
Abstract
Objective
Growth hormone (GH) and insulin-like growth factor-1 (IGF-1) play a major role in bone homeostasis. In this study, we aimed to assess bone mineral density (BMD) in active acromegaly.
Materials and methods
A total of 29 patients with active acromegaly (age 46.10 ± 13.27 years; body mass index [BMI]: 29.51 ± 4.91 kg/m2) and 42 healthy individuals matched for age and BMI (age: 40.35 ± 11.74 years; BMI: 28.18 ± 7.35 kg/m2) were included in the study. BMD was measured by DXA.
Results
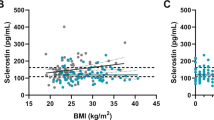
The mean levels of GH and IGF-1 were found to be 12.61 ± 11.34 ng/ml and 676.47 ± 316.19 ng/ml in acromegaly, respectively, while the mean levels of GH and IGF-1 were found to be 0.59 ± 0.81 ng/ml (p = 0.0001) and 178.17 ± 57.11 ng/ml (p = 0.0001) in the control group, respectively. Only total hip t‑score was determined to be significantly lower in acromegaly compared to the control group (p = 0.037). No significant differences were found between the other parameters in DXA and only a positive correlation was found between IGF-1 levels and L1–L4 BMD (r = 0.259, p = 0.029).
Conclusions
Although GH and IGF-1 levels were increased in acromegalic patients, no significant difference was found in terms of vertebral BMD. Only hip t‑scores were found to be lower in acromegalic patients, but this low hip t‑score did not reach the osteopenic level. The positive correlation between IGF-1 and lumbar vertebral BMD suggested a more prominent effect of IGF-1 on BMD compared to GH.
Zusammenfassung
Ziel
Wachtumshormon („growth hormone“, GH) und der insulinähnliche Wachstumsfaktor 1 („insulin-like growth factor 1“, IGF-1) spielen eine wichtige Rolle bei der Knochenhomöostase. Ziel dieser Studie war es, die Knochenmineraldichte („bone mineral density“, BMD) bei aktiver Akromegalie zu beurteilen.
Material und Methoden
Neunundzwanzig Patienten mit aktiver Akromegalie (Alter: 46,10 ± 13,27 Jahre; Body-Mass-Index [BMI]: 29,51 ± 4,91 kg/m2) und 42 gesunde Personen mit entsprechendem Alter und BMI (Alter: 40,35 ± 11,74 Jahre; BMI: 28,18 ± 7,35 kg/m2) wurden in die Studie eingeschlossen. Die BMD wurde mittels DXA gemessen.
Ergebnisse
Die mittleren GH- und IGF-1-Serumspiegel bei Akromegalie betrugen 12,61 ± 11,34 ng/ml bzw. 676,47 ± 316,19 ng/ml, während die mittleren GH- und IGF-1-Serumspiegel in der Kontrollgruppe bei 0,59 ± 0,81 ng/ml (p = 0,0001) bzw. 178,17 ± 57,11 ng/ml (p = 0,0001) lagen. Der T‑Score der Gesamthüfte war signifikant niedriger bei Akromegalie im Vergleich zur Kontrollgruppe (p = 0,037). Es wurden keine signifikanten Unterschiede zwischen den anderen DXA-Parametern gefunden, und zwischen den IGF-1-Serumspiegeln und der BMD in L1–L4 wurde lediglich eine positive Korrelation festgestellt (r = 0,259, p = 0,029).
Schlussfolgerungen
Obwohl bei Patienten mit Akromegalie erhöhte GH- und IGF-1-Serumspiegel festgestellt wurden, gab es keine Hinweise auf signifikante Unterschiede bezüglich der BMD der Wirbelsäule. Der T‑Score der Hüfte war bei Patienten mit Akromegalie niedriger. Diese niedrigen T‑Score-Werte der Hüfte erreichten jedoch kein osteopenisches Ausmaß. Die positive Korrelation zwischen IGF-1 und der BMD im Lendenwirbelsäulenbereich zeigte, dass IGF-1 im Vergleich zu GH eine größere Auswirkung auf die BMD hat.

Similar content being viewed by others

References
Melmed S (2009) Acromegaly pathogenesis and treatment. J Clin Invest 119(11):3189–3202
Rajasoorya C, Holdaway IM, Wrightson P et al (1994) Determinants of clinical outcome and survival in acromegaly. Clin Endocrinol (Oxf) 41:95–102
Ahmed SF, Farquharson C (2010) The effect of GH and IGF1 on linear growth and skeletal development and their modulation by SOCS proteins. J Endocrinol 206(3):249–259
Kasukawa Y, Miyakoshi N, Mohan S (2004) The anabolic effects of GH/IGF system on bone. Curr Pharm Des 10(21):2577–2592
Chihara K, Sugimoto T (1997) The action of GH/IGF-I/IGFBP in osteoblasts and osteoclasts. Horm Res 48(Suppl 5):45–49
Ueland T, Fougner SL, Godang K, Schreiner T, Bollerslev J (2006) Serum GH and IGF-I are significant determinants of bone turnover but not bone mineral density in active acromegaly: a prospective study of more than 70 consecutive patients. Eur J Endocrinol 155(5):709–715
DiGirolamo DJ, Mukherjee A, Fulzele K, Gan Y, Cao X, Frank SJ, Clemens TL (2007) Mode of growth hormone action in osteoblasts. J Biol Chem 282(43):31666–31674
Biermasz NR, Hamdy NA, Pereira AM, Romijn JA, Roelfsema F (2005) Long-term maintenance of the anabolic effects of GH on the skeleton in successfully treated patients with acromegaly. Eur J Endocrinol 152(1):53–60
White HD, Ahmad AM, Durham BH, Joshi AA, Fraser WD, Vora JP (2011) Effect of oral phosphate and alendronate on bone mineral density when given as adjunctive therapy to growth hormone replacement in adult growth hormone deficiency. J Clin Endocrinol Metab 96(3):726–736
Killinger Z, Kužma M, Sterančáková L, Payer J (2012) Osteoarticular changes in acromegaly. Int J Endocrinol 2012:Article ID 839282. doi:10.1155/2012/839282
Padova G, Borzì G, Incorvaia L, Siciliano G, Migliorino V, Vetri M, Tita P (2011) Prevalence of osteoporosis and vertebral fractures in acromegalic patients. Clin Cases Miner Bone Metab 8(3):37–43
Colao A, Ferone D, Marzullo P, Lombardi G (2004) Systemic complications of acromegaly: epidemiology, pathogenesis and management. Endocr Rev 25:102–152
Morselli LL, Manetti L, Cosci C et al (2006) Bone and joint alterations in acromegaly. J Orthop Traumatol 7:169–175
Ho PJ, Fig LM, Barkan AL, Shapiro B (1992) Bone mineral density of the axial skeleton in acromegaly. J Nucl Med 33(9):1608–1612
Kotzmann H, Bernecker P, Hübsch P, Pietschmann P, Woloszczuk W, Svoboda T, Geyer G, Luger A (1993) Bone mineral density and parameters of bone metabolism in patients with acromegaly. J Bone Miner Res 8(4):459–465
Scillitani A, Battista C, Chiodini I, Carnevale V, Fusilli S, Ciccarelli E, Terzolo M, Oppizzi G, Arosio M, Gasperi M, Arnaldi G, Colao A, Baldelli R, Ghiggi MR, Gaia D, Di Somma C, Trischitta V, Liuzzi A (2003) Bone mineral density in acromegaly: the effect of gender, disease activity and gonadal status. Clin Endocrinol (Oxf) 58(6):725–731
Katznelson L, Atkinson JL, Cook DM, Ezzat SZ, Hamrahian AH, Miller KK, AACE Acromegaly Task Force (2011) American Association of Clinical Endocrinologists medical guidelines for clinical practice for the diagnosis and treatment of acromegaly–2011 update: executive summary. Endocr Pract 17(4):636–646
Bolanowski M, Daroszewski J, Medraś M, Zadrozna-Sliwka B (2006) Bone mineral density and turnover in patients with acromegaly in relation to sex, disease activity, and gonadal function. J Bone Miner Metab 24(1):72–78
Giuseppina P, Graziella B, Laura I et al (2011) Prevalence of osteoporosis and vertebral fractures in acromegalic patients. Clin Cases Miner Bone Metab 8(3):37–43
Mazziotti G, Bianchi A, Bonadonna S, Cimino V, Patelli I, Fusco A, Pontecorvi A, De Marinis L, Giustina A (2008) Prevalence of vertebral fractures in men with acromegaly. J Clin Endocrinol Metab 93(12):4649–4655
Unnanuntana A, Gladnick BP, Donnelly E, Lane JM (2010) The assessment of fracture risk. J Bone Joint Surg Am 92(3):743–753
Bonadonna S, Mazziotti G, Nuzzo M, Bianchi A, Fusco A, De Marinis L, Giustina A (2005) Increased prevalence of radiological spinal deformities in active acromegaly: a cross-sectional study in postmenopausal women. J Bone Miner Res 20(10):1837–1844
Madeira M, Neto LV, de Paula Paranhos Neto F, Barbosa Lima IC, Carvalho de Mendonça LM, Gadelha MR, Fleiuss de Farias ML (2013) Acromegaly has a negative influence on trabecular bone, but not on cortical bone, as assessed by high-resolution peripheral quantitative computed tomography. J Clin Endocrinol Metab 98(4):1734–1741
Wassenaar MJ, Biermasz NR, Hamdy NA, Zillikens MC, van Meurs JB, Rivadeneira F, Hofman A, Uitterlinden AG, Stokkel MP, Roelfsema F, Kloppenburg M, Kroon HM, Romijn JA, Pereira AM (2011) High prevalence of vertebral fractures despite normal bone mineral density in patients with long-term controlled acromegaly. Eur J Endocrinol 164(4):475–483
Ezzat S, Melmed S, Endres D, Eyre DR, Singer FR (1993) Biochemical assessment of bone formation and resorption in acromegaly. J Clin Endocrinol Metab 76(6):1452–1457
Hübsch P, Kotzmann H, Svoboda T, Kainberger FM, Bankier A, Seidl G (1993) Bone density of the lumbar spine and femur in acromegaly. Radiologe 33(8):457–461
Jockenhövel F, Rohrbach S, Deggerich S, Reinwein D, Reiners C (1996) Differential presentation of cortical and trabecular peripheral bone mineral density in acromegaly. Eur J Med Res 1(8):377–382
Ueland T (2005) GH/IGF-I and bone resorption in vivo and in vitro. Eur J Endocrinol 152(3):327–332
Jean Ho P, Lorraine M, Barkan A, Shapiro B (1992) Bone mineral density of the axial skeleton in acromegaly. J Nucl Med 33:1608–1612
Wang Y, Nishida S, Elalieh HZ, Long RK, Halloran BP, Bikle DD (2006) Role of IGF-I signaling in regulating osteoclastogenesis. J Bone Miner Res 21(9):1350–1358
Neve A, Corrado A, Cantatore FP (2011) Osteoblast physiology in normal and pathological conditions. Cell Tissue Res 343(2):289–302
Yakar S, Courtland HW, Clemmons D (2010) IGF-1 and bone: new discoveries from mouse models. J Bone Miner Res 25(12):2543–2552
Bikle D, Majumdar S, Laib A, Powell-Braxton L, Rosen C, Beamer W, Nauman E, Leary C, Halloran B (2001) The skeletal structure of insulin-like growth factor I‑deficient mice. J Bone Miner Res 16(12):2320–2329
Bach LA (2004) The insulin-like growth factor system: towards clinical applications. Clin Biochem Rev 25(3):155–164
Garnero P, Sornay-Rendu E, Delmas PD (2000) Low serum IGF-1 and occurrence of osteoporotic fractures in postmenopausal women. Lancet 355(9207):898–899
Friedlander AL, Butterfield GE, Moynihan S, Grillo J, Pollack M, Holloway L, Friedman L, Yesavage J, Matthias D, Lee S, Marcus R, Hoffman AR (2001) One year of insulin-like growth factor I treatment does not affect bone density, body composition, or psychological measures in postmenopausal women. J Clin Endocrinol Metab 86(4):1496–1503
Perrini S, Laviola L, Carreira MC, Cignarelli A, Natalicchio A, Giorgino F (2010) The GH/IGF1 axis and signaling pathways in the muscle and bone: mechanisms underlying age-related skeletal muscle wasting and osteoporosis. J Endocrinol 205(3):201–210
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
S. Tuzcu, Ş.A. Durmaz, A. Carlıoglu, Z. Demircan, A. Tuzcu, C. Beyaz and A. Tay confirm that they have no conflict of interest.
Authors confirm that all procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Additional information
Redaktion
U. Müller-Ladner, Bad Nauheim
U. Lange, Bad Nauheim
Rights and permissions
About this article

Cite this article
Tuzcu, S., Durmaz, Ş.A., Carlıoğlu, A. et al. The effects of high serum growth hormone and IGF-1 levels on bone mineral density in acromegaly. Z Rheumatol 76, 716–722 (2017). https://doi.org/10.1007/s00393-016-0171-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00393-016-0171-6