
Abstract
Background
Although mucolipidosis type II has similar metabolic abnormalities to those found in all the mucopolysaccharidoses and mucolipidoses, there are distinctive diagnostic radiographic changes of mucolipidosis II in the perinatal/newborn/infant period.
Objective
To describe the early characteristic radiographic changes of mucolipidosis II and to document when these changes manifest and resolve.
Materials and methods
We retrospectively reviewed radiographs and clinical records of 19 cases of mucolipidosis II from the International Skeletal Dysplasia Registry (1971–present; fetal age to 2½ years). A radiologist with special expertise in skeletal dysplasias evaluated the radiographs.
Results
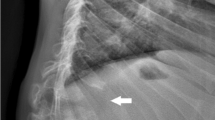
The most common abnormalities were increased vertebral body height (80%, nonspecific), talocalcaneal stippling (86%), periosteal cloaking (74%) and vertebral body rounding (50%). Unreported findings included sacrococcygeal sclerosis (54%) and vertebral body sclerosis (13%). Rickets and hyperparathyroidism-like (pseudohyperparathyroidism) changes (rarely reported) were found in 33% of cases. These changes invariably started in the newborn period and resolved by 1 year of age. The conversion from these early infantile radiographic features to dysostosis multiplex changes occurred in 41% of cases, and within the first year after birth.
Conclusion
Several findings strongly suggest the diagnosis of mucolipidosis II, including cloaking in combination with one or more of the following radiographic criteria: talocalcaneal stippling, sacrococcygeal or generalized vertebral body sclerosis, vertebral body rounding, or rickets/hyperparathyroidism-like changes in the perinatal/newborn/infancy period. These findings are not found in the other two forms of mucolipidosis nor in any of the mucopolysaccharidoses.








Similar content being viewed by others


References
Kollmann K, Pestka JM, Kühn SC et al (2013) Decreased bone formation and increased osteoclastogenesis cause bone loss in mucolipidosis II. EMBO Mol Med 5:1871–1886
David-Vizcarra G, Briody J, Ault J et al (2010) The natural history and osteodystrophy of mucolipidosis types II and III. J Paediatr Child Health 46:316–322
Lachman RS, Burton BK, Clarke LA et al (2014) Mucopolysaccharidosis IVA (Morquio A syndrome) and VI (Maroteaux-Lamy syndrome): under-recognized and challenging to diagnose. Skeletal Radiol 43:359–369
Cathey SS, Leroy JG, Wood T et al (2010) Phenotype and genotype in mucolipidoses II and III alpha/beta: a study of 61 probands. J Med Genet 47:38–48
Leroy JG, Cathey S, Friez MJ (2012) Mucolipidosis II. In: Ragon RA, Adam MP, Ardinger HH et al (eds) GeneReviews. University of Washington, Seattle, pp 1–24
Leroy JG, Demars RI (1967) Mutant enzymatic and cytological phenotypes in cultured human fibroblasts. Science 157:804–806
Leroy JG, Spranger JW (1970) I-cell disease. N Engl J Med 283:598–599
Maroteaux P, Lamy M (1966) Hurler’s pseudo-polydystrophy. Presse Med 74:2889–2892
Landing B, Silverman F, Craig J et al (1964) Familial neurovisceral lipidosis: an analysis of eight cases of a syndrome previously reported as ‘Hurler-variant’, ‘Pseudo-Hurler disease’, and ‘Tay-Sachs disease with visceral involvement’. Am J Dis Child 108:503–522
Leroy JG, Sillence D, Wood T et al (2014) A novel intermediate mucolipidosis II/IIIalphabeta caused by GNPTAB mutation in the cytosolic N-terminal domain. Eur J Hum Genet 22:594–601
Taber P, Gyepes MT, Philippart M et al (1973) Roentgenographic manifestations of Leroy’s I-cell disease. Am J Roentgenol Radium Ther Nucl Med 118:213–221
Lin MH-C, Pitukcheewanont P (2012) Mucolipidosis type II (I-cell disease) masquerading as rickets: two case reports and review of literature. J Pediatr Endocrinol Metab 25:191–195
Pazzaglia UE, Beluffi G, Danesino C et al (1989) Neonatal mucolipidosis 2. The spontaneous evolution of early bone lesions and the effect of vitamin D treatment. Report of two cases. Pediatr Radiol 20:80–84
Pazzaglia UE, Beluffi G, Campbell JB et al (1989) Mucolipidosis II: correlation between radiological features and histopathology of the bones. Pediatr Radiol 19:406–413
Alegra T, Cury G, Todeschini LA et al (2013) Should neonatal hyperparathyroidism associated with mucolipidosis II/III be treated pharmacologically? J Pediatr Endocrinol Metab 26:1011–1013
Sathasivam A, Garibaldi L, Murphy R et al (2006) Transient neonatal hyperparathyroidism: a presenting feature of mucolipidosis type II. J Pediatr Endocrinol Metab 19:859–862
Saul RA, Proud V, Taylor HA et al (2005) Prenatal mucolipidosis type II (I-cell disease) can present as Pacman dysplasia. Am J Med Genet A 135:328–332
Lachman R, Taybi H (2006) Taybi and Lachman’s radiology of syndromes, metabolic disorders, and skeletal dysplasias, 5th edn. Mosby, Philadelphia
Acknowledgments
The authors wish to thank Tess Batchelder for her diligent help on the manuscript and the creation of the tables and other associated research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Additional information
The authors wish to dedicate this work to Dr. Walter Berdon, teacher and mentor but especially good friend.
Rights and permissions
About this article

Cite this article
Lai, L.M., Lachman, R.S. Early characteristic radiographic changes in mucolipidosis II. Pediatr Radiol 46, 1713–1720 (2016). https://doi.org/10.1007/s00247-016-3673-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-016-3673-0