41:481–498
Chierchia G, Namdar M, Sarkozy A, Sorgente A, de Asmundis C, Casado-Arroyo R, Capulzini L, Bayrak F, Rodriguez-Maňero M, Ricciardi D, Rao J, Overeinder I, Paparella G, Brugada P (2012) Verification of pulmonary vein isolation during single transseptal cryoballoon ablation: a comparison between the classical circular mapping catheter and the inner lumen mapping catheter. Europace. doi:10.1093/europace/eus189
Schmidt M, Dorwarth U, Straube F, Wankerl M, Krieg J, Leber A, Ebersberger H, Daccarett M, Huber A, Rummeny E, Hoffmann E (2012) A novel double cryoballoon strategy in persistent atrial fibrillation: a pilot study. Clin Res Cardiol 101:777–785
Calkins H, Kuck K, Cappato R, Brugada J, Camm A, Chen S, Crijns H, Damiano R, Davies D, Di Marco J, Edgerton J, Ellenbogen K, Ezekowitz M, Haines D, Haïssaguerre M, Hindricks G, Iesaka Y, Jackman W, Jalife J, Jais P, Kalman J, Keane D, Kim Y, Kirchhof P, Klein G, Kottkamp H, Kumagai K, Lindsay B, Mansour M, Marchlinski F, McCarthy P, Mont L, Morady F, Nademanee K, Nakagawa H, Natale A, Nattel S, Packer D, Pappone C, Prystowsky E, Raviele A, Reddy V, Ruskin J, Shemin R, Tsao H, Wilber D (2012) 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. J Interv Card Electrophysiol 33:171–257
Camm J, Lip G, De Caterina R, Savelieva I, Atar D, Hohnloser S, Hindricks G, Kirchhof P (2012) 2012 focused update of the ESC Guidelines for the management of atrial fibrillation. Eur Heart J. doi:10.1093/eurheartj/ehs253
Kettering K, Gramley F (2013) Catheter ablation of atrial fibrillation: radiofrequency catheter ablation for redo procedures after cryoablation. World J Cardiol 5(8):280–287
Ouyang F, Tilz R, Chun J, Schmidt B, Wissner E, Zerm T, Neven K, Köktürk B, Konstantinidou M, Metzner A, Fuernkranz A, Kuck KH (2010) Long-term results of catheter ablation in paroxysmal atrial fibrillation. Lessons from a 5-year follow-up. Circulation 122:2368–2377
Pandya B, Sheikh A, Spagnola J, Bekheit S, Lafferty J, Kowalski M (2016) Safety and efficacy of second-generation versus first-generation cryoballoons for treatment of atrial fibrillation: a meta-analysis of current evidence. J Interv Card Electrophysiol 45:49–56
Metzner A, Heeger C, Wohlmuth P, Reissmann B, Rillig A, Tilz R, Mathew S, Lemes C, Deiss S, Maurer T, Saguner A, Ouyang F, Kuck KH, Wissner E (2016) Two-year outcome after pulmonary vein isolation using the second-generation 28-mm cryoballoon: lessons from the bonus freeze protocol. Clin Res Cardiol 105:72–78
Straube F, Dorwarth U, Hartl S, Bunz B, Wankerl M, Ebersberger U, Hoffmann E (2016) Outcome of paroxysmal atrial fibrillation ablation with the cryoballoon using two different application times: the 4‑ versus 3‑min. protocol. J Interv Card Electrophysiol 45:169–177
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
K. Kettering and F. Gramley declare that they have no competing interests.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study. The study comprised a retrospective analysis of data obtained from clinically indicated routine procedures. There was no funding of the study.
Additional information
Both authors have made substantial contributions to the design of the study, to data evaluation and to drafting of the manuscript. They have approved the current version of the manuscript.
Rights and permissions
About this article

Cite this article
Kettering, K., Gramley, F. Radiofrequency catheter ablation for redo procedures after pulmonary vein isolation with the cryoballoon technique. Herzschr Elektrophys 28, 225–231 (2017). https://doi.org/10.1007/s00399-017-0493-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00399-017-0493-3