
Abstract
Introduction
The resection of os trigonum or posterior talar process as treatment for posterior ankle impingement is an established operation. However, the authors encountered several painful stress reactions in the posterior subtalar joint during follow-up resulting in persisting incapacity to do sports.
Methods
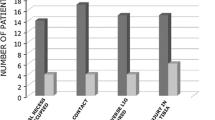
From March 2011 to July 2015, 29 patients with 30 feet were operated (22 endoscopic, 8 open resections). Average follow-up time was 43 ± 13 months. Complications were grouped into “none”, “temporary disadvantage” and “permanent damage”. The following radiographic parameters were measured: (1) length of posterior talar process or os trigonum, (2) length of the uncovered calcaneal joint surface after resection, (3) amount of resection.
Results
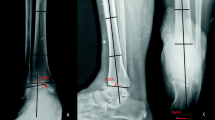
The rate of permanent damage was 13.3% (4 of 30 feet), and all four of these patients developed a painful stress reaction in the posterior subtalar joint. One temporary disadvantage (persistent pain for three months) was found. All patients with major complications showed retrospectively what we call the “risk configuration” —the radius of the talus ending within the subtalar joint. The length of the uncovered calcaneal joint surface was therefore significantly larger (6.4 mm ± 3.33) in feet with permanent damage than in feet without (1.06 mm ± 2.15, P < 0.001).
Conclusion
The resection of os trigonum or posterior talar process has a complication rate of 13.3% with persisting inability to do sports due to painful stress reaction in the posterior subtalar joint. The only risk factor found was the “risk configuration”. In such cases, the resection has to be made not anterior into the subtalar joint and patients have to be informed about this possible complication.
Study design
Retrospective case series; Evidence Level 4.




Similar content being viewed by others

References
Abramowitz Y, Wollstein R, Barzilay Y, London E, Matan Y, Shabat S, Nyska M (2003) Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 85-A(6):1051–1057
Ahn JH, Kim YC, Kim HY (2013) Arthroscopic versus posterior endoscopic excision of a symptomatic os trigonum: a retrospective cohort study. Am J Sports Med 41(5):1082–1089
Calder JD, Sexton SA, Pearce CJ (2010) Return to training and playing after posterior ankle arthroscopy for posterior impingement in elite professional soccer. Am J Sports Med 38(1):120–124
Galla M, Lobenhoffer P (2011) Technique and results of arthroscopic treatment of posterior ankle impingement. Foot Ankle Surg 17(2):79–84
Kim HK, Jeon JY, Dong Q, Kim HN, Park YW (2013) Ankle arthroscopy in a hanging position combined with hindfoot endoscopy for the treatment of concurrent anterior and posterior impingement syndrome of the ankle. J Foot Ankle Surg 52(6):704–709
Russell JA, Kruse DW, Koutedakis Y, McEwan IM, Wyon MA (2010) Pathoanatomy of posterior ankle impingement in ballet dancers. Clin Anat 23:613–621
Chao W (2004) Os trigonum. Foot Ankle Clin N Am 9:787–796
Blake RL, Lallas PJ, Ferguson H (1992) The os trigonum syndrome. A literature review. J Am Podiatr Med Assoc 82(3):154–161
Horibe S, Kita K, Natsu-ume T, Hamada M, Mae T, Shino K (2008) A novel technique of arthroscopic excision of a symptomatic os trigonum. Arthroscopy 24(1):121e1–121e4
Richards DT, Guerra JJ, Council D (2010) Arthroscopic excision of the os trigonum: using the posteromedial portal safely. Am J Orthop (Belle Mead NJ) 39(8):379–381
Willits K, Sonneveld H, Amendola A, Griffin JR, Griffin S, Fowler PJ (2008) Outcome of posterior ankle arthroscopy for hindfoot impingement. Arthroscopy 24(2):196–202
Nickisch F, Barg A, Salzmann CL, Beals TC, Bonasia DE, Phisitkul P, Femino JE, Amendola A (2012) Postoperative complications of posterior ankle and hindfoot arthroscopy. J Bone Joint Surg Am 94(5):439–446
Guo QW, Hu YL, Jiao C, Ao YF, Tian de X (2010) Open versus endoscopic excision of a symptomatic os trigonum: a comparative study of 41 cases. Arthroscopy 26(3):384–390
Marumoto JM, Ferkel RD (1997) Arthroscopic excision of the os trigonum: a new technique with preliminary clinical results. Foot Ankle Int 18(12):777–784
Noguchi H, Ishii Y, Takeda M, Hasegawa A, Monden S, Takagishi K (2010) Arthroscopic excision of posterior ankle bony impingement for early return to the field: short-term results. Foot Ankle Int 31(5):398–403
Park CH, Kim SY, Kim JR, Lee WC (2013) Arthroscopic excision of a symptomatic os trigonum in a lateral decubitus position. Foot Ankle Int 34(7):990–994
Tey M, Monllau JC, Centenera JM, Pelfort X (2007) Benefits of arthroscopic tuberculoplasty in posterior ankle impingement syndrome. Knee Surg Sports Traumatol Arthrosc 15(10):1235–1239
Veazy BL, Heckman JD, Galindo MJ, McGanity PL (1992) Excision of ununited fractures of the posterior process of the talus: a treatment for chronic posterior ankle pain. Foot Ankle 13(8):453–457
Weiss WM, Sanders EJ, Crates JM, Barber FA (2015) Arthroscopic excision of a symptomatic Os Trigonum. Arthroscopy 31(11):2082–2088
Kubosch EJ, Erdle B, Izadpanah K, Kubosch D, Uhl M, Südkamp NP, Niemeyer P (2016) Clinical outcome and T2 assessment following autologous matrix-induced chondrogenesis in osteochondral lesions of the talus. Int Orthop 40(1):65–71
Van Dijk CN, Scholtern PE, Krisp R (2000) A 2-portal endoscopic approach for diagnosis and treatment of posterior ankle pathology. Arthroscopy 16(8):871–876
Gosslings JC, Gouma DJ (2008) What is a surgical complication? World J Surg 32(6):952
Kolb A, Willegger M, Schuh R, Kaider A, Chiari C, Windhager R (2017) The impact of different types of talus deformation after treatment of clubfeet. Int Orthop 41(1):93–99
Badekas T, Takvorian M, Souras N (2013) Treatment principles for osteochondral lesions in foot and ankle. Int Orthop 37(9):1697–1706
Radke S, Vispo-Seara J, Walther M, Ettl V (2001) Transient bone marrow edema of the foot. Int Orthop 25:263–267
Hedrick MR, McBryde AM (1994) Posterior ankle impingement. Foot Ankle Int 15:2–8
Mann HA, Myerson MS (2010) Treatment of posterior ankle pain by excision of a bipartite talar fragment. J Bone Joint Surg (Br) 92-B:954–957
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
There is no funding source.
Ethical approval
The study was approved by the ethical review board. This study was carried out in accordance with the Declaration of Helsinki.
Informed consent
Written informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Frigg, A., Maquieira, G. & Horisberger, M. Painful stress reaction in the posterior subtalar joint after resection of os trigonum or posterior talar process. International Orthopaedics (SICOT) 41, 1585–1592 (2017). https://doi.org/10.1007/s00264-017-3489-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-017-3489-z