
Abstract
Purpose
Although the natural history of dual mobility has been exclusively borne for 20 years by a single company (due to industrial ownership), the concept has undeniably been very widely popularised with nearly 40 cups on the French market which should be regarded as a weight bearing surface, both broadly and in their own right. However, within the same original idea, these implants are not all identical (design, material, fixation ect.).The aim of this work is to propose a classification of different dual mobility cups by distinguishing between thegeneral characteristics of a conventional cup and those particular to this type of implant.
Methods
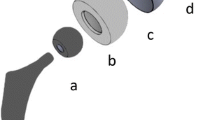
By comparison with a standard metal-back cup, dual mobility is based on at least one additional interface corresponding to the mobility of the polyethylene insert in the concavity of the acetabular cup called the outersurface. Design, constitutive material, fixation of the cup and characteristics of the retentive insert are analysed through the published results.
Results
The complications associated, in particular, the intraprosthetic dislocation and to a lesser extent fixation failures undoubtedly condemned the dissemination of the dual mobility concept, as witnessed by the fact that despite the precedence of this 40-year old concept, the overriding majority of publications (more than 95%) have only appeared in the last ten years.
Conclusion
The latest generation of dual mobility cups combines: 1) a cast chrome-cobalt alloy cup covered with a bilayer coating of porous titanium and hydroxyapatite for long-term press-fit fixation to 2) an insert designed to eliminate all of the risks of intraprosthetic dislocation, whilst keeping all of the elasticity properties of the polyethylene, which has demonstrated its medium and long term effectiveness on preventing instability by overcoming other complications.






Similar content being viewed by others


References
Farizon F, de Lavison R, Azoulai JJ, Bousquet G (1998) Results with a cementless alumina-coated cup with dual mobility. A twelve-year follow-up study. Int Orthop 22:219–24
Bousquet G, Argenson C, Godeneche JL, Cisterne JP, Gazielly DF, Girardin P, Debiesse JL (1986) Recovery after aseptic loosening of cemented total hip arthroplasties with Bousquet’s cementless prosthesis. Apropos of 136 cases. Rev Chir Orthop Reparatrice Appar Mot 72:70–4, Suppl 2
Khan RJ, Fick D, Alakeson R, Haebich S, de Cruz M, Nivbrant B, Wood D (2006) A constrained acetabular component for recurrent dislocation. J Bone Joint Surg (Br) 88:870–6
Morscher EW, Widmer KH, Bereiter H, Elke R, Schenk R (2002) Cementless socket fixation based on the “press-fit” concept in total hip joint arthroplasty. Acta Chir Orthop Traumatol Cech 69:8–15
Widmer KH, Zurfluh B, Morscher EW (2002) Load transfer and fixation mode of press-fit acetabular sockets. J Arthroplasty 17:926–35
Salamon A, Salamon T, Sef D, Jo-Osvatic A (2004) Morphological characteristics of the acetabulum. Coll Antropol 28(Suppl 2):221–6
Wegrzyn J, Tebaa E, Jacquel A, Carret JP, Bejui-Hugues J, Pibarot V (2015) Can dual mobility cups prevent dislocation in all situations after revision total hip arthroplasty? J Arthroplasty 30:631–40
Nag S, Banerjee R, Fraser HL (2007) A novel combinatorial approach for understanding microstructural evolution and its relationship to mechanical properties in metallic biomaterials. Acta Biomater 3:369–76
Philippot R, Farizon F, Camilleri JP, Boyer B, Derhi G, Bonnan J, Fessy MH, Lecuire F (2008) Survival of dual mobility socket with a mean 17 years follow-up. Rev Chir Orthop Reparatrice Appar Mot 94:43–8
Mavrogenis AF, Papagelopoulos PJ, Babis GC (2011) Osseointegration of cobalt-chrome alloy implants. J Long Term Eff Med Implants 21:349–58
Patel B, Inam F, Reece M, Edirisinghe M, Bonfield W, Huang J, Angadji A (2010) A novel route for processing cobalt-chromium-molybdenum orthopaedic alloys. J R Soc Interface 7:1641–5
HAS (2007) Evaluation des prothèses de hanche. Révision des descriptions génériques de la liste de produits et prestations remboursables implants articulaires de hanche. Paris
Wegrzyn J, Pibarot V, Jacquel A, Carret JP, Bejui-Hugues J, Guyen O (2014) Acetabular reconstruction using a Kerboull cross-plate, structural allograft and cemented dual-mobility cup in revision THA at a minimum 5-year follow-up. J Arthroplasty 29:432–7
Schneider L, Philippot R, Boyer B, Farizon F (2011) Revision total hip arthroplasty using a reconstruction cage device and a cemented dual mobility cup. Orthop Traumatol Surg Res 97:807–13
Hamadouche M, Biau DJ, Huten D, Musset T, Gaucher F (2010) The use of a cemented dual mobility socket to treat recurrent dislocation. Clin Orthop Relat Res 468:3248–54
Langlais FL, Ropars M, Gaucher F, Musset T, Chaix O (2008) Dual mobility cemented cups have low dislocation rates in THA revisions. Clin Orthop Relat Res 466:389–95
Wegrzyn J, Thoreson AR, Guyen O, Lewallen DG, An KN (2013) Cementation of a dual-mobility acetabular component into a well-fixed metal shell during revision total hip arthroplasty: a biomechanical validation. J Orthop Res 31:991–7
Ryan G, Pandit A, Apatsidis DP (2006) Fabrication methods of porous metals for use in orthopaedic applications. Biomaterials 27:2651–70
LeGeros RZ (2002) Properties of osteoconductive biomaterials: calcium phosphates. Clin Orthop: 81–98
Dumbleton JH, Manley M (2004) Hydroxyapatite-coated prostheses in total hip and knee arthroplasty. In The journal of bone and joint surgery, pp. 2526
Laursen MB, Nielsen PT, Soballe K (2007) Bone remodelling around HA-coated acetabular cups: a DEXA study with a 3-year follow-up in a randomised trial. Int Orthop 31:199–204
Orlik J, Zhurov A, Middleton J (2003) On the secondary stability of coated cementless hip replacement: parameters that affected interface strength. Med Eng Phys 25:825–31
Yamada H, Yoshihara Y, Henmi O, Morita M, Shiromoto Y, Kawano T, Kanaji A, Ando K, Nakagawa M, Kosaki N, Fukaya E (2009) Cementless total hip replacement: past, present, and future. J Orthop Sci 14:228–41
Munting E (1994) Géométrie et caractéristiques de surface des implants: deux aspects indissociables de la fixation prothétique. In Cahiers d’enseignement de la SOFCOT - Hydroxyapatite et prothèses articulaires, ed. ES Française, pp. 13–9. Paris
Manley MT, Capello WN, D’Antonio JA, Edidin AA, Geesink RG (1998) Fixation of acetabular cups without cement in total hip arthroplasty. A comparison of three different implant surfaces at a minimum duration of follow-up of five years. J Bone Joint Surg Am 80:1175–85
Simian E, Chatellard R, Druon J, Berthouet J, Rosset J (2015) Dual mobility in revision total hip arthroplasty: dislocation rate and survival at 5 years. Orthop Traumatol Surg Res 101:577
Massin P, Orain V, Philippot R, Farizon F, Fessy MH (2012) Fixation failures of dual mobility cups: a mid-term study of 2601 hip replacements. Clin Orthop Relat Res 470:1932–40
Prudhon JL, Ferreira A, Verdier R (2013) Dual mobility cup: dislocation rate and survivorship at ten years of follow-up. Int Orthop 37:2345–50
Caton JH, Prudhon JL, Ferreira A, Aslanian T, Verdier R (2014) A comparative and retrospective study of three hundred and twenty primary Charnley type hip replacements with a minimum follow up of ten years to assess whether a dual mobility cup has a decreased dislocation risk. Int Orthop 38:1125–9
Lecuire F, Benareau I, Rubini J, Basso M (2004) Intra-prosthetic dislocation of the Bousquet dual mobility socket. Rev Chir Orthop Reparatrice Appar Mot 90:249–55
Philippot R, Boyer B, Farizon F (2013) Intraprosthetic dislocation: a specific complication of the dual-mobility system. Clin Orthop Relat Res 471:965–70
Varadarajan KM, Zumbrunn T, Duffy MP, Patel R, Freiberg AA, Rubash HE, Malchau H, Muratoglu OK (2016) Reducing the distal profile of dual mobility liners can mitigate soft-tissue impingement and liner entrapment without affecting mechanical performance. J Orthop Res 34:889–97
Philippot R, Camilleri JP, Boyer B, Adam P, Farizon F (2009) The use of a dual-articulation acetabular cup system to prevent dislocation after primary total hip arthroplasty: analysis of 384 cases at a mean follow-up of 15 years. Int Orthop 33:927–32
Hamadouche M, Arnould H, Bouxin B (2012) Is a Cementless Dual Mobility Socket in Primary THA a Reasonable Option? Clin Orthop Relat Res 470:3048–53
Puch JM, Derhi G, Descamps L, Verdier R, Caton JH (2016) Dual-mobility cup in total hip arthroplasty in patients less than fifty five years and over ten years of follow-up: a prospective and comparative series. Int Orthop
Dowd JE, Sychterz CJ, Young AM, Engh CA (2000) Characterization of long-term femoral-head-penetration rates. Association with and prediction of osteolysis. J Bone Joint Surg Am 82-A:1102–7
Dumbleton JH, Manley MT, Edidin AA (2002) A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 17:649–61
Shen C, Tang ZH, Hu JZ, Zou GY, Xiao RC, Yan DX (2014) Does cross-linked polyethylene decrease the revision rate of total hip arthroplasty compared with conventional polyethylene? A meta-analysis. Orthop Traumatol Surg Res 100:745–50
D’Apuzzo MR, Koch CN, Esposito CI, Elpers ME, Wright TM, Westrich GH (2016) Assessment of damage on a dual mobility acetabular system. J Arthroplasty 31:1828-35. doi: 10.1016/j.arth.2016.01.039
Brach Del Prever EM, Bistolfi A, Bracco P, Costa L (2009) UHMWPE for arthroplasty: past or future? J Orthop Traumatol 10:1–8
Pruitt LA (2005) Deformation, yielding, fracture and fatigue behavior of conventional and highly cross-linked ultra high molecular weight polyethylene. Biomaterials 26:905–15
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Thierry ASLANIAN is an employee of groupe lépine.
Funding
There is no funding source.
Ethical approval
No procedure in this study has involved human participants.
Rights and permissions
About this article

Cite this article
Aslanian, T. All dual mobility cups are not the same. International Orthopaedics (SICOT) 41, 573–581 (2017). https://doi.org/10.1007/s00264-016-3380-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-016-3380-3