
Abstract
Introdution
Medical technology has benefited many types of patients, but trauma care has arguably benefited more from technologic development than almost any other field.
Methods
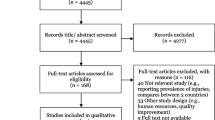
A literature review to identify key technological advances in the care of trauma patients was performed.
Results
The advances in trauma care are in great measure due to the integration of many different systems. Medical technology impacts care in the field at the site of the trauma, in the transport to trauma facilities, and care at the trauma center itself. Once at the hospital, technology has impacted care in the trauma bay, intensive care units, the operating room, and in postoperative and long-term care settings. The integration of advancements, however, needs to be examined in a careful systematic fashion to insure that patients will actually derive benefit.
Similar content being viewed by others


Premedical care
Aeromedical transport
Prehospital trauma services follow a centripetal paradigm. Most early preventable trauma death is from noncompressible cavitary hemorrhage. Emergency medical services (EMS) systems and integrated aeromedical transport that can quickly transfer bleeding patients to definitive care are critical technical assets to prehospital care.
Although, in general, “faster is better,” a commonly applied principle is that bleeding patients should reach definitive care during the “golden hour” after injury. This concept has been around for many years and rapid transport to level 1 trauma centers improves outcomes. Aeromedical transport has generally extended the 1-h radii of hospitals from 45 miles by ground to 150 miles by air evacuation [1–4]. Thus, aeromedical transport systems have been shown to reduce mortality, particularly when distances are greater than 45 miles or when ground transport is not possible [5]. The use of air transport in urban settings has not demonstrated clear benefits, most likely due to the dilution of effects by the inappropriate triage of patients with minor injuries [6–9]. Bledsoe et al. [10] showed that 60% of patients transported by air had minor injuries only and 25% of patients required less than 24 h of hospital care. Aeromedical operational costs are in excess of $5,000 per hour, making the over-utilization of these services very costly. Moreover, aeromedical personnel often put themselves at risk to deliver timely care and several are injured or killed every year. One important future improvement in air transport should be the rigorous applications of care algorithms that define candidates for air transport and enact peer review of requests. Technical advances in scene care delivered via telepresence may help bring the needed expertise in triage to the injury scene. Despite these controversies, we expect aeromedical evacuation to remain an important aspect of trauma technology for the foreseeable future.
Telemedicine
The rapid advancement of telecommunications technology over the last 20 years has allowed the simultaneous emergence of telemedicine. This initially began in the 1960s with early medical data transmission from space via National Aeronautics and Space Administration (NASA) technology. The technology was applied to military endeavors in the 1990s, most recently reaching civilian healthcare. The electronic transfer of medical records and imaging and audiovisual data from one location to another has now become commonplace. Currently, 12-lead electrocardiogram (ECG) and echocardiogram images are routinely transmitted from the field to receiving hospitals. Focused Assessment with Sonography for Trauma (FAST) images from a remote location using a laptop with cellular phone tethering can also be transmitted using a satellite network to tertiary facilities [11, 12]. These solutions are a few of the numerous examples of cost-effective methods of transmitting real-time field data to expedite therapy [11, 13].
The concept of “telepresence” is currently being explored in intensive care unit (ICU) settings, the operating room, and the trauma bay. Level 1 trauma centers extend their expertise by guiding trauma resuscitations at community hospitals using bidirectional audiovisual equipment. Telepresence may improve patient care and lower the cost of care, but prospective evidence is still needed [14, 15]. Perhaps one of the most sophisticated applications of “telepresence” is the concept of “telesurgery.” Telesurgery has been used for femoral artery repair, gastrotomy closure, cholecystectomy, liver laceration repair, and enterotomy diagnosis. However, the telesurgical operative time is three times longer than conventional surgery and on-site assistance is still required. Nonetheless, future applications may well be possible in “austere environments.” Many limitations still exist in regard to the widespread development of telemedicine. Cost, staffing, malpractice, establishing reliable communications systems, and the lack of prospective evidence have been contributing factors [16, 17].
Resuscitation and hemorrhage control
Rapid warmers/infusers
Rapid infusers/blood and fluid warming systems have been developed that use mounted chambers to provide a constant flow of either blood or resuscitation fluids at constant pressures while, at the same time, applying fluid through a counter-current heat exchanger at 42° to provide stable heating. The use of these devices has become routine in the trauma bay. They are effective at administering large amounts of blood products and maintaining normothermia with little risk of hemolysis [18–21]. This approach can avoid the contribution of hypothermia due to cold fluids to trauma-induced coagulopathy or “TIC” [22].
Hemostatic compounds
Topical hemostatic compounds can be useful when cautery or sutures are impractical in an area to attain hemostasis. Regenerated oxidized cellulose is frequently used in these situations. It is supplied as a knitted strip that can be trimmed to the desired size. The cellulose activates the clotting cascade by direct contact and its acidic pH is thought to contribute to bactericidal activity. Gelatin-based compounds can also be useful, as they can spread into the contours of a bleeding surface. The paste covering the target structure can easily be removed, if desired, using a suction device, leaving residual hemostatic particles that enabling better visualization [23, 24]. Fibrillar collagen-based materials are also available that can be similarly used. Another type of hemostatic compound is a combination of bovine-derived gelatin mixed with human-derived thrombin. This can be directly applied to an area by a syringe and it works through two mechanisms—the direct effects of thrombin and a tamponade effect secondary to the swelling of the granules. It can achieve hemostasis quickly and has few side effects. The granules are absorbed within 6–8 weeks. It was initially used in cardiac surgery and its use has been described in abdominal surgery as well [25, 26].
Fibrin glues were originally made noncommercially from cryoprecipitate and bovine thrombin, but are now made from commercially available human fibrinogen and thrombin [27]. Fibrinolysis inhibitors such as aprotinin can be added, but there is no prospective research showing the efficacy of this combination. In general, research showing outcomes improvement due to the use of any of these biomaterials or devices in trauma is lacking.
Angiographic embolization of bleeding
Unstable trauma patients can have surgically inaccessible bleeding encountered in cases of pelvic fractures, major liver injuries, or retroperitoneal bleeds. These injuries tend to be associated with high rates of morbidity and mortality, and traditional operative approaches have led to poor outcomes [28]. With the advent of modern interventional radiology (IR) though, previously inaccessible or occult bleeding arteries can be commonly controlled, often avoiding the need for operations that can, in fact, remove tamponade from venous structures, thus, worsening the bleeding. This approach has been shown to lead to improved outcomes in large studies [29]. Normotensive patients with suspected ongoing interstitial or parenchymal bleeding are often assessed using computed tomography (CT) scans to localize target areas for IR [30]. The rapid appearance of a “blush” is best seen on early-phase CT scans.
There are also, however, situations where the direct transport of patients from the emergency department (ED) to the angiography suite is preferred, as long as those areas are capable of critical care. Hypotensive patients with pelvic fractures and no blood seen on FAST examination are ideal examples. Angiography may be fruitful even where there is no extravasation seen on CT scan in unstable patients and delayed CT images looking for contrast accumulation in suspect areas may be helpful in localizing “puddling” from slower bleeding [31]. Again, this depends upon local logistics and the ability to care for sick patients in radiology. The IR control of parenchymal liver and spleen injuries leads, by necessity, to some tissue infarction. Thus, it has also been associated with significant localized morbidity and mortality. These may be simple associations however, since the patients are typically very ill individuals. Moreover, mortality increases are also associated with delays in treatment and the increasing need for transfusions [32]. However, complications like the bilomas seen after the embolization of hepatic injuries may simply be “diseases of survivorship,” representing the natural history of the injury in patients who have survived due to hemorrhage control. In any case, rapid access to IR has been shown to be critical to trauma care, and the ability to mobilize an on-call IR team has been shown to be essential [33].
Operative techniques
Endovascular techniques in trauma
Endovascular interventions for both peripheral and central vascular trauma are becoming increasingly commonplace. Peripheral interventions are particularly helpful in difficult-to-reach areas, such as the subclavian vessels, the neck, and the lower extremities. However, it is not helpful in situations where a wire cannot cross the injury or if that vessel cannot be embolized. In injuries where operative debridement is still needed, endovascular interventions can be used to gain hemostatic control either definitively or with balloon occlusion before opening [34]. Thoracic aortic injuries are also common in blunt force injuries. The endovascular repair of injuries to the traumatic thoracic aorta (TEVAR) offers a survival advantage and reduction in major morbidity, including paraplegia. Furthermore, TEVAR may be less expensive than open surgery, but endovascular procedures require a sophisticated multidisciplinary team to be available on trauma call. Hybrid operating rooms may represent the ideal setting for traumatic endovascular procedures [35].
As endovascular techniques become the norm in elective vascular procedures, the “trade-offs” inherent in using them to control traumatic injuries are likely to depend upon the long-term patency of the vessel. These considerations need to be recognized even at our early time point. For instance, the risks of open operation in subclavian-axillary injuries coupled with the proliferation of collateral vessels in the area make the endovascular repair of trauma intrinsically attractive. In contrast, the vast majority of femoral artery injuries are easily amenable to direct local control and end-to-end repair. Thus, the youth of trauma patients and the limited long-term patency of current medium and small endovascular prostheses favor open repair. Our concern is that the evolution of elective vascular surgery for organic disease away from open procedures may lead to the loss of this important skill set and worse long-term outcomes.
Laparoscopy
Endoscopy has become an important part of almost every field of surgery and plays a central role in general surgery. It is used far less in trauma surgery, in great measure due to inherent problems with the lack of visibility and hemorrhage control. Laparoscopy has been reported for use in specific blunt and penetrating traumatic injuries. Laparoscopic splenectomy in trauma has been reported, but laparoscopic vision is markedly impaired in the face of bleeding, and laparoscopy can actually cause the recurrence of splenic bleeding after spontaneous hemostasis and has led to splenectomies that were otherwise unneeded [36–38]. So, with the evolution of the nonoperative management of hemodynamically stable trauma and the IR management of visceral bleeding, it should be axiomatic at this point that any splenic injury which can be managed by laparoscopy does not require surgery at all.
In our experience, one of the more rational uses of laparoscopic techniques in trauma may be thoracoscopy for the repair of diaphragmatic injuries [39]. There have also been attempts to use diagnostic laparoscopy to assess penetrating abdominal injuries in hemodynamically stable patients [40, 41]. The rate of negative laparoscopy is high though, and many of the injuries found in stable patients are clinically insignificant, so most patients can be managed expectantly with serial examinations at much lower cost and with far less morbidity. In patients with clear peritoneal penetration, there is no difference in hospital costs, mortality, or recovery time between laparotomy and laparoscopy [42]. Thus, considering that complete laparoscopic evaluation of the bowel is tedious and carries risk for missed injuries, our practice is not to perform laparoscopy routinely for traumatic injuries. Rather, patients with obvious high-risk peritoneal violation undergo laparotomy. Patients with tangential truncal injuries are better imaged by CT [43]. Stable patients at risk for peritoneal violation can be observed without risk as long as individuals who develop signs of intra-abdominal injury undergo laparotomy promptly.
Surgical stapling devices
The use of surgical stapling devices has become universal in trauma. Gastrointestinal anastomotic staplers come in different lengths and staple spacing based on the thickness of the tissue and place two double-staggered rows of titanium staples and simultaneously cut and divide the tissues between the two double rows. These can be used for bowel, lung, and vascular pedicles. The thoracoabdominal stapler is an alternative stapler whose shape and angulation make it useful in difficult spaces such as deep in the pelvis and in the left upper quadrant [44]. Most devices are now also made in configurations that can be angulated. Surgical stapling devices have a speed advantage over hand-sewn anastomoses and have been used in a wide range of general and thoracic surgery procedures [45]. Surgical stapling devices have been shown in some studies to have a lower rate of anastomotic leak for bowel resections, particularly in cancer surgery [46].
However, the results in trauma surgery are equivocal. Conflicting multi-institutional reviews show either no difference in anastomotic leak rates or an increased rate among stapled anastomoses [47, 48]. Of importance, staplers are likely a poor choice in edematous tissue, as can occur in shock. So, anastomoses are often best deferred in this situation or hand-sewn.
Tissue sealing devices
Vessel sealing and tissue fusion devices were introduced in the late 1990s. They apply high current and low voltage to vessel walls while they are being held in tight apposition under pressure to produce a unique seal. The applied energy denatures collagen and elastin within the vessel walls and the surrounding connective tissue, and the pressure causes the denatured protein to reform with the walls in apposition into a seal that may then be transected by the instrument [49]. Vessels up to 7 mm in size can be sealed with this system. Vessel sealing devices have also become increasingly used in elective open and laparoscopic general surgery procedures, including gastrectomies, colectomies, adrenalectomies, and splenectomies. They have been shown to be cost-effective when compared to other techniques and devices, mostly because it saves time and decreases blood loss [50–53].
The speed advantages seen in general surgery have also been shown to carry over to trauma [54]. So, these devices have been used increasingly commonly in trauma and we use them commonly during trauma laparotomies, particularly to divide bowel mesentery and, occasionally, to divide the splenic hilum. Lastly, coagulation without division is a very effective technique in coagulopathies where needle hole bleeding can be troublesome.
Argon beam coagulator
The argon beam coagulator delivers a monopolar current to tissue via an ionized channel of argon gas that flows between an electrode and the tissue surface. It delivers radiofrequency (RF) electrical energy to tissues across a jet of argon gas, facilitating noncontact, monopolar, electrothermal hemostasis. The major advantages are control of the depth of penetration and the lack of contact by an electrode that can pull the coagulum off the tissue. The argon beam has been in laparoscopic and open situations for splenic salvage. It is widely used to achieve hemostasis in elective hepatic surgery, but there are no studies investigating that indication in trauma [55–57].
Vacuum-assisted closure devices
Vacuum-assisted closure (VAC) devices for wounds have become an integral part of the inpatient and outpatient care of trauma patients over the past decade. VAC devices use semi-occlusive dressings and a polyurethane foam sponge with a resting pore size of 400–600 mm to deliver suction forces typically in the range of 125 mmHg. They have been shown to increase wound angiogenesis and neovascularization [58, 59]. VAC devices have been shown lead to faster primary closure and a higher rate of primary closure than traditional wet-to-dry dressings, as well as shorter time to skin grafting, decreased length of hospital stay, greater patient satisfaction, and quicker time to rehabilitation [60].
VAC dressings can be particularly beneficial in treating deep cavitary defects due to injury. Such deep defects can often be converted to superficial defects by preventing premature walling off of the deeper cavity. This can allow for delayed primary or secondary closure of the wound defects without the need for increasing the size of the superficial wound to facilitate drainage [61]. VAC devices have also been noted to help close complex open abdominal wounds. These benefits have been suggested to occur through the reduction of edema, increased blood flow, decreased bacterial colonization, and the reduction of wound size. They can also be useful in abdominal wall reconstruction after damage control laparotomy [62].
Hemodynamic monitoring
The search for less invasive PAC replacements
No discussion of hemodynamic monitoring technology would be complete without mention of the Swan–Ganz or pulmonary artery catheter (PAC). PACs revolutionized our clinical understanding of hemodynamic function and were an integral part of critical care medicine in the 1980s and 1990s. The PAC was shown to improve outcomes in prospective randomized studies and the use of the PAC in the ICU care became widely accepted [63]. Outcome benefits were never firmly established though, and when studies carried out decades later using different study populations failed to confirm benefit, it led to a widespread search for replacements [64, 65]. Replacing the array of data gathered by the PAC is difficult. Thermodilution PACs allow the clinician to assess or derive cardiac output, right ventricular ejection fraction and end-diastolic volume, mixed venous oxygen saturation, central venous, pulmonary arterial, and pulmonary capillary wedge pressures, systemic and pulmonary vascular resistance, as well as systemic oxygen delivery and consumption. The strategy of novel monitoring technologies has become to obtain the same or related hemodynamic parameters in “less invasive” ways.
Echocardiography
Echocardiography predates the 1960s, but its use has been modernized in critical care. Two-dimensional images combined with Doppler ultrasound provide information regarding vascular volume status, cardiac physiology, and anatomy. Echocardiography can also be used to diagnose other pathologies, such as aortic dissection and pulmonary emboli. Transesophageal echocardiography can be used to calculate dynamic parameters such as cardiac output, cardiac index, stroke volume, heart rate, and corrected flow [66]. This has led to improvements in patient outcome and shorter hospital stays after major operations [67, 68]. It is still unclear whether improvements in clinical outcomes are related to esophageal doppler monitoring itself or the goal-directed therapy based on it, but combined use has proven to be advantageous to patient care.
Pulse contour cardiac output technology
Cardiac output can be estimated using arterial pressure waveform monitors placed in the proximal arterial system. The contour of the waveform can be used to estimate stroke volume by the integration of the pressure wave from end diastole to end systole. Aortic impedance is critical to the determination of stroke volume and cardiac output. The two commercially available technologies, the Pulse-induced contour cardiac output (PiCCO) monitor (Pulsion Medical, Munich, Germany) and FloTrac/Vigileo (Edwards, Irvine, CA, USA), have important differences in their approach to measuring aortic impedance. PiCCO does not adjust for aortic impedance changes that occur over time. Instead, it calibrates to thermodilution measurements done every 20–30 min. The FloTrac/Vigileo system estimates aortic impedance by the arterial pressure waveform and the patient’s demographics: age, gender, height, and weight. This system is convenient in that it does not require calibration, but it also has not proved to be as accurate as the PiCCO in unstable patients [69, 70].
The extravascular lung water (EVLW), global end-diastolic volume, intra-thoracic lung volume, and pulmonary thermal volume can also be calculated by pulse contour systems, and may prove to be useful measures of volume status and lung water. EVLW may detect pulmonary edema early, and may be an indicator of mortality in acute lung injury or severe sepsis [71–73]. EVLW has been used to guide fluid management in acute respiratory distress syndrome and subarachnoid hemorrhage [74–77]. An important drawback to both systems, however, is that data interpretation is unreliable in the setting of common tachyarrhythmias like atrial fibrillation. Moreover, both products require proximal arterial access. Thus, the extent to which they are “less invasive” than PACs is debatable.
Non-invasive cardiac output
Use of the Fick dilution technique requires an indicator like Cardio-Green dye or cold injected saline to calculate the cardiac output. The Fick principle, however, can also be applied to a gas diffusing through the lungs. The Non-invasive cardiac output (NICO) sensor (Novametrix Medical Systems, Wallingford, CT, USA) utilizes partial rebreathing of an additional 150 ml of dead space in the ventilator circuit and an infrared sensor to calculate minute ventilation and content of arterial and venous carbon dioxide (CaCO2, CvCO2). The system relies on a stable CO2 dissociation curve, a constant mixed venous CO2 content, and a constant dead space. Furthermore, changes in the pulmonary capillary blood flow and the shunt fraction may affect the accuracy of cardiac output estimates [78]. Experimental studies report conflicting data regarding the agreement of the measured outputs with validated methods like thermodilution. Hesitancy in adopting the technology has largely been due to the perceived inaccuracy of the CO2 indicator itself, thus, limiting its applicability [79–81].
Organ support
A significant proportion of critically ill patients suffer from multisystem organ failure (MOF). Clinical outcomes are strongly correlated with the number of organ systems in failure [82, 83]. Advances in medical care have been directed at both supporting and replacing dysfunctional organs. Pioneered by advances in renal replacement therapy and dialysis, the ability to support cardiopulmonary, hepatic, and neurologic function still represents the horizon of technologic advancement.
ECMO
Extracorporeal membrane oxygenation (ECMO) is the most invasive form of cardiopulmonary support. Widely used in neonatal and pediatric populations, its use has broadened to include critically ill adults needing bridging therapy for life-threatening cardiopulmonary failure. Arteriovenous ECMO may be used for cardiac failure, whereas venovenous ECMO is used primarily for the support of failing oxygenation. ECMO is either configured peripherally using the femoral artery and vein, or centrally either through an open chest or via tunneled subcostal cannula into the right or left atria. Central ECMO establishes antegrade flow through the aortic arch and coronary vessels, decreasing right ventricular afterload and left ventricular preload. Central ECMO also achieves higher flow and there is less mixing of oxygenated and deoxygenated blood compared to when using peripheral access. ECMO is beset with a myriad of complications: bleeding, coagulopathy, clotting, sepsis, and peripheral or splanchnic ischemia are frequent, as are technical problems with the system [84].
Most importantly, data supporting ECMO use in adults is limited. After two randomized controlled trials failed to show the benefit of adult ECMO, the 2009 CESAR study published data in support of ECMO use in adult respiratory failure, but there were many problems with the trial [85, 86]. Observational studies have also suggested potential advantages of ECMO after cardiac arrest [87, 88]. Long-term functional outcomes are similar to hemodialysis and acute respiratory distress syndrome (ARDS) survivors [89, 90]. Hand-held portable ECMO and extracorporeal lung assist devices have been reported [91, 92].
Circulatory assist devices
Mechanical assist devices have greatly changed the therapy of the failing heart. Intra-aortic balloon pumps (IABPs) and ventricular assist devices (VADs) have emerged as important therapies.
Intra-aortic balloon pump
The IABP is a mechanical hemodynamic support device that is well established in the care of patients with poor left ventricular ejection fractions. The device supplies two major benefits to cardiac function. Diastolic insufflation increases the filling of the proximal aorta and coronaries. Desufflation during systole decreases afterload by inducing a vacuum in the proximal aorta. Due to the lack of clinical equipoise, randomized controlled trials of IABPs in the postoperative setting have never been performed. Preoperative IABP use has extended to patients with unstable angina, those who have undergone percutaneous coronary interventions, or who are awaiting coronary artery bypass surgery. IABP use prior to coronary artery bypass surgery has been shown to decrease mortality and improve postoperative cardiac output [93].
Ventricular assist devices
First introduced in the 1990s, larger pulsatile positive displacement pumps were transitioned into the smaller “second-generation” nonpulsatile continuous flow pumps. Each subsequent generation has been reduced in the size and the number of mobile parts. Third-generation pumps, currently on trial in Europe, have only one mobile part, thus, greatly increasing the durability of the device and decreasing the size to allow for intra-pericardial implantation. The outcomes of mechanical circulatory devices have been evaluated in a variety of patient populations, including bridge to transplantation or possible transplant, bridge to recovery, and long-term permanent destination therapy [94]. The Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure (REMATCH) trial was the landmark study of New York Heart Association (NYHA) class 4 heart failure patients. This randomized trial demonstrated that those patients with ventricular assistance showed improved quality of life and, more importantly, an increased survival benefit from 25 to 52% over 1 year compared to medical therapy [95]. Second-generation, continuous-flow left ventricular assist devices (LVADs) were evaluated compared to first-generation models. The results showed a survival benefit of 68% versus 52% at 1 year and 58% versus 24% after 2 years [96–98]. The risk of device failure and stroke were decreased with newer ventricular assist devices. The Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) continues to follow all data from U.S. Food and Drug Administration (FDA)-approved devices. The continued monitoring of outcomes as devices evolve will help better stratify risk, identify the optimal patients for implantation, and target complications in order to help further the technology [99, 100].
Ventilators
A full review of advances in mechanical ventilation is beyond the scope of this work, but microprocessor control of ventilation has radically improved our ability to support the failing lung. Microprocessor-based ventilation allows for the precise real-time control of inspiratory pressure and flow, as well as of expiratory airway pressure. The graphic depictions generated with each breathing cycle make the interface between machine and clinician more intuitive, but the future of ventilators may lead away from such frequent clinical interventions. Sophisticated microprocessors allow the creation of increasingly advanced programs optimizing ventilator support and weaning. Closed-loop controls assist basic ventilator functions by the regulation of inspiratory pressure and flow multiple times during each breath. Using algorithmically derived “target” values, ventilators can equilibrate patient responses towards the target responses, as well as adapt to the patient’s underlying pathophysiology, thus, diminishing ventilator-induced lung injury, optimizing the work of breathing, and enhancing patient–ventilator synchrony [101, 102]. These functions can now be used to transition patients from control modes to support modes and wean them towards extubation [103]. Microprocessor–based weaning systems now “on the horizon” can make use of patient information like age, weight, central nervous system function, and the presence of pre-existing lung dysfunction to create staged algorithms for patient weaning. A typical algorithm might use pressure support to target a PCO2, tidal volume, or respiratory rate before automatically introducing spontaneous breathing trials [104]. Recent work suggests that such an approach can lead to improved respiratory mechanics, fewer ventilator days, and decreased ICU length of stay [105, 106].
Two additional experimental models that are on the horizon of ventilator technology are neurally adjusted ventilatory assist (NAVA) control and artificial neural networks. NAVA control is an experimental model of ventilation that synchronizes with the electromyography (EMG) activity of the diaphragm to control the inspiratory timing and pressure. The ventilator is able to synchronize with the patient’s respiratory efforts. Limited human data exists to verify this mode of ventilation, but, nonetheless, it is an exciting development. Artificial neural networks are data integration systems similar to the synaptic networks of the brain. Multiple inputs can be summed to either encourage or inhibit a response. In essence, artificial intelligence can allow the ventilator to learn from real-time, patient-triggered cues [107, 108].
Renal and liver replacement therapy
Renal failure is a frequent complication in severely injured trauma patients, some of whom require renal replacement therapy. Malnutrition, Injury Severity Score (ISS), polyorgan system dysfunction, and sepsis all predispose to acute renal failure. Acute renal failure in the trauma population has a high mortality, which is correlated with other organ system dysfunction, particularly cardiac and pulmonary [109, 110]. Continuous renal replacement therapy has been traditionally used rather than intermittent hemodialysis in patients with labile blood pressures; however, there is conflicting retrospective evidence as to the benefit of routine use, with prospective data showing no difference in outcomes [110–113]. This, combined with high cost, has led to many centers, including ours, preferentially using intermittent dialysis where applicable [110]. Prospective data in the trauma population is needed.
Liver replacement therapy has been tried by multiple modalities, including hemodialysis, hemodiabsorption, and plasmaphoresis and plasma exchange, with little success. However, no method has been shown to improve survival and it is not a therapy that we use [114, 115]. Unfortunately, our care for hepatic failure in the trauma patient is only supportive unless they meet criteria for transplantation.
Conclusion
Technological advances improved the care of the trauma patient in the prehospital, trauma bay, intraoperative, and inpatient care. Future advances in first responder technology, less invasive and faster surgical techniques and devices, as well as multiorgan system support are continuously being developed. However, their potential improvement in patient care, as well as a significant portion of the current technology, needs to be assessed in a systematic prospective fashion.
References
Olson CJ, Brand D, Mullins RJ, Harrahill M, Trunkey DD. Time to death of hospitalized injured patients as a measure of quality of care. J Trauma. 2003;55(1):45–52.
The Trauma Center Association of America. Trauma’s golden hour. Home page at: http://www.traumafoundation.org. Accessed May 1, 2011.
Demetriades D, Martin M, Salim A, Rhee P, Brown C, Chan L. The effect of trauma center designation and trauma volume on outcome in specific severe injuries. Ann Surg. 2005;242:512–9.
McKenney MG, Livingstone AS, Schulman C, Stahl K, Lineen E, Namias N, Augenstein J. Trauma surgeon mortality rates correlate with surgeon time at institution. J Am Coll Surg. 2009;208(5):750–3. Discussion 753–4.
Boyd CR, Corse KM, Campbell RC. Emergency interhospital transport of the major trauma patient: air versus ground. J Trauma. 1989;29:789–94.
Nicholl JP, Brazier JE, Snooks HA. Effects of London helicopter emergency medical service on survival after trauma. BMJ. 1995;311:217–22.
Schiller WR, Knox R, Zinnecker H, Jeevanandam M, Sayre M, Burke J, Young DH. Effect of helicopter transport of trauma victims on survival in an urban trauma center. J Trauma. 1988;28:1127–34.
Cunningham P, Rutledge R, Baker CC, Clancy TV. A comparison of the association of helicopter and ground ambulance transport with the outcome of injury in trauma patients transported from the scene. J Trauma. 1997;43:940–6.
Brathwaite CE, Rosko M, McDowell R, Gallagher J, Proenca J, Spott MA. A critical analysis of on-scene helicopter transport on survival in a statewide trauma system. J Trauma. 1998;45:140–6.
Bledsoe BE, Wesley AK, Eckstein M, Dunn TM, O’Keefe MF. Helicopter scene transport of trauma patients with nonlife-threatening injuries: a meta-analysis. J Trauma. 2006;60(6):1257–65. Discussion 1265–6.
McBeth PB, Hamilton T, Kirkpatrick AW. Cost-effective remote iPhone-teathered telementored trauma telesonography. J Trauma. 2010;69(6):1597–9.
Dyer D, Cusden J, Turner C, Boyd J, Hall R, Lautner D, Hamilton DR, Shepherd L, Dunham M, Bigras A, Bigras G, McBeth P, Kirkpatrick AW. The clinical and technical evaluation of a remote telementored telesonography system during the acute resuscitation and transfer of the injured patient. J Trauma. 2008;65(6):1209–16.
Strode CA, Rubal BJ, Gerhardt RT, Christopher FL, Bulgrin JR, Kinkler ES Jr, Bauch TD, Boyd SY. Satellite and mobile wireless transmission of focused assessment with sonography in trauma. Acad Emerg Med. 2003;10:1411–4.
Duchesne JC, Kyle A, Simmons J, Islam S, Schmieg RE Jr, Olivier J, McSwain NE Jr. Impact of telemedicine upon rural trauma care. Trauma. 2008;64(1):92–7. Discussion 97–8.
Bowersox JC, Cordts PR, LaPorta AJ. Use of an intuitive telemanipulator system for remote trauma surgery: an experimental study. J Am Coll Surg. 1998;186(6):615–21.
Bowersox JC, Shah A, Jensen J, Hill J, Cordts PR, Green PS. Vascular applications of telepresence surgery: initial feasibility studies in swine. J Vasc Surg. 1996;23:281–7.
Rogers FB, Ricci M, Caputo M, Shackford S, Sartorelli K, Callas P, Dewell J, Daye S. The use of telemedicine for real-time video consultation between trauma center and community hospital in a rural setting improves early trauma care: preliminary results. J Trauma. 2001;51(6):1037–41.
Satiani B, Fried SJ, Zeeb P, Falcone RE. Normothermic rapid volume replacement in vascular catastrophes using the Infuser 37. Ann Vasc Surg. 1988;2(1):37–42.
Satiani B, Fried SJ, Zeeb P, Falcone RE. Normothermic rapid volume replacement in traumatic hypovolemia. A prospective analysis using a new device. Arch Surg. 1987;122(9):1044–7.
Falcone RE, Fried SJ, Zeeb P, Satiani B. Rapid volume replacement with warmed blood and fluids. Angiology. 1989;40(11):964–9.
Kim P, Chin-Yee I, Eckert K, Malthaner RA, Gray DK. Hemolysis with rapid transfusion systems in the trauma setting. Can J Surg. 2004;47(4):295–7.
Hess JR, Brohi K, Dutton RP, Hauser CJ, Holcomb JB, Kluger Y, Mackway-Jones K, Parr MJ, Rizoli SB, Yukioka T, Hoyt DB, Bouillon B. The coagulopathy of trauma: a review of mechanisms. J Trauma. 2008;65(4):748–54 Review.
Tomizawa Y. Clinical benefits and risk analysis of topical hemostats: a review. J Artif Organs. 2005;8(3):137–42. Review.
Sabel M, Stummer W. The use of local agents: Surgicel and Surgifoam. Eur Spine J. 2004;13(Suppl 1):S97–101. Epub 2004 May 15.
Oz MC, Rondinone JF, Shargill NS. FloSeal Matrix: new generation topical hemostatic sealant. J Card Surg. 2003;18(6):486–93. No abstract available.
Oz MC, Cosgrove DM 3rd, Badduke BR, Hill JD, Flannery MR, Palumbo R, Topic N. Controlled clinical trial of a novel haemostatic agent in cardiac surgery. The Fusion Matrix Study Group. Ann Thorac Surg. 2000;69(5):1376–82.
Hauser CJ. Hemostasis of solid viscus trauma by intraparenchymal injection of fibrin glue. Arch Surg. 1989;124(3):291–3.
Verbeek D, Sugrue M, Balogh Z, Cass D, Civil I, Harris I, Kossmann T, Leibman S, Malka V, Pohl A, Rao S, Richardson M, Schuetz M, Ursic C, Wills V. Acute management of hemodynamically unstable pelvic trauma patients: time for a change? Multicenter review of recent practice. World J Surg. 2008;32(8):1874–82.
Velmahos GC, Toutouzas KG, Vassiliu P, Sarkisyan G, Chan LS, Hanks SH, Berne TV, Demetriades D. A prospective study on the safety and efficacy of angiographic embolization for pelvic and visceral injuries. J Trauma. 2002;53(2):303–8. Discussion 308.
Pereira SJ, O’Brien DP, Luchette FA, Choe KA, Lim E, Davis K Jr, Hurst JM, Johannigman JA, Frame SB. Dynamic helical computed tomography scan accurately detects hemorrhage in patients with pelvic fracture. Surgery. 2000;128(4):678–85.
Fu CY, Wang YC, Wu SC, Chen RJ, Hsieh CH, Huang HC, Huang JC, Lu CW, Huang YC (2010) Angioembolization provides benefits in patients with concomitant unstable pelvic fracture and unstable hemodynamics. Am J Emerg Med. [Epub ahead of print]
Mohr AM, Lavery RF, Barone A, Bahramipour P, Magnotti LJ, Osband AJ, Sifri Z, Livingston DH. Angiographic embolization for liver injuries: low mortality, high morbidity. J Trauma. 2003;55(6):1077–81. Discussion 1081–2.
Wong YC, Wang LJ, Ng CJ, Tseng IC, See LC. Mortality after successful transcatheter arterial embolization in patients with unstable pelvic fractures: rate of blood transfusion as a predictive factor. J Trauma. 2000;49(1):71–5.
Johnson CA. Endovascular management of peripheral vascular trauma. Semin Intervent Radiol. 2010;27(1):38–43.
Rousseau H, Elaassar O, Marcheix B, Cron C, Chabbert V, Combelles S, Dambrin C, Leobon B, Moreno R, Otal P, Auriol J (2011) The role of stent-grafts in the management of aortic trauma. Cardiovasc Intervent Radiol. [Epub ahead of print]
Carobbi A, Romagnani F, Antonelli G, Bianchini M. Laparoscopic splenectomy for severe blunt trauma: initial experience of ten consecutive cases with a fast hemostatic technique. Surg Endosc. 2010;24(6):1325–30. Epub 2009 Dec 9.
Lujan-Mompean JA, Parrilla-Paricio P, Robles-Campos R, Torralba-Martinez JA, Sanchez-Bueno F, Arenas-Ricart J. Laparoscopic surgery in the management of traumatic hemoperitoneum in stable patients. Surg Endosc. 1995;9(8):879–81.
Hauser CJ, Poole GV, Thomae KR. Laparoscopic surgery and the management of traumatic hemoperitoneum in stable patients. Surg Endosc. 1996;10(6):694–5. No abstract available.
Matthews BD, Bui H, Harold KL, Kercher KW, Adrales G, Park A, Sing RF, Heniford BT. Laparoscopic repair of traumatic diaphragmatic injuries. Surg Endosc. 2003;17(2):254–8. Epub 2002 Oct 29.
Mallat AF, Mancini ML, Daley BJ, Enderson BL. The role of laparoscopy in trauma: a ten-year review of diagnosis and therapeutics. Am Surg. 2008;74(12):1166–70.
Ahmed N, Whelan J, Brownlee J, Chari V, Chung R. The contribution of laparoscopy in evaluation of penetrating abdominal wounds. J Am Coll Surg. 2005;201(2):213–6.
Leppäniemi A, Haapiainen R. Diagnostic laparoscopy in abdominal stab wounds: a prospective, randomized study. J Trauma. 2003;55(4):636–45.
Hauser CJ, Huprich JE, Bosco P, Gibbons L, Mansour AY, Weiss AR. Triple-contrast computed tomography in the evaluation of penetrating posterior abdominal injuries. Arch Surg. 1987;122(10):1112–5.
Uranüs S, Kronberger L, Kraft-Kine J. Partial splenic resection using the TA-stapler. Am J Surg. 1994;168(1):49–53. Review.
Laurent A, Parc Y, McNamara D, Parc R, Tiret E. Colonic J-pouch-anal anastomosis for rectal cancer: a prospective, randomized study comparing handsewn vs. stapled anastomosis. Dis Colon Rectum. 2005;48(4):729–34.
Choy PY, Bissett IP, Docherty JG, Parry BR, Merrie AE. Stapled versus handsewn methods for ileocolic anastomoses. Cochrane Database Syst Rev. 2007;18(3):CD004320. Review.
Demetriades D, Murray JA, Chan LS, Ordoñez C, Bowley D, Nagy KK, Cornwell EE 3rd, Velmahos GC, Muñoz N, Hatzitheofilou C, Schwab CW, Rodriguez A, Cornejo C, Davis KA, Namias N, Wisner DH, Ivatury RR, Moore EE, Acosta JA, Maull KI, Thomason MH, Spain DA. Handsewn versus stapled anastomosis in penetrating colon injuries requiring resection: a multicenter study. J Trauma. 2002;52(1):117–21.
Brundage SI, Jurkovich GJ, Hoyt DB, Patel NY, Ross SE, Marburger R, Stoner M, Ivatury RR, Ku J, Rutherford EJ, Maier RV; WTA Multi-institutional Study Group. Western Trauma Association. Stapled versus sutured gastrointestinal anastomoses in the trauma patient: a multicenter trial. J Trauma. 2001;51(6):1054–61.
Heniford BT, Matthews BD, Sing RF, Backus C, Pratt B, Greene FL. Initial results with an electrothermal bipolar vessel sealer. Surg Endosc. 2001;15(8):799–801. Epub 2001 May 14.
Macario A, Dexter F, Sypal J, Cosgriff N, Heniford BT. Operative time and other outcomes of the electrothermal bipolar vessel sealing system (LigaSure) versus other methods for surgical hemostasis: a meta-analysis. Surg Innov. 2008;15(4):284–91. Epub 2008 Oct 22.
Romano F, Gelmini R, Caprotti R, Andreotti A, Guaglio M, Franzoni C, Uggeri F, Saviano M. Laparoscopic splenectomy: ligasure versus EndoGIA: a comparative study. J Laparoendosc Adv Surg Tech A. 2007;17(6):763–7.
Romano F, Caprotti R, Franciosi C, De Fina S, Colombo G, Uggeri F. Laparoscopic splenectomy using Ligasure. Preliminary experience. Surg Endosc. 2002;16(11):1608–11. Epub 2002 May 3.
Marcello PW, Roberts PL, Rusin LC, Holubkov R, Schoetz DJ. Vascular pedicle ligation techniques during laparoscopic colectomy. A prospective randomized trial. Surg Endosc. 2006;20(2):263–9. Epub 2005 Dec 9.
Hope WW, Burns JM, Newcomb WL, Heniford BT, Sing RF. Safety and efficacy of the electrothermal bipolar vessel sealer in trauma. Injury. 2009;40(5):564–6. Epub 2008 May 19.
Kwon AH, Inui H, Kamiyama Y. Successful laparoscopic haemostasis using an argon beam coagulator for blunt traumatic splenic injury. Eur J Surg. 2001;167(4):316–8. No abstract available.
Dunham CM, Cornwell EE 3rd, Militello P. The role of the Argon Beam Coagulator in splenic salvage. Surg Gynecol Obstet. 1991;173(3):179–82.
Asensio JA, Roldán G, Petrone P, Rojo E, Tillou A, Kuncir E, Demetriades D, Velmahos G, Murray J, Shoemaker WC, Berne TV, Chan L. Operative management and outcomes in 103 AAST-OIS grades IV and V complex hepatic injuries: trauma surgeons still need to operate, but angioembolization helps. J Trauma. 2003;54(4):647–53. Discussion 653–4.
Labler L, Rancan M, Mica L, Härter L, Mihic-Probst D, Keel M. Vacuum-assisted closure therapy increases local interleukin-8 and vascular endothelial growth factor levels in traumatic wounds. J Trauma. 2009;66(3):749–57.
Scherer SS, Pietramaggiori G, Mathews JC, Prsa MJ, Huang S, Orgill DP. The mechanism of action of the vacuum-assisted closure device. Plast Reconstr Surg. 2008;122(3):786–97.
Zannis J, Angobaldo J, Marks M, DeFranzo A, David L, Molnar J, Argenta L. Comparison of fasciotomy wound closures using traditional dressing changes and the vacuum-assisted closure device. Ann Plast Surg. 2009;62(4):407–9.
Rispoli DM, Horne BR, Kryzak TJ, Richardson MW. Description of a technique for vacuum-assisted deep drains in the management of cavitary defects and deep infections in devastating military and civilian trauma. J Trauma. 2010;68(5):1247–52.
DeFranzo AJ, Pitzer K, Molnar JA, Marks MW, Chang MC, Miller PR, Letton RW, Argenta LC. Vacuum-assisted closure for defects of the abdominal wall. Plast Reconstr Surg. 2008;121(3):832–9.
Shoemaker WC, Kram HB, Appel PL, Fleming AW. The efficacy of central venous and pulmonary artery catheters and therapy based upon them in reducing mortality and morbidity. Arch Surg. 1990;125:1332–7. Discussion 1337–8.
Connors AF Jr, Speroff T, Dawson NV, Thomas C, Harrell FE Jr, Wagner D, Desbiens N, Goldman L, Wu AW, Califf RM, Fulkerson WJ Jr, Vidaillet H, Broste S, Bellamy P, Lynn J, Knaus WA. The effectiveness of right heart catheterization in the initial care of critically ill patients. SUPPORT Investigators. JAMA. 1996;276:889–97.
Taylor RW Jr, Calvin JE, Matuschak GM. Pulmonary Artery Catheter Consensus Conference: the first step. Crit Care Med. 1997;25:2064–5.
Daigle RE, Miller CW, Histand MB, McLeod FD, Hokanson DE. Nontraumatic aortic blood flow sensing by use of an ultrasonic esophageal probe. J Appl Physiol. 1975;38:1153–60.
Hadian M, Angus DC. Protocolized resuscitation with esophageal Doppler monitoring may improve outcome in post-cardiac surgery patients. Crit Care. 2005;9(4):E7.
Gan TJ, Soppitt A, Maroof M, el-Moalem H, Robertson KM, Moretti E, Dwane P, Glass PS. Goal-directed intraoperative fluid administration reduces length of hospital stay after major surgery. Anesthesiology. 2002;97:820–6.
Monnet X, Anguel N, Naudin B, Jabot J, Richard C, Teboul JL. Arterial pressure-based cardiac output in septic patients: different accuracy of pulse contour and uncalibrated pressure waveform devices. Crit Care. 2010;14(3):R109.
Chaney JC, Derdak S. Minimally invasive hemodynamic monitoring for the intensivist: current and emerging technology. Crit Care Med. 2002;30(10):2338–45.
Brown LM, Liu KD, Matthay MA. Measurement of extravascular lung water using the single indicator method in patients: research and potential clinical value. Am J Physiol Lung Cell Mol Physiol. 2009;297(4):L547–58.
Kuzkov VV, Kirov MY, Sovershaev MA, Kuklin VN, Suborov EV, Waerhaug K, Bjertnaes LJ. Extravascular lung water determined with single transpulmonary thermodilution correlates with the severity of sepsis-induced acute lung injury. Crit Care Med. 2006;34:1647–53.
Martin GS, Eaton S, Mealer M, Moss M. Extravascular lung water in patients with severe sepsis: a prospective cohort study. Crit Care. 2005;9:R74–82.
Mitchell JP, Schuller D, Calandrino FS, Schuster DP. Improved outcome based on fluid management in critically ill patients requiring pulmonary artery catheterization. Am Rev Respir Dis. 1992;145:990–8.
Mutoh T, Kazumata K, Ishikawa T, Terasaka S. Performance of bedside transpulmonary thermodilution monitoring for goal-directed hemodynamic management after subarachnoid hemorrhage. Stroke. 2009;40:2368–74.
Michard F, Alaya S, Zarka V, Bahloul M, Richard C, Teboul JL. Global end-diastolic volume as an indicator of cardiac preload in patients with septic shock. Chest. 2003;124(5):1900–8.
Isakow W, Schuster DP. Extravascular lung water measurements and hemodynamic monitoring in the critically ill: bedside alternatives to the pulmonary artery catheter. Am J Physiol Lung Cell Mol Physiol. 2006;291(6):L1118–31.
Berton C, Cholley B. Equipment review: new techniques for cardiac output measurement—oesophageal Doppler, Fick principle using carbon dioxide, and pulse contour analysis. Critical Care. 2002;6:216–21.
van Heerden PV, Baker S, Lim SI, Weidman C, Bulsara M. Clinical evaluation of the non-invasive cardiac output (NICO) monitor in the intensive care unit. Anaesth Intensive Care. 2000;28(4):427–30.
Burchell SA, Yu M, Takiguchi SA, Ohta RM, Myers SA. Evaluation of a continuous cardiac output and mixed venous oxygen saturation catheter in critically ill surgical patients. Crit Care Med. 1997;25:388–91.
Kotake Y, Moriyama K, Innami Y, Shimizu H, Ueda T, Morisaki H, Takeda J. Performance of noninvasive partial CO2 rebreathing cardiac output and continuous thermodilution cardiac output in patients undergoing aortic reconstruction surgery. Anesthesiology. 2003;99:283–8.
Minne L, Abu-Hanna A, de Jonge E. Evaluation of SOFA-based models for predicting mortality in the ICU: a systematic review. Crit Care. 2008;12(6):R161. Epub 2008 Dec 17.
Marshall JC, Cook DJ, Christou NV, Bernard GR, Sprung CL, Sibbald WJ. Multiple organ dysfunction score: a reliable descriptor of a complex clinical outcome. Crit Care Med. 1995;23(10):1638–52.
Marasco SF, Lukas G, McDonald M, McMillan J, Ihle B. Review of ECMO (extra corporeal membrane oxygenation) support in critically ill adult patients. Heart Lung Circ. 2008;17(Suppl 4):S41–7.
Zapol WM, Snider MT, Hill JD, Fallat RJ, Bartlett RH, Edmunds LH, Morris AH, Peirce EC 2nd, Thomas AN, Proctor HJ, Drinker PA, Pratt PC, Bagniewski A, Miller RG Jr. Extracorporeal membrane oxygenation in severe acute respiratory failure. A randomized prospective study. JAMA. 1979;242:2193–6.
Morris AH, Wallace CJ, Menlove RL, Clemmer TP, Orme JF Jr, Weaver LK, Dean NC, Thomas F, East TD, Pace NL, Suchyta MR, Beck E, Bombino M, Sittig DF, Böhm S, Hoffmann B, Becks H, Butler S, Pearl J, Rasmusson B. Randomized clinical trial of pressure-controlled inverse ratio ventilation and extracorporeal CO2 removal for adult respiratory distress syndrome. Am J Respir Crit Care Med. 1994;149:295–305.
Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, Hibbert CL, Truesdale A, Clemens F, Cooper N, Firmin RK, Elbourne D; CESAR trial collaboration. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009;374(9698):1351–63. Epub 2009 Sep 15.
Thiagarajan RR, Brogan TV, Scheurer MA, Laussen PC, Rycus PT, Bratton SL. Extracorporeal membrane oxygenation to support cardiopulmonary resuscitation in adults. Ann Thorac Surg. 2009;87:778–85.
Shin TG, Choi JH, Jo IJ, Sim MS, Song HG, Jeong YK, Song YB, Hahn JY, Choi SH, Gwon HC, Jeon ES, Sung K, Kim WS, Lee YT. Extracorporeal cardiopulmonary resuscitation in patients with inhospital cardiac arrest: a comparison with conventional cardiopulmonary resuscitation. Crit Care Med. 2011;39:1–7.
Chen YS, Lin JW, Yu HY, Ko WJ, Jerng JS, Chang WT, Chen WJ, Huang SC, Chi NH, Wang CH, Chen LC, Tsai PR, Wang SS, Hwang JJ, Lin FY. Cardiopulmonary resuscitation with assisted extracorporeal life-support versus conventional cardiopulmonary resuscitation in adults with in-hospital cardiac arrest: an observational study and propensity analysis. Lancet. 2008;372(9638):554–61. Epub 2008 Jul 4.
Arlt M, Philipp A, Voelkel S, Camboni D, Rupprecht L, Graf BM, Schmid C, Hilker M (2011) Hand-held minimised extracorporeal membrane oxygenation: a new bridge to recovery in patients with out-of-centre cardiogenic shock. Eur J Cardiothorac Surg. 40(3):689–94.
Haneya A, Philipp A, Mueller T, Lubnow M, Pfeifer M, Zink W, Hilker M, Schmid C, Hirt S. Extracorporeal circulatory systems as a bridge to lung transplantation at remote transplant centers. Ann Thorac Surg. 2011;91(1):250–5.
Theologou T, Bashir M, Rengarajan A, Khan O, Spyt T, Richens D, Field M. Preoperative intra aortic balloon pumps in patients undergoing coronary artery bypass grafting. Cochrane Database Syst Rev. 2011;19:CD004472.
Fitzpatrick JR III, Woo YJ. Mechanical circulatory assistance: an evolving therapy. Circ J. 2011;75:38–46.
Rose EA, Gelijns AC, Moskowitz AJ, Heitjan DF, Stevenson LW, Dembitsky W, Long JW, Ascheim DD, Tierney AR, Levitan RG, Watson JT, Meier P, Ronan NS, Shapiro PA, Lazar RM, Miller LW, Gupta L, Frazier OH, Desvigne-Nickens P, Oz MC, Poirier VL; Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure (REMATCH) Study Group. Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med. 2001;345:1435–43.
Lietz K. Destination therapy: patient selection and current outcomes. J Card Surg. 2010;25:462–71.
Slaughter MS, Rogers JG, Milano CA, Russell SD, Conte JV, Feldman D, Sun B, Tatooles AJ, Delgado RM 3rd, Long JW, Wozniak TC, Ghumman W, Farrar DJ, Frazier OH; HeartMate II Investigators. Advanced heart failure treated with continuous-flow left ventricular assist device. N Engl J Med. 2009;361:2241–51.
Fang JC. Rise of the machines—left ventricular assist devices as permanent therapy for advanced heart failure. N Engl J Med. 2009;361(23):2282–5.
Kirklin JK, Naftel DC, Kormos RL, Stevenson LW, Pagani FD, Miller MA, Ulisney KL, Baldwin JT, Young JB. Third INTERMACS Annual Report: the evolution of destination therapy in the United States. J Heart Lung Transplant. 2011;30(2):115–23.
Holman WL, Pae WE, Teutenberg JJ, Acker MA, Naftel DC, Sun BC, Milano CA, Kirklin JK. INTERMACS: interval analysis of registry data. J Am Coll Surg. 2009;208:755–61. Discussion 761–2.
Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) Official website at: http://www.intermacs.org/membership.aspx. Accessed February 28, 2011.
Slutsky AS, Ranieri VM. Mechanical ventilation: lessons from the ARDSNet trial. Respir Res. 2000;1:73–7.
Arnal JM, Wysocki M, Nafati C, Donati S, Granier I, Corno G, Durand-Gasselin J. Automatic selection of breathing pattern using adaptive support ventilation. Intensive Care Med. 2008;34:75–81.
Burns KE, Lellouche F, Lessard MR. Automating the weaning process with advanced closed-loop systems. Intensive Care Med. 2008;34:1757–65.
Dojat M, Harf A, Touchard D, Lemaire F, Brochard L. Clinical evaluation of a computer-controlled pressure support mode. Am J Respir Crit Care Med. 2000;161:1161–6.
Lellouche F, Mancebo J, Jolliet P, Roeseler J, Schortgen F, Dojat M, Cabello B, Bouadma L, Rodriguez P, Maggiore S, Reynaert M, Mersmann S, Brochard L. A multicenter randomized trial of computer-driven protocolized weaning from mechanical ventilation. Am J Respir Crit Care Med. 2006;174:894–900.
Snowden S, Brownlee KG, Smye SW, Dear PR. An advisory system for artificial ventilation of the newborn utilizing a neural network. Med Inform (Lond). 1993;18(4):367–76.
Chatburn RL. Computer control of mechanical ventilation. Respir Care. 2004;49(5):507–17.
Tran DD, Cuesta MA, Oe PL. Acute renal failure in patients with severe civilian trauma. Nephrol Dial Transplant. 1994;9(Suppl 4):121–5.
Rauf AA, Long KH, Gajic O, Anderson SS, Swaminathan L, Albright RC. Intermittent hemodialysis versus continuous renal replacement therapy for acute renal failure in the intensive care unit: an observational outcomes analysis. J Intensive Care Med. 2008;23(3):195–203.
Eachempati SR, Wang JC, Hydo LJ, Shou J, Barie PS. Acute renal failure in critically ill surgical patients: persistent lethality despite new modes of renal replacement therapy. J Trauma. 2007;63(5):987–93.
Swartz RD, Bustami RT, Daley JM, Gillespie BW, Port FK. Estimating the impact of renal replacement therapy choice on outcome in severe acute renal failure. Clin Nephrol. 2005;63(5):335–45.
Lins RL, Elseviers MM, Van der Niepen P, Hoste E, Malbrain ML, Damas P, Devriendt J; SHARF investigators. Intermittent versus continuous renal replacement therapy for acute kidney injury patients admitted to the intensive care unit: results of a randomized clinical trial. Nephrol Dial Transplant. 2009;24(2):512–8. Epub 2008 Oct 14.
Pryor HI 2nd, Vacanti JP. The promise of artificial liver replacement. Front Biosci. 2008;13:2140–59. Review.
Sechser A, Osorio J, Freise C, Osorio RW. Artificial liver support devices for fulminant liver failure. Clin Liver Dis. 2001;5(2):415–30. Review.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Siracuse, J.J., Saillant, N.N. & Hauser, C.J. Technological advancements in the care of the trauma patient. Eur J Trauma Emerg Surg 38, 241–251 (2012). https://doi.org/10.1007/s00068-011-0160-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-011-0160-z