
Abstract
Background
Enhanced recovery after surgery (ERAS) pathways represent the optimal approach for patients undergoing colorectal surgery. Elderly or low physical status patients have been often excluded from ERAS pathways because considered at high risk. The aim of this study is to assess the adherence to ERAS protocol and its impact on short-term postoperative outcome in patients with different surgical risk undergoing elective colorectal resection.
Methods
Prospectively collected data entered in an electronic Italian registry specifically designed for ERAS were reviewed. Patients were divided into four groups according to age (70-year-old cutoff) and preoperative physical status as measured by the ASA grade (I–II vs. III–IV). Adherence to 18 ERAS elements and postoperative outcomes were compared between groups. Regression analysis was used to identify independent factors associated with improved outcomes.
Results
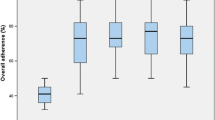
Eleven Italian hospitals reported data on 706 patients undergoing elective colorectal surgery within an ERAS protocol. Patients with low physical status had reduced adherence to preoperative carbohydrate loading, epidural analgesia, PONV prophylaxis, and early urinary catheter removal. No difference was found between groups for adherence to other perioperative elements. Major complications occurred in 37 (5.2 %) patients without significant differences among groups (p = 0.384). Median (IQR) time to readiness for discharge (TRD) was 4 (3–6) days, length of hospital stay (LOS) was 6 (4–7) days, and both were significantly shorter by only 1 day in the groups of younger patients (p < 0.001). At multivariate analysis, laparoscopy increased adherence to ERAS items and reduced TRD, LOS, and morbidity. A high ASA grade was significantly associated with lower adherence, whereas older age significantly prolonged TRD and LOS.
Conclusion
ERAS pathway can be safely applied in elderly and low physical status patients yielding slight differences in postoperative morbidity and time to recover. Laparoscopy was independently associated with increased adherence to ERAS protocol and improved short-term postoperative outcome.
Similar content being viewed by others

References
Tan KY, Kawamura YJ, Tokomitsu A, Tang T (2012) Assessment for frailty is useful for predicting morbidity in elderly patients undergoing colorectal cancer resection whose comorbidities are already optimized. Am J Surg 204:139–143
Marusch F, Koch A, Schmidt U et al (2005) The impact of the risk factor ‘age’ on the early postoperative results of surgery for colorectal carcinoma and its significance for perioperative management. World J Surg 29:1013–1021
Veenhof AAFA, Vlug MS, Van Der Pas MHGM et al (2012) Surgical stress response and postoperative immune function after laparoscopy or open surgery with fast track or standard perioperative care: a randomized trial. Ann Surg 255:216–221
Spanjersberg WR, Reurings J, Keus F et al (2011) Fast track surgery versus conventional recovery strategies for colorectal surgery. Cochrane Database Syst Rev 16:CD007635
Varadhan KK, Neal KR, Dejong CH et al (2010) The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clin Nutr 29:434–440
Greco M, Capretti G, Beretta L et al (2014) Enhanced recovery program in colorectal surgery: a meta-analysis of randomized controlled trials. World J Surg 38:1531–1541
Sammour T, Zargar-Shoshtari K, Bhat A et al (2010) A programme of Enhanced Recovery After Surgery (ERAS) is a cost-effective intervention in elective colonic surgery. N Z Med J 123:61–70
Roulin D, Donadini A, Gander S et al (2013) Cost-effectiveness of the implementation of enhanced recovery protocol for colorectal surgery. Br J Surg 100:1108–1114
Lyon A, Payne C, MacKay GJ (2012) Enhanced recovery programme in colorectal surgery: does one size fit all? World J Gastroenterol 18:5661–5663
Bagnall NM, Malietzis G, Kennedy RH et al (2014) A systematic review of enhanced recovery care after colorectal surgery in elderly patients. Colorectal Dis 16:947–956
von Elm E, Altman DG, Egger M et al (2007) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370:1453–1457
Fiore JF, Faragher IG, Bialocerkowski A et al (2013) Time to readiness for discharge is a valid and reliable measure of short-term recovery after colorectal surgery. World J Surg 37:2927–2934
Bozzetti F, Braga M, Gianotti L et al (2001) Postoperative enteral versus parenteral nutrition in malnourished patients with gastrointestinal cancer: a randomised multicentre trial. Lancet 358:1487–1492
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Faiz O, Haji A, Bottle A et al (2011) Elective colonic surgery for cancer in the elderly: an investigation into postoperative mortality in English NHS hospitals between 1996 and 2007. Colorectal Dis 13:779–785
Heriot AG, Tekkis PP, Smith JJ et al (2006) Prediction of postoperative mortality in elderly patients with colorectal cancer. Dis Colon Rectum 29:816–824
ERAS Compliance Group (2015) The impact of enhanced recovery protocol compliance on elective colorectal cancer resection. Results from an International Registry. Ann Surg 261:1153–1159
Khoo CK, Vickery CJ, Forsyth N et al (2007) A prospective randomized controlled trial of multimodal perioperative management protocol in patients undergoing elective colorectal resection for cancer. Ann Surg 245:867–872
Muller S, Zalunardo MP, Hubner M et al (2009) A fast-track program reduces complications and length of stay after open colonic surgery. Gastroenterology 136:842–847
Feroci F, Lenzi E, Baraghini M et al (2013) Fast-track surgery in real life: how patient factors influence outcomes and compliance with an enhanced recovery clinical pathway after colorectal surgery. Surg Laparosc Endosc Percutaneous Techn 23:259–265
Beak SJ, Kim SH, Kim SY et al (2013) The safety of a “fast-track” program after laparoscopic colorectal surgery is comparable in older patients as in younger patients. Surg Endosc 27:1225–1232
Basse L, Jakobsen DH, Bardram L et al (2005) Functional recovery after open versus laparoscopic colonic resection. Ann Surg 241:416–423
Gatt M, Anderson ADG, Reddy BS et al (2005) Randomized clinical trial of multimodal optimization of surgical care in patients undergoing major colonic resection. Br J Surg 92:1354–1362
Pecorelli N, Hershorn O, Baldini G et al (2016) Impact of adherence to care pathway interventions on recovery following bowel resection within an established enhanced recovery program. Surg Endosc. doi:10.1007/s00464-016-5169-2
Vlug MS, Wind J, Hollmann MW et al (2011) Laparoscopy in combination with fast track multimodal management is the best perioperative strategy in patients undergoing colonic surgery. Ann Surg 254:868–875
Kennedy RH, Francis EA, Wharton R et al (2014) Multicenter randomized controlled trial of conventional vs. laparoscopic surgery for colorectal cancer within an enhanced recovery program: EnROL. J Clin Oncol 32:1804–1811
Haines KJ, Skinner EH, Berney S (2013) Association of postoperative pulmonary complications with delayed mobilisation following major abdominal surgery: an observational cohort study. Physiotherapy 99:119–125
Zaouter C, Kaneva P, Carli F (2009) Less urinary tract infection by earlier removal of bladder catheter in surgical patients receiving thoracic epidural analgesia. Reg Anesth Pain Med 34:542–548
PeriOperative Italian Society collaborative members
Luigi Beretta MD (Department of Anesthesiology, Vita-Salute University San Raffaele Hospital, Milan), Stefano Bona MD (Department of Surgery, Humanitas Hospital IRCCS, Milan), Roberta Monzani MD (Department of Surgery, Humanitas Hospital IRCCS, Milan), Marco Azzola MD (Department of Surgery, Cantù Hospital), Andrea Muratore MD (Department of Surgery, Candiolo Hospital, Turin), Michele Crespi MD (Department of Surgery, Luigi Sacco Hospital, Milan), Riccardo Iuliani MD (Department of Surgery, Cottolengo Hospital Turin), Carlo Bima MD (Department of Surgery, Cottolengo Hospital Turin), Hedayat Bouzari MD (Department of Surgery, Mauriziano Hospital Turin), Andrea Pisani Ceretti MD (Department of Surgery, San Paolo Hospital), Luca Pellegrino MD (Department of Surgery, Cuneo Hospital), Marianna Maspero (Department of Surgery, Vita-Salute University San Raffaele Hospital, Milan), Umberto Casiraghi (Department of Surgery, Vita-Salute University San Raffaele Hospital, Milan), Ferdinando Ficari MD (Department of Surgery, Careggi Hospital, University of Florence).
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
About this article

Cite this article
Braga, M., Pecorelli, N., Scatizzi, M. et al. Enhanced Recovery Program in High-Risk Patients Undergoing Colorectal Surgery: Results from the PeriOperative Italian Society Registry. World J Surg 41, 860–867 (2017). https://doi.org/10.1007/s00268-016-3766-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-016-3766-9