
Abstract
Introduction
Focal therapy can offer the middle ground for treatment between active surveillance and radical therapy in patients with low- and intermediate-risk prostate cancer. Factors that prohibit focal therapy from being standard of care are numerous. Several consensus projects have been conducted to position the utilization of imaging and trial design in focal therapy. However, the literature is still scarce on patient follow-up after focal therapy. For these reasons, an international multidisciplinary consensus project was established in order to reach consensus about a uniform follow-up protocol after focal therapy.
Objective
To standardize patient follow-up after focal therapy.
Materials and methods
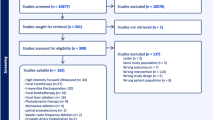
A literature study was performed, and a questionnaire was constructed. The questionnaire was sent out to 76 participants (70 % urologists, 28 % radiologists and 2 % biomedical engineers) in three consecutive rounds according to the Delphi method. In each round, the panelists were presented with the results of the previous round. Participants each had the opportunity to adapt, delete or add questions. The topics discussed pertaining to follow-up after focal therapy were as follows: (1) general,(2) biopsies, (3) PSA, (4) digital rectal examination (DRE), (5) imaging, (6) quality of life (QoL) and (7) registration and pooling of data. The project was concluded with a face-to-face meeting in which final conclusions were formulated.
Results
The follow-up after focal therapy should be a minimum of 5 years. The following modalities should be included in assessing post-treatment outcomes: multiparametric MRI (mpMRI), biopsies, assessment of erectile function, QoL, urinary symptoms and incontinence. A systematic 12-core TRUS biopsy combined with 4–6 targeted biopsy cores of the treated area and any suspicious lesion(s) should be performed after 1 year, and thereafter only when there is suspicion on imaging. The ideal way to perform targeted biopsies is to use TRUS–MRI fusion technology. PSA should be performed for research purposes, in the first year, every 3 months, and after the first year, every 6 months. mpMRI is the optimal imaging modality for follow-up after focal therapy. On a 1.5T scanner, an endorectal coil is strongly advised by the panel, whereas on a 3T machine, it is optional, however, it will improve image quality. The following sequences should be included: T2WI, DWI including high b values of >1,000 and ADC maps of DWI, DCE and T1WI. Imaging should be performed at 6 months and at 1 year following treatment; after the first year post-treatment, it should be performed every year until 5 years following treatment. All data should ideally be pooled in a common global database.
Conclusion
Focal therapy is a relatively new form of treatment for prostate cancer. In order to include focal therapy as a standard of care treatment, consistent follow-up is necessary. By implementing the results of this consensus study, focal therapy users will be able to provide important and standardized outcome data.

Similar content being viewed by others


Notes
Participants of the meeting B. G. Muller, M. Brausi, J. J. Fütterer, S. Ghai, P. A. Pinto, I. V. Popeneciu, T. M. de Reijke, C. Robertson, S. Scionti, H. Wijkstra, O. Ukimura and T. J. Polascik.
References
Valerio M et al (2014) The role of focal therapy in the management of localised prostate cancer: a systematic review. Eur Urol 66(4):732–751
Ahmed HU et al (2012) Transatlantic Consensus Group on active surveillance and focal therapy for prostate cancer. BJU Int 109(11):1636–1647
Cordeiro ER et al (2012) High-intensity focused ultrasound (HIFU) for definitive treatment of prostate cancer. BJU Int 110(9):1228–1242
Heidenreich A et al (2014) EAU guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent-update 2013. Eur Urol 65(1):124–137
Tsivian M, Polascik TJ (2010) Focal cryotherapy for prostate cancer. Curr Urol Rep 11(3):147–151
Oto A et al (2013) MR imaging-guided focal laser ablation for prostate cancer: phase I trial. Radiology 267(3):932–940
Garcia MAB, Gimeno AV, Cruz JF (2007) Radiofrequency interstitial tumor ablation (RITA) for the treatment of localised prostate cancer. Actas Urol Esp 31(6):627–632
Valerio M et al (2014) Initial assessment of safety and clinical feasibility of irreversible electroporation in the focal treatment of prostate cancer. Prostate Cancer Prostatic Dis 17(4):343–347
Moore CM et al (2014) Determination of optimal drug dose and light dose index to achieve minimally invasive focal ablation of localized prostate cancer using WST11-vascular targeted photodynamic (VTP) therapy. BJU Int. doi:10.1111/bju.12816
Kovacs G, Cosset JM, Carey B (2014) Focal radiotherapy as focal therapy of prostate cancer. Curr Opin Urol 24(3):231–235
de la Rosette J et al (2010) Focal therapy in prostate cancer-report from a consensus panel. J Endourol 24(5):775–780
Dickinson L et al (2011) Magnetic resonance imaging for the detection, localisation, and characterisation of prostate cancer: recommendations from a European consensus meeting. Eur Urol 59(4):477–494
Muller BG et al (2014) Role of multiparametric magnetic resonance imaging (MRI) in focal therapy for prostate cancer: a Delphi consensus project. BJU Int 114(5):698–707. doi:10.1111/bju.12548
van den Bos W et al (2014) Focal therapy in prostate cancer: international multidisciplinary consensus on trial design. Eur Urol 65(6):1078–1083
Linstone HA, Turoff M (1975) The Delphi method: techniques and applications. Addison-Wesley, London
Stewart J et al (1999) Identifying appropriate tasks for the preregistration year: modified Delphi technique. BMJ 319(7204):224–229
Williams PL, Webb C (1994) The Delphi technique: a methodological discussion. J Adv Nurs 19:180–186. doi:10.1111/j.1365-2648.1994.tb01066.x
Collins GN et al (1997) The effect of digital rectal examination, flexible cystoscopy and prostatic biopsy on free and total prostate specific antigen, and the free-to-total prostate specific antigen ratio in clinical practice. J Urol 157(5):1744–1747
Yuan JJ et al (1992) Effects of rectal examination, prostatic massage, ultrasonography and needle biopsy on serum prostate specific antigen levels. J Urol 147(3 Pt 2):810–814
Biermann K et al (2010) Histopathological findings after treatment of prostate cancer using high-intensity focused ultrasound (HIFU). Prostate 70(11):1196–1200
Oesterling JE et al (1993) Effect of cystoscopy, prostate biopsy, and transurethral resection of prostate on serum prostate-specific antigen concentration. Urology 42(3):276–282
Hamoen EH et al (2014) Measuring health-related quality of life in men with prostate cancer: a systematic review of the most used questionnaires and their validity. Urol Oncol. doi:10.1016/j.urolonc.2013.10.005
Penson DF, Litwin MS, Aaronson NK (2003) Health related quality of life in men with prostate cancer. J Urol 169(5):1653–1661
Esper P et al (1997) Measuring quality of life in men with prostate cancer using the functional assessment of cancer therapy-prostate instrument. Urology 50(6):920–928
Rosen RC, Cappelleri JC, Gendrano N 3rd (2002) The International Index of Erectile Function (IIEF): a state-of-the-science review. Int J Impot Res 14(4):226–244
Conflict of interest
The following authors declare no conflict of interest: B.G. Muller, W. van den Bos, M. Brausi, J.J. Fütterer, S. Ghai, P.A. Pinto, I.V. Popeneciu, T.M. de Reijke, B. Turkbey and H. Wijkstra. C. Robertson is consultant/PI at EDAP TMS Inc., S. Scionti is consultant at SonaCare Medical, T.J. Polascik receives a research grant from Endocare, O. Ukimura is advisory board member at SonaCare Medical, J.J.M.C.H. and de la Rosette is consultant to AngioDynamics.
Ethical standard
The manuscript does not contain clinical studies or patient data.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Muller, B.G., van den Bos, W., Brausi, M. et al. Follow-up modalities in focal therapy for prostate cancer: results from a Delphi consensus project. World J Urol 33, 1503–1509 (2015). https://doi.org/10.1007/s00345-014-1475-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-014-1475-2