
Abstract
Background
Two recent meta-analyses of mostly retrospective studies have shown high recurrence rates following subtotal resection of bilateral multinodular goiter. Therefore, many endocrine centers have changed their operative procedures in favor of thyroidectomy. Consequently, the rate of complications, especially hypoparathyroidism, has increased. Hemithyroidectomy plus subtotal resection (Dunhill operation) overcomes some disadvantages of bilateral subtotal resection (BST). We performed a prospective, randomized trial to compare the Dunhill operation (DO) and BST for benign goiters.
Methods
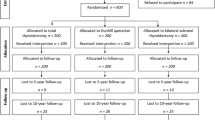
Between October 1994 and March 1997, a total of 200 consecutive patients were randomized into two study groups. Primary outcome measure was the incidence of recurrent goiter. Secondary outcome measures were incidence of recurrent nerve palsy and hypoparathyroidism. In all patients, ultrasonography of the thyroid and measurement of serum calcium and parathyroid hormone were performed. Recurrent nerve function was analyzed by indirect laryngoscopy. Long term data (>10 years after surgery) were available in 70 DO patients and 65 BST patients. Mean follow-up was 11.3 ± 4.2 years (10–12 years).
Results
No differences were seen in the operating times, transient and permanent hypoparathyroidism, or recurrent nerve palsy. In the long-term, mean thyroid volumes were significantly lower in the DO group (3.5 ± 3.5 vs. 6.4 ± 6.5 ml, p = 0.01). One reoperation was required in the BST group because of recurrence versus none in the DO group. 68 of 70 (97 %) patients in group DO and 59 of 65 (91 %) in group BST had ongoing thyroid hormone therapy with no significant differences in mean dosages of l-thyroxine.
Conclusions
The Dunhill operation and BST are safe procedures. In case of small remnants, clinically significant recurrence is a rare event especially after the Dunhill operation.
Similar content being viewed by others

References
Röher HD (1999) Ansprüche zeitgemäß problemorientierter Schilddrüsenchirurgie. Chirurg 70:969–970
Bay V, Engel U (1980) Komplikationen bei Schilddrüsenoperationen. Chirurg 51:91–98
Moalem J, Suh I, Duh QY (2008) Treatment and prevention of recurrence of multinodular goitre: an evidence based review of the literature. World J Surg 32:1301–1312. doi:10.1007/s00268-008-9477-0
Musholt TJ (2010) Totale Thyreoidektomie bei Knotenstruma. Chirurg 81:603–611
Barczynski M, Konturek A, Hubalewski-Dydejczyk A et al (2010) Five-year follow up of a randomized clinical trial of total thyroidectomy versus Dunhill operation versus bilateral subtotal thyroidectomy for multinodular nontoxic goiter. World J Surg 34:1203–1213. doi:10.1007/s00268-010-0491-7
Thomusch O, Machens A, Sekulla C et al (2003) The impact of surgical technique on postoperative hypoparathyroidism in bilateral thyroid surgery: a multivariate analysis of 5846 consecutive patients. Surgery 133:180–185
Agarwal G, Agarwal V (2008) Is total thyroidectomy the surgical procedure of choice for benign multinodular goiter? An evidence-based review. World J Surg 32:1313–1324. doi:10.1007/s00268-008-9579-8
Lennquist S (1987) The thyroid nodule: diagnosis and surgical treatment. Surg Clin North Am 67:213–232
Steinmüller T, Ulrich F, Rayes N et al (2001) Different surgical approaches and risk factors in the therapy of benign multinodular goiter: a comparison of complication rates. Chirurg 72:1453–1457
Klein E, Kracht J, Krüskemper HL et al (1974) Sektion der deutschen Gesellschaft für Endokrinologie: epidemiologische Einteilung der endemischen Struma. Dtsch Med Wochenschr 99:299
Liu Q, Djuricin G, Prinz A (1998) Total thyroidectomy for benign thyroid disease. Surgery 123:2–7
Delbridge L, Guinea AI, Reeve TS (1999) Total thyroidectomy for bilateral benign multinodular goiter: effect of changing practice. Arch Surg 134:1389–1393
Pappalardo G, Guadalaxara A, Frattaroli FM et al (1998) Total compared with subtotal thyroidectomy in benign nodular disease: personal series and review of published reports. Eur J Surg 164:501–506
Marchesi M, Biffoni M, Tartaglia F et al (1998) Total versus subtotal thyroidectomy in the management of multinodular goiter. Int Surg 83:202–204
Bergamaschi R, Becouarn G, Ronceray J et al (1998) Morbidity of thyroid surgery. Am J Surg 176:71–75
Kraimps JL, Marechaud R, Gineste D et al (1993) Analysis and prevention of recurrent goiter. Surg Gynecol Obstet 176:319–322
Miccoli P, Antonelli A, Iacconi P et al (1993) Prospective, randomized, double-blind study about effectiveness of levothyroxine suppression therapy in prevention of recurrence after operation: results at the third year follow-up. Surgery 114:1097–1101
Piraneo S, Vitri P, Galimberti A et al (1994) Recurrence of goiter after operation in euthyroid patients. Eur J Surg 160:351–356
Andaker L, Johansson K, Smeds S et al (1992) Surgery for hyperthyroidism: hemithyroidectomy plus contralateral resection or bilateral resection? A prospective randomized study of postoperative complications and long-term results. World J Surg 16:765–769. doi:10.1007/BF02067381
Dralle H, Sekulla C, Haerting J et al (2004) Risk factors of paralysis and functional outcome after recurrent laryngeal nerve monitoring in thyroid surgery. Surgery 136:1310–1322
Pacini F, Castagna MG, Brilli L et al (2009) Thyroid cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 21(Suppl 5):214–219
Friguglietti CU, Lin CS, Kulcsar MA (2003) Total thyroidectomy for benign thyroid disease. Laryngoscope 113:1820–1826
Reeve TS, Curtin A, Fingleton L et al (1994) Can total thyroidectomy be performed as safely by general surgeons in provincial centers as by surgeons in specialized endocrine surgical units? Making the case for surgical training. Arch Surg 129:834–836
Mishra A, Agarwal G, Agarwal A et al (1999) Safety and efficacy of total thyroidectomy in hands of endocrine surgery trainees. Am J Surg 178:377–380
Thomusch O, Machens A, Sekulla C et al (2000) Multivariate analysis of risk factors for postoperative complications in benign goiter surgery: prospective multicenter study in Germany. World J Surg 24:1335–1341. doi:10.1007/s002680010221
Zedenius J, Wadstrom C, Delbridge L (1999) Routine autotransplantation of at least one parathyroid gland during total parathyroidectomy may reduce permanent hypoparathyroidism to zero. Aust N Z J Surg 69:794–797
Kihara M, Yokomise H, Miyauchi A et al (2000) Recovery of parathyroid function after total thyroidectomy. Surg Today 30:333–338
Lo CY, Lam KY (1998) Postoperative hypocalcemia in patients who did or did not undergo parathyroid autotransplantation during thyroidectomy: a comparative study. Surgery 124:1081–1086
Conflict of interest
The authors have no potential or real conflict of interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rayes, N., Steinmüller, T., Schröder, S. et al. Bilateral Subtotal Thyroidectomy Versus Hemithyroidectomy Plus Subtotal Resection (Dunhill Procedure) for Benign Goiter: Long-Term Results of a Prospective, Randomized Study. World J Surg 37, 84–90 (2013). https://doi.org/10.1007/s00268-012-1793-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-012-1793-8