
Abstract
Background
Few studies in the literature have reported recovery data for different types of recurrent laryngeal nerve injuries (RLNIs). This study is the first attempt to classify RLNIs and rank them by severity.
Methods
This prospective clinical study analyzed 281 RLNIs in which a true loss of signal was identified by intraoperative neuromonitoring (IONM), and vocal cord palsy (VCP) was confirmed by a postoperative laryngoscope. For each injury type, the prevalence of VCP, the time of VCP recovery, and physical changes on nerves were analyzed. Additionally, different RLNI types were experimentally induced in a porcine model to compare morphological change.
Results
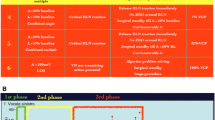
The overall VCP rate in at-risk patients/nerves was 8.9/4.6 %, respectively. The distribution of RLNI types, in order of frequency, was traction (71 %), thermal (17 %), compression (4.2 %), clamping (3.4 %), ligature entrapment (1.6 %), suction (1.4 %), and nerve transection (1.4 %). Complete recovery from VCP was documented in 91 % of RLNIs. Recovery time was significantly faster in the traction group compared to the other groups (p < 0.001). The rates of temporary and permanent VCP were 98.6 and 1.4 % for traction lesion, 72 and 28 % for thermal injury, 100 and 0 % for compression injury, 50 and 50 % for clamping injury, 100 and 0 % for ligature entrapment, 100 and 0 % for suction injury, and 0 and 100 % for nerve transection, respectively. Physical changes were noted in 14 % of RLNIs in which 56 % of VCP was permanent. However, among the remaining 86 % IONM-detectable RLNIs without physical changes, only 1.2 % of VCP was permanent. A porcine model of traction lesion showed only distorted outer nerve structure, whereas the thermal lesion showed severe damage in the inner endoneurium.
Conclusions
Different RNLIs induce different morphological alterations and have different recovery outcomes. Permanent VCP is rare in lesions that are visually undetectable but detectable by IONM. By enabling early detection of RLNI and prediction of outcome, IONM can help clinicians plan intra- and postoperative treatment.


Similar content being viewed by others


References
Randolph GW (2013) Surgery of the thyroid and parathyroid glands. Saunders, Philadelphia
Chiang FY, Lu IC, Kuo WR, Lee KW, Chang NC, Wu CW (2008) The mechanism of recurrent laryngeal nerve injury during thyroid surgery–the application of intraoperative neuromonitoring. Surgery 143(6):743–749
Snyder SK, Lairmore TC, Hendricks JC, Roberts JW (2008) Elucidating mechanisms of recurrent laryngeal nerve injury during thyroidectomy and parathyroidectomy. J Am Coll Surg 206(1):123–130
Chiang FY, Lee KW, Chen HC, Chen HY, Lu IC, Kuo WR, Hsieh MC, Wu CW (2010) Standardization of intraoperative neuromonitoring of recurrent laryngeal nerve in thyroid operation. World J Surg 34(2):223–229
Randolph GW, Dralle H, Abdullah H, Barczynski M, Bellantone R, Brauckhoff M, Carnaille B, Cherenko S, Chiang FY, Dionigi G, Finck C, Hartl D, Kamani D, Lorenz K, Miccolli P, Mihai R, Miyauchi A, Orloff L, Perrier N, Poveda MD, Romanchishen A, Serpell J, Sitges-Serra A, Sloan T, Van Slycke S, Snyder S, Takami H, Volpi E, Woodson G (2011) Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. Laryngoscope 121(Suppl 1):S1–S16
Dralle H, Sekulla C, Lorenz K, Brauckhoff M, Machens A (2008) Intraoperative monitoring of the recurrent laryngeal nerve in thyroid surgery. World J Surg 32(7):1358–1366
Dionigi G, Barczynski M, Chiang FY, Dralle H, Duran-Poveda M, Iacobone M, Lombardi CP, Materazzi G, Mihai R, Randolph GW, Sitges-Serra A (2010) Why monitor the recurrent laryngeal nerve in thyroid surgery? J Endocrinol Invest 33(11):819–822. doi:10.1007/bf03350349
Dionigi G, Alesina PF, Barczynski M, Boni L, Chiang FY, Kim HY, Materazzi G, Randolph GW, Terris DJ, Wu CW (2012) Recurrent laryngeal nerve injury in video-assisted thyroidectomy: lessons learned from neuromonitoring. Surg Endosc 26(9):2601–2608
Wu CW, Chai YJ, Dionigi G, Chiang FY, Liu X, Sun H, Randolph GW, Tufano RP, Kim HY (2015) Recurrent laryngeal nerve safety parameters of the harmonic focus during thyroid surgery: porcine model using continuous monitoring. Laryngoscope 125(12):2838–2845. doi:10.1002/lary.25412
Wu CW, Dionigi G, Sun H, Liu X, Kim HY, Hsiao PJ, Tsai KB, Chen HC, Chen HY, Chang PY, Lu IC, Chiang FY (2014) Intraoperative neuromonitoring for the early detection and prevention of RLN traction injury in thyroid surgery: a porcine model. Surgery 155(2):329–339
Lin YC, Dionigi G, Randolph GW, Lu IC, Chang PY, Tsai SY, Kim HY, Lee HY, Tufano RP, Sun H, Liu X, Chiang FY, Wu CW (2015) Electrophysiologic monitoring correlates of recurrent laryngeal nerve heat thermal injury in a porcine model. Laryngoscope 125(8):E283–E290. doi:10.1002/lary.25362
Puram SV, Chow H, Wu CW, Heaton JT, Kamani D, Gorti G, Chiang FY, Dionigi G, Barczynski M, Schneider R, Dralle H, Lorenz K, Randolph GW (2015) Vocal cord paralysis predicted by neural monitoring electrophysiologic changes with recurrent laryngeal nerve compressive neuropraxic injury in a canine model. Head Neck. doi:10.1002/hed.24225
Dionigi G, Bacuzzi A, Boni L, Rovera F, Dionigi R (2008) What is the learning curve for intraoperative neuromonitoring in thyroid surgery? Int J Surg 6(Suppl 1):S7–12
Dralle H, Sekulla C, Lorenz K, Thanh PN, Schneider R, Machens A (2012) Loss of the nerve monitoring signal during bilateral thyroid surgery. Br J Surg 99(8):1089–1095
Dionigi G, Chiang FY, Hui S, Wu CW, Xiaoli L, Ferrari CC, Mangano A, Lianos GD, Leotta A, Lavazza M, Frattini F, Annoni M, Rausei S, Boni L, Kim HY (2015) Continuous intraoperative neuromonitoring (C-IONM) technique with the automatic periodic stimulating (APS) accessory for conventional and endoscopic thyroid surgery. Surg Technol Int 26:101–114
Dionigi G, Boni L, Rovera F, Rausei S, Castelnuovo P, Dionigi R (2010) Postoperative laryngoscopy in thyroid surgery: proper timing to detect recurrent laryngeal nerve injury. Langenbeck’s Arch Surg 395(4):327–331. doi:10.1007/s00423-009-0581-x
Dionigi G (2009) Energy based devices and recurrent laryngeal nerve injury: the need for safer instruments. Langenbeck’s Arch Surg 394(3):579–580 author reply 581-576
Wang LF, Lee KW, Kuo WR, Wu CW, Lu SP, Chiang FY (2006) The efficacy of intraoperative corticosteroids in recurrent laryngeal nerve palsy after thyroid surgery. World J Surg 30(3):299–303
Bacuzzi A, Dralle H, Randolph GW, Chiang FY, Kim HY, Barczynski M, Dionigi G (2015) Safety of continuous intraoperative neuromonitoring (C-IONM) in thyroid surgery. World J Surg. doi:10.1007/s00268-015-3288-x
Phelan E, Schneider R, Lorenz K, Dralle H, Kamani D, Potenza A, Sritharan N, Shin J, Randolph WG (2014) Continuous vagal IONM prevents recurrent laryngeal nerve paralysis by revealing initial EMG changes of impending neuropraxic injury: a prospective, multicenter study. Laryngoscope 124(6):1498–1505. doi:10.1002/lary.24550
Schneider R, Bures C, Lorenz K, Dralle H, Freissmuth M, Hermann M (2013) Evolution of nerve injury with unexpected EMG signal recovery in thyroid surgery using continuous intraoperative neuromonitoring. World J Surg 37(2):364–368
Acknowledgments
The animal experiments in this study were supported by grants from the Kaohsiung Medical University Hospital (KMUH 103-3T07, 103-3R36) and the Ministry of Science and Technology, Taiwan. (MOST 103-2314-B-037-037- MY2).The authors are grateful to Dr. Pao-Chu Hun (Veterinarian, Laboratory Animal Center, KMU), Dr. Pi-Ying Chang, Dr. I-Cheng Lu (Anesthesiologists, KMUH), and Dr. Kuo-Bow Tsai (Pathologist, KMU) for their valuable technical assistance.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors have no other funding, financial relationships, or conflicts of interest to disclose.
Rights and permissions
About this article

Cite this article
Dionigi, G., Wu, CW., Kim, H.Y. et al. Severity of Recurrent Laryngeal Nerve Injuries in Thyroid Surgery. World J Surg 40, 1373–1381 (2016). https://doi.org/10.1007/s00268-016-3415-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-016-3415-3