
Abstract
Introduction
Because of the nonspecific symptoms and unapparent radiographic findings, occult osteoporotic vertebral fractures (VFs) have a high rate of missed diagnosis, and the treatment of these fractures has rarely been discussed in the literature. We investigated diagnostic key factors of such occult VFs and evaluated the effects of cement augmentation in these patients.
Methods
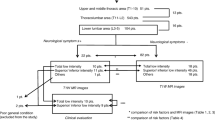
A total of 225 patients with VFs treated with vertebroplasty (VP) or kyphoplasty (KP) were retrospectively analyzed. All patients have taken preoperatively magnetic resonance imaging (MRI) including T1/T2-weighted images and short tau inversion recovery (STIR) sequences, and 45 patients met the inclusion criteria. Clinical outcomes were evaluated by comparing visual analog scale (VAS) and Oswestry disability index (ODI) values preoperatively, postoperatively, and at the final follow-up.
Results
MRI (T1 and STIR sequences) showed bone marrow edema in all fresh fractures including occult VFs and concomitant VFs; five patients showed no abnormality signal in their T2-weighted sequences of occult VFs. While 40 patients underwent KP, and five patients underwent VP. We did not find delayed collapsed fractures in the augmented occult VFs in both groups after operation. Both groups had significant improvement in pain and functional activity after the intervention (p<0.01).
Conclusion
The presence of previous or concomitant VFs leads to further imaging examination, which helps identify the occult VFs. Preoperative MRI examination especially T1 and STIR sequences plays a vital role in the early diagnosis of occult VFs. Except for significant pain relief and functional improvement, VP and KP can effectively prevent delayed vertebral collapse of occult VFs comparing to previous reported data.




Similar content being viewed by others


References
Center JR, Nguyen TV, Schneider D et al (1999) Mortality after all major types of osteoporotic fracture in men and women: an observational study. Lancet 353:878–882
Bliuc D, Nguyen ND, Milch VE et al (2009) Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA 301:513–521
Buchbinder R, Osborne RH, Ebeling PR et al (2009) A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N Engl J Med 361:557–568
Kallmes DF, Comstock BA, Heagerty PJ et al (2009) A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med 361:569–579
Hulme PA, Krebs J, Ferguson SJ et al (2006) Vertebroplasty and kyphoplasty: a systematic review of 69 clinical studies. Spine 31:1983–2001
Lee MJ, Dumonski M, Cahill P et al (2009) Percutaneous treatment of vertebral compression fractures: a meta-analysis of complications. Spine 34:1228–1232
McKiernan FE (2009) The broadening spectrum of osteoporotic vertebral fracture. Skeletal Radiol 38:303–308
Spiegl UJ, Beisse R, Hauck S et al (2009) Value of MRI imaging prior to a kyphoplasty for osteoporotic insufficiency fractures. Eur Spine J 18:1287–1292
Benz BK, Gemery JM, McIntyre JJ et al (2009) Value of immediate preprocedure magnetic resonance imaging in patients scheduled to undergo vertebroplasty or kyphoplasty. Spine 34:609–612
Pham T, Azulay-Parrado J, Champsaur P et al (2005) “Occult” osteoporotic vertebral fractures: vertebral body fractures without radiologic collapse. Spine 30:2430–2435
Belkoff SM, Jasper LE, Stevens SS (2002) An ex vivo evaluation of an inflatable bone tamp used to reduce fractures within vertebral bodies under load. Spine 27:1640–1643
Belkoff SM, Mathis JM, Jasper LE et al (2001) The biomechanics of vertebroplasty. The effect of cement volume on mechanical behavior. Spine 26:1537–1541
Klazen CA, Lohle PN, de Vries J et al (2010) Vertebroplasty versus conservative treatment in acute osteoporotic vertebral compression fractures (Vertos II): an open-label randomised trial. Lancet 376(9746):1085–1092
Yang X, Mi S, Mahadevia AA et al (2008) Pain reduction in osteoporotic patients with vertebral pain without measurable compression. Neuroradiology 50:153–159
Genant HK, Wu CY, van Kuijk C et al (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8:1137–1148
Do HM (2000) Magnetic resonance imaging in the evaluation of patients for percutaneous vertebroplasty. Top Magn Reson Imaging 11:235–244
Tanigawa N, Komemushi A, Kariya S et al (2006) Percutaneous vertebroplasty: relationship between vertebral body bone marrow edema pattern on MR images and initial clinical response. Radiology 239:195–200
Fairbank JC, Pynsent PB (2000) The Oswestry disability index. Spine 25:2940–2952
Yang HL, Wang GL, Niu GQ et al (2008) Using MRI to determine painful vertebrae to be treated by kyphoplasty in multiple-level vertebral compression fractures: a prospective study. J Int Med Res 36:1056–1063
Zou J, Mei X, Gan M et al (2010) Is kyphoplasty reliable for osteoporotic vertebral compression fracture with vertebral wall deficiency? Injury 41:360–364
Antonacci MD, Mody DR, Rutz K et al (2002) A histologic study of fractured human vertebral bodies. J Spinal Disord Tech 15:118–126
Chou LH, Knight RQ (1997) Idiopathic avascular necrosis of a vertebral body. Case report and literature review. Spine 22:1928–1932
Prakash PLV, Saralaya VV et al (2007) Vertebral body integrity: a review of various anatomical factors involved in the lumbar region. Osteoporos Int 18:891–903
Wang G, Yang H, Chen K (2010) Osteoporotic vertebral compression fractures with an intravertebral cleft treated by percutaneous balloon kyphoplasty. J Bone Joint Surg Br 92:1553–1557
Yu CW, Hsu CY, Shih TT et al (2007) Vertebral osteonecrosis: MR imaging findings and related changes on adjacent levels. AJNR Am J Neuroradiol 28:42–47
Conflict of interest
We declare that we have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
H. Mao and J. Zou contributed equally to this work
Rights and permissions
About this article
Cite this article
Mao, H., Zou, J., Geng, D. et al. Osteoporotic vertebral fractures without compression: key factors of diagnosis and initial outcome of treatment with cement augmentation. Neuroradiology 54, 1137–1143 (2012). https://doi.org/10.1007/s00234-012-1018-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00234-012-1018-8