
Abstract
Purpose
Despite the fact that new and modern short-stems allow bone sparing and saving of soft-tissue and muscles, we still face the challenge of anatomically reconstructing the femoro-acetabular offset and leg length. Therefore a radiological and clinical analysis of a short-stem reconstruction of the femoro-acetabular offset and leg length was performed.
Methods
Using an antero-lateral approach, the optimys short-stem (Mathys Ltd, Bettlach, Switzerland) was implanted in 114 consecutive patients in combination with a cementless cup (Fitmore, Zimmer, Indiana, USA; vitamys RM Pressfit, Mathys Ltd, Bettlach, Switzerland). Pre- and postoperative X-rays were done in a standardized technique. In order to better analyse and compare X-ray data a special double coordinate system was developed for measuring femoral- and acetabular offset. Harris hip score was assessed before and six weeks after surgery. Visual analogue scale (VAS) satisfaction, leg length difference and the existence of gluteal muscle insufficiency were also examined.
Results
Postoperative femoral offset was significantly increased by a mean of 5.8 mm. At the same time cup implantation significantly decreased the acetabular offset by a mean of 3.7 mm, which resulted in an increased combined femoro-acetabular offset of 2.1 mm. Postoperatively, 81.7 % of patients presented with equal leg length. The maximum discrepancy was 10 mm. Clinically, there were no signs of gluteal insufficiency. No luxation occurred during hospitalization. The Harris hip score improved from 47.3 before to 90.1 points already at six weeks after surgery while the mean VAS satisfaction was 9.1.
Conclusion
The analysis showed that loss of femoro-acetabular offset can be reduced with an appropriate stem design. Consequently, a good reconstruction of anatomy and leg length can be achieved. In the early postoperative stage the clinical results are excellent.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
As part of the endoprosthetic treatment of hip osteoarthritis new femoral stems have been developed in recent years aiming at better preservation of bone stock. In this context the femoral neck preserving short-stem prostheses have gained importance. These prosthetic designs have been on the market since the 1980s but they were restricted to a young patient clientele and have hence not prevailed extensively. Initially the goal was to achieve a good osteointegration with only metaphyseal anchoring systems, e.g. thrust plate prosthesis (Zimmer), CUT prosthesis (Orthodynamics), Spiron prosthesis (k-implant) [1]. However, an exact reconstruction of the natural anatomy could not be achieved this way. In recent years the market share of short stems has markedly increased due to new studies describing equivalent or superior bone stability even in elderly patients [2, 3]. At the same time, the literature is increasing in agreement that an accurate reconstruction of the hip joint anatomy is crucial for the clinical outcome. Besides leg length and caput-collum-diaphyseal angle (CCD angle), the femoro-acetabular offset has increasingly come into focus. The femoro-acetabular offset consists of two parts: the femoral offset, as the distance from the centre line of the femur to the centre of rotation, as well as the acetabular offset, as the distance from the centre of rotation to the central point of the acetabular coordinate system, which is the midline of the pelvis. For a long time the offset recovery has been neglected in comparison to the restoration of leg length. However, studies have indicated that a reduced offset can have severe consequences [4], like instability of the hip joint. By causing low soft tissue tension it leads to a restricted range of motion and an increased risk of dislocation [5]. At the same time a decreased postoperative muscular preload can cause muscle weakness and fatigue. Insufficiency of the gluteus muscle group results in a Trendelenburg gait [6].
Further, an increased wear of prosthetic material and frequently occurring impingement with concomitant femoral pelvic rubbing were detected with a reduced offset [7–9].
In contrast, by increasing the lever arm of the abductors an increased femoro-acetabular offset counteracts the above aspects by maximizing the transmission of muscle forces [10, 11]. This, by reducing the forces on the hip joint, causes reduction of abrasion of the articular capsule and the inlay [12]. However, a disproportionate increase in offset can cause trochanteric bursitis.
Given these findings, it appears that a loss of offset has great clinical relevance.
Implantation of the cup typically causes a reduction of the acetabular offset due to a medialisation. The design of any stem should thus make possible the maintenance of femoral offset, or even its increase. This should, however, remain within reasonable limits in conformity to the individual anatomy of the patient.
The present study examined if the femoro-acetabular offset can be reconstructed with implantation of an optimys short-stem prosthesis and if leg length can be maintained as well.
Materials and methods
In the present study a total of 114 consecutive, unilateral hip joints were prospectively included. For 109 patients evaluation and follow up could be performed. In all patients the meta-diaphyseal anchoring short-stem system optimys (Mathys Ltd. Bettlach, Switzerland) was used (Fig. 1). It is a femoral neck preserving prosthesis made of titanium, which is available in 12 different sizes, with a 12/14-mm cone and two different offset versions. Neck length increases in steps of 1.4 mm in analogy to stem size. The lateral offset variant shifts the centre of rotation by 5 mm without influencing leg length. The special stem design allows good bone contact at the distal lateral cortex and the proximal medial cortex.

Pelvis overview with optimys short-stem implanted on the right side
The prosthesis is aligned along the proximal medial cortex and the calcar femorale. Anchoring is based on the fit-and-fill principle, but can also be done as classic three-point anchoring in some cases. In addition the triple conical shape is supposed to achieve good primary stability and prevent sintering. The greater trochanter region remains intact.
The optimys stem was combined with cementless press-fit cups (Fitmore, Zimmer; RM Pressfit vitamys, Mathys Ltd. Bettlach) with a ceramic-polyethylene bearing couple. The implantations were performed at the Department of Orthopaedic Surgery at St. Josef's Hospital Wiesbaden, Germany, in the years 2010 to 2012. All operations were performed through a minimally invasive, antero-lateral approach in a standardized surgical technique [13]. Mean patient age was 63 years (range, 33–86 years). Fifty-one women and 58 men were operated upon. In 46 cases, the left side was affected, 63 patients were treated on the right side.
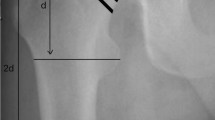
All patients underwent pre- and postoperative digital antero-posterior imaging with a standardized technique. For the purpose of producing the deep pelvic X-ray-survey a positioning splint with 20° internal rotation of hip joints was used. Radiological evaluation was performed by one examiner. In order to achieve an accurate measurement of the hip anatomy a double coordinate system was applied on both the preoperative and the postoperative images (Figs. 2 and 3). This method has already been described [14–16]. Measurement of the femoral, the acetabular as well as the combined total offset was performed. The measured data were calculated with an individual scaling factor, which was generated using the diameter of the femoral head of the opposite side, comparing the preoperative to the postoperative image [14]. Data analysis was performed using MS Excel (Microsoft, Redmond, USA). In addition, patients were clinically examined six weeks postoperative or later for possible signs of an insufficiency of the gluteal muscles like a Trendelenburg gait or a positive Trendelenburg sign. Harris hip score and satisfaction on a visual analogue scale (VAS 0–10) were also assessed. Finally, leg-length discrepancy compared with the non-operated side was examined clinically by comparing the height of iliac crests on both sides of the standing patient.

Pre-operative digital measurement. Acetabular offset—midline pelvis to centre of rotation (83 mm). Femoral offset—centre of rotation to centre line femur (38 mm). Total offset—acetabular offset plus femoral offset (121 mm)

Postoperative digital measurement. Acetabular offset—midline pelvis to centre of rotation (78 mm). Femoral offset—centre of rotation to centre line femur (43 mm). Total offset—acetabular offset plus femoral offset (121 mm)
Ethical approval
A positive ethics committee vote of Freiburg Ethics Commission International from 10/04/2010 was received (feci Code: 010/2071).
Statistics
The two-sided Wilcoxon signed rank test was used to compare the pre- and postoperative acetabular offset, femoral offset, total offset, leg-length difference as well as the Harris hip score and VAS satisfaction. A p-value <0.05 was considered to be statistically significant. All statistical analyses were performed using SAS Enterprise Guide 4.2 (SAS Institute Inc., Cary, USA).
Results
Of the originally 114 enrolled patients five had to be withdrawn in the course of the study. Four patients had not presented for follow up, but assured that they were free of complaints by telephone. One patient underwent an intra-operative method change because of femoral perforation and could not be evaluated according to protocol.
The postoperative femoral offset changed significantly by an average of 5.8 mm (standard deviation [SD]: 4.8). The corresponding maximum was 17.9 mm, the most marked reduction was −5.0 mm (Table 1). In contrast, due to a frequent medial shift of the cup and the centre of rotation, a significant reduction of the acetabular offset by an average of 3.7 mm (SD: 5.1) resulted. Here, the corresponding maximum was 19.5 mm; the most pronounced lateralisation was 9.1 mm (Table 1). The calculation of the combined total offset thus showed a statistically significant mean increase of 2.1 mm (SD: 5.8) (Table 1).
A clinical mean leg length discrepancy of 1.2 mm (maximum: 10 mm; SD: 3.3) was observed in the complete patient sample whereby discrepancies were only seen in 18.3 % (20 patients) (Table 2).
No signs for postoperative gluteal muscle insufficiency were found in any of the patients included. One traumatic dislocation occurred during rehabilitation. It could be repositioned and required no further therapy. The Harris hip score at six weeks after surgery was 90.1, compared with 47.4 before surgery. Patient satisfaction on VAS was 9.1 (Table 3).
Discussion
We found an increase of total offset of 2.1 mm. While the acetabular offset was reduced by 3.7 mm the femoral offset gained 5.8 mm. The clinical results in the early postoperative stage were excellent.
The development of the latest generation short-stem prostheses aimed at mapping the patient-specific anatomy as well as possible. Reconstruction of the patient-specific hip geometry is of decisive importance for the clinical function of the hip joint after total hip arthroplasty. This was already suggested for other types of prostheses [14, 17]. The pre-operatively performed digital planning allows a 2D simulation of the implantation and thus the possibility of determining elements such as the femoro-acetabular offset, leg length or varus/valgus positioning of the stem in advance. The accuracy and the usefulness of digital planning could be confirmed in the majority of studies [18, 19]. Nevertheless a statement on the potential for anatomic reconstruction of the important geometric parameters (offset/CCD angle/leg length) was rarely found in studies using a standardized radiological evaluation of the pre- and post-operative conditions [1]. Many short-stem systems could not convince regarding the implementation of the planned results for the femoro-acetabular offset and leg length. Babisch [20] showed that an adequate individualized reconstruction of the anatomical situation is only possible with a few short-stem models and that it is critically dependent on the anatomical conditions of the patient. Jerosch [21] showed an inadequate reconstruction of the individual offsets using digital planning in a total of 90 different implants. Wedemeyer et al. [16] was able to find a great match of pre-operatively planned sizes with those actually implanted in a series of 40 Mayo (Zimmer) stems. The intended offset and CCD angle could, however, not be implemented sufficiently, leading to changes in hip geometry.
A common problem is the loss of femoro-acetabular offset. Studies have shown that a reduced offset can have severe consequences [4–9]. Overall, an increase of offset by an extension of the abductor lever and thus an improved force transmission can reduce the load on the hip joint [22], which often leads to more muscular stability. In addition, the risk of possible impingement symptoms is reduced and the range of motion can be increased [23].
Röthlisberger [24] showed a medium loss of acetabular offset of about 4.6 mm in the context of 120 implantations of cementless short-stem systems with a corresponding cementless press-fit cup (optimys; RM Pressfit vitamys, Mathys Ltd, Bettlach, Switzerland) [24]. A medialization of the cup is especially typical using cementless cups. The press-fit principle requires a sufficient cavity of the acetabulum in order to achieve a stable situation. As a result the hip joint’s centre of rotation is often medialized resulting in a loss of offset. It can therefore be regarded as the duty of the stem to compensate the loss of acetabular offset by increasing the femoral offset to prevent a total offset loss and thus limitations in clinical function. In the study of Höhle et al. [15], 191 Metha (B.Braun Melsungen) and Mayo (Zimmer) stems were implanted in combination with cementless press-fit cups. The results also showed a reduction of the acetabular offset by a mean of 4.9 mm. However, the examined short-stems could not compensate the loss of acetabular offset. In addition a mean loss of 0.7 mm of femoral offset and a total offset loss of 5.6 mm was observed [15].
The reasons for the offset loss can be found by looking at the design of these short-stem systems. For most of them, the variance of the individual positioning of the stem is limited and the CCD angles are often rather large. Frequently, the stem aligns itself in a valgus position during the implantation, which results in a reduced femoral offset and can consequently lead to gluteal insufficiency. Although the average CCD angle of patients with arthritis of the hip joint is about 125°, it shows a significant variance and can commonly range from 110° to 145° [23]. A stem design with an average CCD angle of 135° after implantation can’t compensate the large CCD angles and will inevitably lead to an overall loss of offset. In the study of Höhle et al. [15] the implantation of the short-stem systems Metha and Mayo often led to an increased valgus position compared to the preoperative planning. On the other hand Jerosch et al. [1] showed an average reduction of the CCD angle of only 0.5° in a series of the MiniHip stem (Corin), a short-stem of the latest generation.
In case of exceptional anatomical features such as a significant varus position of the femoral neck, however, a careful pre-operative planning is essential. In such cases the new generation short-stem systems can also reach their limits.
The optimys short-stem uses the anatomy of the medial cortex to position itself along the calcar femorale. According to the pre-existing pre-operative CCD angle it can re-establish the varus-valgus position of the femoral neck in a large bandwidth (Figs. 4 and 5). In addition, the resection of the femoral neck determines the positioning of the stem in the proximal femur. Thus, according to the digital planning, resection can be varied to affect the stem position. A high resection of the femoral neck leads the stem alongside the calcar in a varus position with a correspondingly large offset; a valgus position is also achieved along the calcar, but by deep resection. The stem is available in 12 sizes. Unlike other systems, the neck length extends with each prosthesis size for another 1.4 mm. Thus, it takes account of the tendency that a marked varus anatomy needs rather small implant sizes whereas in femoral neck valgus positions rather large implant sizes are used [1]. This means that implants brought into valgus position are able to better counteract a loss of offset by an implicit extension in comparison to smaller stems. Furthermore, given the option of choosing from two different offset versions, a standard and a lateral version, which increases the offset compared to the standard cone by about 5 mm, an optimal offset recovery can be achieved.

Pre-operative digital planning (left) and postoperative result (right). According to the pre-existing preoperative CCD angle the varus position of the femoral neck can be reestablished

Pre-operative digital planning (left) and postoperative result (right). According to the pre-existing preoperative CCD angle the valgus position of the femoral neck can be reestablished
The reconstruction of the patient’s normal anatomy is decisive. In summary it is both an individualized resection of the femoral neck for the purpose of varying the femoral offset for a varus or valgus anatomy, as well as the possibility contained in the stem design in being able to choose a standard or a lateral offset version. These features, taken together, have been developed in order to prevent a possible offset loss.
The patients included in this study were examined for signs of gluteal muscle insufficiency. For this purpose, the occurrence of a Trendelenburg gait or a positive Trendelenburg test was chosen. It is characterized by a descent of the pelvis in the stance phase to the opposite side with a corresponding lateral bending of the trunk onto the supporting leg. It is considered a sign of weakness or paralysis of the hip abductors (M. gluteus medius and M. gluteus minimus). The absence of this limp in this entire cohort of 109 patients suggests a sufficient stabilization of the gluteal muscles by maintaining the offset. The increase of femoral offset with a medial shift of the centre of rotation, effected by increasing the lever arm of the abductor muscles, enhanced muscular stability. The single dislocation, which occurred during rehabilitation was due to a fall out of bed and was therefore not regarded as a cause of instability.
Future studies of these patients should also include the possible negative consequences of an increased offset, e.g. cortical hypertrophy caused by a suspected increased medial bending stress in the distal part of the prosthesis [17]. Clinical care should be taken in particular of induced symptomatic trochanteric bursitis.
Weakness of study
The short follow-up period of six weeks limits the present study regarding information about mid- and long-term survival of the optimys stem. To date, a statement concerning its long-term stability cannot be made, which was, however, not the goal of the investigation. In addition, since the Department of Orthopaedic Surgery of St. Josefs Hospital Wiesbaden has been involved in the development of the stem, the surgeons involved in the study are very experienced, and in the future it needs to be seen if other centres can replicate our results.
Conclusion
The present study showed that the versatile design of the optimys short-stem system is able to compensate loss of offset due to medialization of the cup in cementless press-fit-cup systems. The special design and the wide range of resulting possibilities for an individual positioning combined with two offset versions can effectively prevent the frequently occurring loss of total offset in hip arthroplasty. This can be achieved for a multitude of different hip anatomies. A gluteal muscle insufficiency and the associated clinical consequences can therefore be prevented satisfactorily. Leg length can be adequately balanced in comparison to the contralateral side. Preoperative digital planning remains essential in order to achieve the objective of an individually reconstructed hip geometry.
References
Jerosch J, Grasselli C, Kothny P (2012) Veränderungen von Offset, CCD-Winkel und Beinlänge nach Implantation einer metadiaphysär fixierten Kurzschaftprothese–eine radiologische Untersuchung. Zeitschrift Für Orthopädie Und Unfallchirurgie, pp 20–26
Roth A, Richartz G, Sander K, Sachse A, Fuhrmann R, Wagner A, Venbrocks R-A (2005) Verlauf der periprothetischen Knochendichte nach H{ü}fttotalendoprothesenimplantation. Abh{ä}ngigkeit von Prothesentyp und kn{ö}cherner Ausgangssituation. Orthopade 34:334–344. doi:10.1007/s00132-005-0773-1
Götze C, Ehrenbrink J, Ehrenbrink H (2010) Is there a bone-preserving bone remodelling in short-stem prosthesis? DEXA analysis with the Nanos total hip arthroplasty. Zeitschrift Für Orthopadie Und Unfallchirurgie 148:398–405. doi:10.1055/s-0030-1250151
Matsushita A, Nakashima Y, Jingushi S, Yamamoto T, Kuraoka A, Iwamoto Y (2009) Effects of the femoral offset and the head size on the safe range of motion in total hip arthroplasty. J Arthroplasty 24:646–651. doi:10.1016/j.arth.2008.02.008
McCabe JP (1998) Dislocation following total hip arthroplasty. Curr Opin Orthop 9:9–13
Asayama I, Chamnongkich S, Simpson KJ, Kinsey TL, Mahoney OM (2005) Reconstructed hip joint position and abductor muscle strength after total hip arthroplasty. J Arthroplasty 20:414–420. doi:10.1016/j.arth.2004.01.016
Sakalkale DP, Sharkey PF, Eng K, Hozack WJ, Rothman RH (2001) Effect of femoral component offset on polyethylene wear in total hip arthroplasty. Clin Orthop Related Res 338:125–134
Malik A, Maheshwari A, Dorr LD (2007) Impingement with total hip replacement. J Bone Joint Surg Am Vol 89:1832–1842. doi:10.2106/JBJS.F.01313
Johnston TL, Schenker ML, Briggs KK, Philippon MJ (2008) Relationship between offset angle alpha and hip chondral injury in femoroacetabular impingement. Arthroscopy J Arthrosc Relat Surg 24:669–675. doi:10.1016/j.arthro.2008.01.010
Yamaguchi T, Naito M, Asayama I, Ishiko T (2004) Total hip arthroplasty: the relationship between posterolateral reconstruction, abductor muscle strength, and femoral offset. J Orthop Surg (Hong Kong) 12(2):164–167
McGrory BJ, Morrey BF, Cahalan TD, An KN, Cabanela ME (1995) Effect of femoral offset on range of motion and abductor muscle strength after total hip arthroplasty. J Bone Joint Surg Br 77:865–869
Charles MN, Bourne RB, Davey JR, Greenwald AS, Morrey BF, Rorabeck CH (2005) Soft-tissue balancing of the hip: the role of femoral offset restoration. Instr Course Lect 54:131–141
Pfeil J (2010) Minimally invasive surgery in total hip arthroplasty. Springer, Berlin
Schröder SM (2011) Prädiktion und Qualitätsverbesserung in der Hüftendoprothetik durch digitale Planung bezüglich des Prothesentyps, der Prothesengröße, der Beinlänge, des Offsets und des Pfannenreinigungswinkels. Dissertation, University of Heidelberg, Germany
Höhle P, Schröder SM, Pfeil J (2014) Comparison between preoperative digital planning and postoperative outcomes in 197 hip endoprosthesis cases using short stem prostheses. Clin Biomech. 18 Nov [Epub ahead of print]
Wedemeyer C, Quitmann H, Xu J, Heep H, von Knoch M, Saxler G (2008) Digital templating in total hip arthroplasty with the Mayo stem. Arch Orthop Trauma Surg 128(10):1023–1029. doi:10.1007/s00402-007-0494-5
Jerosch J, Funken S (2004) Change of offset after implantation of hip alloarthroplasties. Unfallchirurg 107(6):475–482. doi:10.1007/s00113-004-0758-2
Della Valle AG, Padgett DE, Salvati EA (2005) Preoperative planning for primary total hip arthroplasty. J Am Acad Orthop Surg 13(7):455–462
Iorio R, Siegel J, Specht LM, Tilzey JF, Hartman A, Healy WL (2009) A comparison of acetate vs digital templating for preoperative planning of total hip arthroplasty: is digital templating accurate and safe? J Arthroplast 24(2):175–179. doi:10.1016/j.arth.2007.11.019
Babisch J (2013) Möglichkeiten der patientenindividuellen Hüftgelenkrekonstruktion und Knochenresektion bei Kurzschaftprothesen. In: Jerosch J (ed) Kurzschaftendoprothesen—Wo liegen dieUnterschiede? Deutscher Ärzte-Verlag, Köln
Jerosch, J (2012) Kurzschaftendoprothesen: Wo liegen die Unterschiede? Deutscher Ärzteverlag, Köln, p 234
Steinberg B, Harris W (1992) The offset problem in total hip arthroplasty. J Contemp Orthop Res 24:556–562
Massin P, Geais L, Astoin E, Simondi M, Lavaste F (2000) The anatomic basis for the concept of lateralized femoral stems: a frontal plane radiographic study of the proximal femur. J Arthroplast 15(1):93–101
Röthlisberger M (2014) Reconstruction of radiological parameters using a short stem hip prosthesis. Diploma thesis, Institute of Mathematical Statistics and Actuarial Science, University of Bern, Switzerland
Conflict of interest
The authors declare that they have no conflict of interest.
Prof. Dr. Joachim Pfeil has a medical advisor contract with Mathys Ltd., Switzerland.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article

Cite this article
Kutzner, K.P., Kovacevic, M.P., Roeder, C. et al. Reconstruction of femoro-acetabular offsets using a short-stem. International Orthopaedics (SICOT) 39, 1269–1275 (2015). https://doi.org/10.1007/s00264-014-2632-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-014-2632-3