
Abstract
Background
This observational study was carried out to investigate the effect of intravenous (i.v.) iron administration on the clinical symptoms of restless legs syndrome (RLS) in geriatric outpatients over 65 years old.
Methods
In this study geriatric outpatients (mean 4.5 ± 3.4 comorbidities and 5.7 ± 4.4 drugs taken) were recruited according to the following inclusion criteria: ≥ 65 years, diagnosis of RLS due to iron deficiency, i.e. ferritin < 50 µg/l or transferrin saturation (TFS) < 16 %) as well as no other iron therapy within 2 weeks prior to the study. Of the patients 7 (41 %) received 500 mg ferric carboxymaltose (FCM) and 10 patients (59 %) received iron gluconate (62.5 mg) based on the degree of iron deficiency. As assessed by the international RLS severity scale (IRLS) symptoms were recorded 3 times: at the beginning of iron therapy (t0), after 2 weeks (t1) and after 12 weeks (t2).
Results
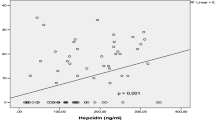
A total of 17 patients (13 female, 4 male, mean age 73.2 ± 5.9 years) were included. The IRLS score significantly improved in all patients as shown by an average decrease from 30.2 (± 4.3) to 20.2 (± 4.7) (p < 0.001) after 2 weeks of i.v. iron treatment and to 23.2 ± 6.6 (p < 0.001) after 12 weeks. There was a high correlation between ferritin values and the IRLS score (C 0.729, p < 0.001). The part of the IRLS referring to activities of daily living (ADL) improved from a median of 3 (scores 3–4) to 2 (scores 2–3, p = 0.001) after 2 weeks (effect size − 0.6).
Conclusion
In this study group of geriatric outpatients i.v. administration of iron was associated with a significant improvement of symptoms in RLS as assessed by the IRLS score 2 weeks after treatment. In geriatric patients with RLS associated with iron deficiency, i.v. iron administration should be considered regarding improvement of RLS symptoms and ADL.
Zusammenfassung
Hintergrund
Es wurde eine Beobachtungstudie zur Untersuchung der Wirkung der intravenösen (i.v.) Eisengabe auf die klinischen Symptome des Restless-legs-Syndroms (RLS) bei geriatrischen ambulanten Patienten über 65 Jahren durchgeführt.
Methoden
Eingeschlossen wurden Patienten (4,5 ± 3,4 Komorbiditäten, 5,7 ± 4,4 eingenommene Wirkstoffe) gemäß folgender Einschlusskriterien: ≥ 65 Jahre, Eisenmangel assoziiertes RLS (Ferritin < 50 µg/l oder Transferrinsättigung (TFS) < 16 %) sowie keine Eisengabe 2 Wochen vor Studieneinschluss. Sieben Patienten (41 %) erhielten 500 mg Eisencarboxymaltose (FCM) und 10 Patienten (59 %) erhielten Eisenglukonat (62,5 mg) basierend auf der Höhe des Eisenmangels. Mittels International RLS Severity Scale (IRLS), wurde der Schweregrad des RLS dreimal bewertet: zu Beginn der Eisengabe (t0), nach 2 Wochen (t1) und nach 12 Wochen (t2).
Ergebnisse
Siebzehn Patienten (13 weiblich, 4 männlich, mittleres Alter 73,2 ± 5,9 Jahre) wurden eingeschlossen. Der IRLS-Score verbesserte sich signifikant bei allen Patienten, basierend auf einer Abnahme des IRLS-Score von 30,2 (± 4,3) auf 20,2 (± 4,7) (p < 0,001) 2 Wochen nach der i.v. Eisenbehandlung und auf 23,2 ± 6,6 (p < 0,001) nach 12 Wochen. Der Schweregrad des RLS zeigte eine hohe Korrelation mit den gemessenen Ferritinwerten (C 0,729, p < 0,001). Der Teil des IRLS, welcher die Aktivitäten des täglichen Lebens (ADL) abbildet verbesserte sich im Median von 3 [3–4] auf 2 [2–3; p = 0,001)] nach 2 Wochen (Effektgröße − 0,6).
Schlussfolgerung
In diesem geriatrischen ambulanten Kollektiv ist eine i.v. Eisengabe mit einer signifikanten Besserung der RLS Symptome nach 2 Wochen verbunden. Bei geriatrischen Patienten mit Eisenmangel assoziiertem RLS sollte immer auch eine i.v. Eisengabe zur Besserung von RLS und ADL erwogen werden.



Similar content being viewed by others

References
Allen RP, Adler CH, Du W et al (2011) Clinical efficacy and safety of IV ferric carboxymaltose (FCM) treatment of RLS: a multi-centred, placebo-controlled preliminary clinical trial. Sleep Med 12(9):906–913
Allen RP, Ondo WG, Ball E et al (2011) Restless legs syndrome (RLS) augmentation associated with dopamine agonist and levodopa usage in a community sample. Sleep Med 12(5):431–439
Allen RP, Picchietti D, Hening WA et al (2003) Restless legs syndrome: diagnostic criteria, special considerations, and epidemiology. A report from the restless legs syndrome diagnosis and epidemiology workshop at the National Institutes of Health. Sleep Med 4(2):101–119
Berger K, Kurth T (2007) RLS epidemiology—frequencies, risk factors and methods in population studies. Mov Disord 22(Suppl 18):S420–S423
Bjerrum L, Gonzalez Lopez-Valcarcel B, Petersen G (2008) Risk factors for potential drug interactions in general practice. Eur J Gen Pract 14(1):23–29
Cankurtaran M, Yavuz BB, Halil M et al (2012) Increased ferritin levels could reflect ongoing aging-associated inflammation and may obscure underlying iron deficiency in the geriatric population. Eur Geriatr Med 3(5):277–280
Celle S, Roche F, Kerleroux J et al (2010) Prevalence and clinical correlates of restless legs syndrome in an elderly French population: the synapse study. J Gerontol A Biol Sci Med Sci 65A(2):167–173
Çurgunlu A, Döventaş A, Karadeniz D et al (2012) Prevalence and characteristics of restless legs syndrome (RLS) in the elderly and the relation of serum ferritin levels with disease severity: hospital-based study from Istanbul, Turkey. Arch Gerontol Geriatr 55(1):73–76
Davis BJ, Rajput A, Rajput ML et al (2000) A randomized, double-blind placebo-controlled trial of iron in restless legs syndrome. Eur Neurol 43(2):70–75
Earley CJ, Allen RP, Beard JL et al (2000) Insight into the pathophysiology of restless legs syndrome. J Neurosci Res 62(5):623–628
Earley CJ, Horska A, Mohamed MA et al (2009) A randomized, double-blind, placebo-controlled trial of intravenous iron sucrose in restless legs syndrome. Sleep Med 10(2):206–211
Frauscher B, Gschliesser V, Brandauer E et al (2009) The severity range of restless legs syndrome (RLS) and augmentation in a prospective patient cohort: association with ferritin levels. Sleep Med 10(6):611–615
Grote L, Leissner L, Hedner J, Ulfberg J. (2009) A randomized, double-blind, placebo controlled, multi-center study of intravenous iron sucrose and placebo in the treatment of restless legs syndrome. Mov Disord 24:1445–1452
Hamilton RA, Briceland LL, Andritz MH (1998) Frequency of hospitalization after exposure to known drug-drug interactions in a Medicaid population. Pharmacotherapy 18(5):1112–1120
Hornyak M, Scholz H, Kiemen A et al (2012) Investigating the response to intravenous iron in restless legs syndrome: an observational study. Sleep Med 13(6):732–735
Hornyak M, Scholz H, Kohnen R et al (2014) What treatment works best for restless legs syndrome? Meta-analyses of dopaminergic and non-dopaminergic medications. Sleep Med Rev 18(2):153–164
Mizuno S, Mihara T, Miyaoka T, Inagaki T, Horiguchi J. (2005) CSF iron, ferritin and transferrin levels in restless legs syndrome. J Sleep Res 14(1):43–47
Röhrig G, Doehner W, Schaefer RM et al (2012) Anämie und Eisenmangel in der Geriatrie. Prävalenz, Diagnostik und neue Therapieoptionen (Anemia and iron deficiency in the elderly. Prevalence, diagnostics and new therapeutic options). Z Gerontol Geriatr 45(3):191–196
Trenkwalder C, Högl B, Benes H et al (2008) Augmentation in restless legs syndrome is associated with low ferritin. Sleep Med 9(5):572–574
Trenkwalder C, Kohnen R, Allen RP et al (2007) Clinical trials in restless legs syndrome—recommendations of the European RLS Study Group (EURLSSG). Mov Disord 22(Suppl 18):S495–S504
Trotti LM, Bhadriraju S, Becker LA (2012) Iron for restless legs syndrome. Cochrane Database Syst Rev 5:CD007834
Walters AS, LeBrocq C, Dhar A et al (2003) Validation of the International Restless Legs Syndrome Study Group rating scale for restless legs syndrome. Sleep Med 4(2):121–132
Wang J, O’Reilly B, Venkataraman R et al (2009) Efficacy of oral iron in patients with restless legs syndrome and a low-normal ferritin: a randomized, double-blind, placebo-controlled study. Sleep Medicine 10(9):973–975
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
G. Roehrig and R. J. Schulz have received honoraria for academic lectures from viforpharma. J. Kassubek has received personal compensation for activities with UCB Pharma, GlaxoSmithKline, Teva, Medtronic and Boehringer Ingelheim Pharmaceuticals as a consultant and honoraria for academic lectures from Merz and Bayer. M. C. Polidori, I. Becker and B. Lieske declare that there are no conflicts of interest.
The study was approved by the local ethics committees of the University Hospital Cologne (reference nr. 12–273) and the University of Ulm (reference nr. 309/13). All included patients gave written informed consent to participate.
Rights and permissions
About this article

Cite this article
Lieske, B., Becker, I., Schulz, R. et al. Intravenous iron administration in restless legs syndrome. Z Gerontol Geriat 49, 626–631 (2016). https://doi.org/10.1007/s00391-015-0984-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00391-015-0984-y