
Abstract
Introduction
The use of targeted intraoperative radiotherapy (TARGIT-IORT) as a tumour bed boost during breast-conserving surgery (BCS) for breast cancer has been reported since 1998. We present its use in patients undergoing breast conservation following neoadjuvant therapy (NACT).
Method
In this retrospective study involving 116 patients after NACT we compared outcomes of 61 patients who received a tumour bed boost with IORT during lumpectomy versus 55 patients treated in the previous 13 months with external (EBRT) boost. All patients received whole breast radiotherapy. Local recurrence-free survival (LRFS), disease-free survival (DFS), distant disease-free survival (DDFS), breast cancer mortality (BCM), non-breast cancer mortality (NBCM) and overall mortality (OS) were compared.
Results
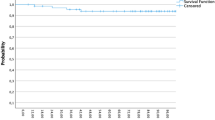
Median follow up was 49 months. The differences in LRFS, DFS and BCM were not statistically significant. The 5‑year Kaplan–Meier estimate of OS was significantly better by 15% with IORT: IORT 2 events (96.7%, 95%CI 87.5–99.2), EBRT 9 events (81.7%, 95%CI 67.6–90.1), hazard ratio (HR) 0.19 (0.04–0.87), log rank p = 0.016, mainly due to a reduction of 10.1% in NBCM: IORT 100%, EBRT 89.9% (77.3–95.7), HR (not calculable), log rank p = 0.015. The DDFS was as follows: IORT 3 events (95.1%, 85.5–98.4), EBRT 12 events (69.0%, 49.1–82.4), HR 0.23 (0.06–0.80), log rank p = 0.012.
Conclusion
IORT during lumpectomy after neoadjuvant chemotherapy as a tumour bed boost appears to give results that are not worse than external beam radiotherapy boost. These data give further support to the inclusion of such patients in the TARGIT-B (boost) randomised trial that is testing whether IORT boost is superior to EBRT boost.
Zusammenfassung
Einleitung
Die intraoperative Radiotherapie (TARGIT-IORT) als vorgezogener Boost im Rahmen der brusterhaltenden Therapie (BET) ist seit 1998 Gegenstand der wissenschaftlichen Diskussion. Wir präsentieren Daten zum Einsatz der IORT bei der BET nach neoadjuvanter Therapie (NACT).
Methode
In diese retrospektive Analyse wurden 116 Patientinnen nach NACT eingeschlossen. Verglichen wurden 61 Patientinnen, die während der Lumbektomie einen Boost als IORT erhalten hatten, mit 55 Patientinnen, die in den vergangenen 13 Monaten mit einem externen Boost (EBRT) behandelt worden waren. Bei allen 116 Patientinnen wurde postoperativ eine Granzbrustbestrahlung durchgeführt. Verglichen wurden lokales rezidivfreies (LRFS), krankheitsfreies (DFS) und fernmetastasenfreies Überleben (DDFS) sowie Brustkrebs- (BCM), nichtbrustkrebsbezogene (NBCM) und Gesamtmortalität (OS).
Ergebnisse
Das mediane Follow-up betrug 49 Monate. Die Unterschiede bezüglich LRFS, DFS und BCM waren statistisch nicht signifikant. Die 5‑Jahres-Kaplan-Meier-Schätzung für das OS ergab einen signifikanten Vorteil von 15 % für die IORT: IORT 2 Ereignisse (96,7 %, 95%-KI 87,5–99,2), EBRT 9 Ereignisse (81,7 %, 95%-KI 67,6–90,1), Hazard Ratio (HR) 0,19 (0,04–0,87), Log Rank p = 0,016, vor allem durch eine Reduktion von 10,1 % bei der NBCM: IORT 100 %, EBRT 89,9 % (77,3–95,7), HR (nicht berechenbar), Log Rank p = 0,015. Des Weiteren zeigte sich eine signifikante Verbesserung beim DDFS: IORT 3 Ereignisse (95,1 %, 85,5–98,4), EBRT 12 Ereignisse (69,0 %, 49,1–82,4), HR 0,23 (0,06–0,80), Log Rank p = 0,012.
Schlussfolgerung
Die IORT im Rahmen der Lumpektomie nach NACT als Tumorbett-Boost ist der EBRT nicht unterlegen. Diese Daten unterstreichen die Wichtigkeit der Rekrutierung in die randomisierte TARGIT-B-(Boost-)Studie, die untersucht, ob der IORT- dem EBRT-Boost überlegen ist.


Similar content being viewed by others


References
Vaidya JS, Wenz F, Bulsara M et al (2014) Risk-adapted targeted intraoperative radiotherapy versus whole-breast radiotherapy for breast cancer: 5‑year results for local control and overall survival from the TARGIT-A randomised trial. Lancet 383(9917):603–613
Krug D (2016) Accelerated partial breast irradiation using interstitial multicatheter brachytherapy: A valid treatment option for breast cancer patients with a low-risk profile? Strahlenther Onkol 192(2):127–129
Vaidya JS, Baum M, Tobias JS et al (2011) Long-term results of targeted intraoperative radiotherapy (Targit) boost during breast-conserving surgery. Int J Radiat Oncol Biol Phys 81(4):1091–1097
Wenz F, Welzel G, Blank E et al (2010) Intraoperative radiotherapy as a boost during breast-conserving surgery using low-kilovoltage X‑rays: the first 5 years of experience with a novel approach. Int J Radiat Oncol Biol Phys 77(5):1309–1314
Fastner G, Hauser-Kronberger C, Moder A et al (2016) Survival and local control rates of triple-negative breast cancer patients treated with boost-IOERT during breast-conserving surgery. Strahlenther Onkol 192(1):1–7
Huober J, von Minckwitz G, Denkert C et al (2010) Effect of neoadjuvant anthracycline-taxane-based chemotherapy in different biological breast cancer phenotypes: overall results from the gepartrio study. Breast Cancer Res Treat 124:133–140
Fastner G, Reitsamer R, Ziegler I et al (2015) IOERT as anticipated tumor bed boost during breast-conserving surgery after neoadjuvant chemotherapy in locally advanced breast cancer – Results of a case series after 5‑year follow-up. Int J Cancer 136:1193–1201
Kolberg HC, Loevey G, Akpolat-Basci L et al (2015) Intraoperative radiotherapy as a boost after neoadjuvant chemotherapy: DFS after a median follow-up of 4 years. J Clin Oncol 33(Suppl):abstr e12050
Sperk E, Welzel G, Keller A et al (2012) Late radiation toxicity after intraoperative radiotherapy (IORT) for breast cancer: results from the randomized phase III trial TARGIT A. Breast Cancer Res Treat 135(1):253–260
Kolberg HC, Stephanou M, Akpolat-Basci L et al (2013) Intraoperative Radiotherapie mit dem Intrabeam® als vorgezogener Boost bei der brusterhaltenden Therapie des Mammakarzinoms – Erfahrungen nach den ersten 200 Fällen. Senologie 10:A73. doi:10.1055/s-0033-1347608
Kolberg HC, Stephanou M, Akpolat-Basci L et al (2014) Intraoperative Radiotherapie mit dem Intrabeam® als vorgezogener Boost nach neoadjuvanter Chemotherapie des Mammakarzinoms – Erfahrungen nach den ersten 130 Fällen. Senologie 11:A67
Loibl S, Volz C, Mau C et al (2014) Response and prognosis after neoadjuvant chemotherapy in 1,051 patients with infiltrating lobular breast carcinoma. Breast Cancer Res Treat 144:153–162
Krug D, Lederer B, Debus J (2015) Relationship of omission of adjuvant radiotherapy to outcomes of locoregional control and disease-free survival in patients with or without pCR after neoadjuvant chemotherapy for breast cancer: a meta-analysis on 3481 patients from the Gepar-trials. J Clin Oncol 33(Suppl):abstr 1008
Dent R, Hanna WM, Trudeau M et al (2009) Time to disease recurrence in basal-type breast cancers: effects of tumor size and lymph node status. Cancer 115(21):4917–4923
Vaidya JS, Bulsara M, Wenz F et al (2013) The lower non-breast cancer mortality with TARGIT in the TARGIT-A trial could be a systemic effect of TARGIT on tumor microenvironment. Int J Radiat Oncol Biol Phys 87(2):S240
Belletti B, Vaidya JS, D’Andrea S et al (2008) Targeted intraoperative radiotherapy impairs the stimulation of breast cancer cell proliferation and invasion caused by surgical wounding. Clin Cancer Res 14(5):1325–1332
Vaidya JS, Bulsara M, Wenz F (2013) Ischemic heart disease after breast cancer radiotherapy. New Engl J Med 368(26):2526
Sta Maria NS, Barnes SR, Weist MR et al (2015) Low dose focused ultrasound induces enhanced tumor accumulation of natural killer cells. PLOS ONE 10(11):e0142767
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
L. Akpolat-Basci, M. Stephanou, and M. Untch state that they have no competing interests. H.-C. Kolberg reports personal fees from Carl Zeiss meditec, TEVA, Theraclion, Novartis, Amgen, Janssen, GSK, LIV Pharma, and Genomic Health outside the submitted work. G. Loevey reports personal fees from Carl Zeiss meditec outside the submitted work. P.A. Fasching reports personal fees from Roche, TEVA, Pfizer, and Genomic Health and grants and personal fees from Novartis and from Amgen outside the submitted work. C. Liedtke reports personal fees from Celgene, TEVA, Pierre Fabre, Novartis, Amgen, Eisai, GSK, Roche, and Genomic Health outside the submitted work. M. Bulsara reports grants and personal fees from Carl Zeiss meditec outside the submitted work. J.S. Vaidya reports grants from Photoelectron corporation 1996–1999, personal fees from Carl Zeiss, non-financial support and other from Carl Zeiss, during the conduct of the study; personal fees from Carl Zeiss meditec, non-financial support and other from Carl Zeiss meditec outside the submitted work.
Ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Kolberg, H., Loevey, G., Akpolat-Basci, L. et al. Targeted intraoperative radiotherapy tumour bed boost during breast-conserving surgery after neoadjuvant chemotherapy. Strahlenther Onkol 193, 62–69 (2017). https://doi.org/10.1007/s00066-016-1072-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-016-1072-y