
Abstract
Aim
The purpose of this work was to retrospectively evaluate survival and local control rates of triple-negative breast cancer subtypes classified as five marker negative (5NP) and core basal (CB), respectively, after breast-conserving surgery and intraoperative boost radiotherapy with electrons (IOERT) followed by whole breast irradiation.
Methods and materials
A total of 71 patients with triple-negative breast cancer were enrolled, who were treated with lumpectomy, axillary lymph node dissection, and IOERT with 9.6 Gy (median Dmax) followed by normofractionated whole breast irradiation to median total doses of 54 Gy. Chemotherapy was applied in a neoadjuvant (12 %), adjuvant (75 %), or combinational setting (7 %).
Results
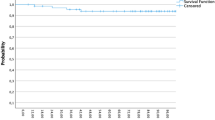
After a median follow-up of 97 months (range 4–170 months), 5 in-breast recurrences were detected (7.0 %). For all patients, 8-year actuarial rates for local control, metastases-free survival, disease-specific survival, and overall survival amounted to 89, 75, 80, and 69 %, respectively. All local recurrences occurred in grade 3 (G3) tumors irrespective of their specific immunohistochemical phenotype; thus, the local control rate for grades 1/2 (G1/2) was 100 % for both 5NP and CB, while for G3 it was 88 % for 5NP and 90 % for CB (p = 0.65 and 0.82, respectively, n.s.). For disease-specific survival, only the difference of the best-prognosis group 5-NP/G3 vs. the worst-prognosis cohort CB/G1/2 was statistically significant: 90 % vs. 54 % (p = 0.03).
Conclusion
Boost-IOERT provides acceptable long-term in-breast control in triple negative breast cancer. The best subgroup in terms of disease-specific survival was represented by 5NP in combination with tumor grading G3.
Zusammenfassung
Hintergrund
Ziel der Studie war es, im Rahmen einer retrospektiven Analyse Überlebens- und Lokalkontrollraten bei triple-negativen Mammakarzinomen zu untersuchen. Die Tumoren waren in 5NP(5-Marker-negative)- und CB(core basal)-Subtypen klassifiziert und die Patientinnen hatten nach brusterhaltender Operation und intraoperativem Elektronenboost (IOERT) eine Ganzbrustbestrahlung erhalten.
Material und Methoden
Insgesamt 71 Patientinnen mit triple-negativem Mammakarzinom erhielten während einer Lumpektomie und axillärer Lymphknotendissektion eine IOERT (med Dmax 9,6 Gy ) und danach eine Ganzbrustbestrahlung in konventioneller Fraktionierung (mediane Gesamtdosis 54 Gy). Eine Chemotherapie wurde in neoadjuvanter (12 %), adjuvanter (75 %) oder kombinierter (7 %) Sequenz durchgeführt.
Ergebnisse
Nach einer medianen Follow-up-Phase von 97 Monaten (Bereich 4–170) wurden 5 ipsilaterale In-Brust-Rezidive festgestellt (7%). Die aktuarischen Achtjahresraten aller Patientinnen für lokale Kontrolle bzw. metastasenfreies, krankheitsspezifisches und Gesamtüberleben lagen entsprechend bei 89, 75, 80 und 69 %. Unabhängig vom immunhistochemischen Phänotyp traten alle Lokalrezidive bei Tumoren mit niedrigem Differenzierungsgrad G3 auf [Lokalkontrollen: G1/2 (CB und 5NP) 100 % vs. G3 88 % (5NP) und 90 % (CB), p = 0,65 bzw. 0,82; n.s.]. Bezüglich des krankheitsspezifischen Überlebens zeigte der Vergleich zwischen der Subgruppe mit der besten Prognose 5NP/G3 und der mit der schlechtesten Prognose CB/G1/2 statistische Signifikanz: 90 vs. 54 % (p = 0,03).
Zusammenfassung
Bei konservativ operierten triple-negativen Mammakarzinomen erzielt die IOERT als Boostmodalität vor einer Ganzbrustbestrahlung auch langfristig akzeptable Lokalkontrollraten. Die Kombination eines 5NP-Subtyps mit dem Tumordifferenzierungsgrad G3 zeigt einen signifikanten Vorteil im krankheitsspezifischen Überleben.

Similar content being viewed by others


Notes
In-breast and regional recurrences together
References
Goldhirsch A, Winer EP, Coates AS et al (2013) Personalizing the treatment of women with early breast cancer: highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann Oncol 24:2206–2223
Lowery AJ, Kell MR, Glynn RW et al (2012) Locoregional recurrence after breast cancer surgery: a systematic review by receptor phenotype. Breast Cancer Res Treat 133:831–841
Lehmann BD, Bauer JA, Chen X et al (2011) Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J Clin Invest 121:2750–2767
Perou CM (2010) Molecular stratification of triple-negative breast cancers. Oncologist 15:39–48
Peddi PF, Ellis MJ, Ma C (2012) Molecular basis of triple negative breast cancer and implications for therapy. Int J Breast Cancer 2012:217185. doi:10.1155/2012/217185
Cheang MC, Voduc D, Bajdik C et al (2008) Basal-like breast cancer defined by five biomarkers has superior prognostic value than triple-negative phenotype. Clin Cancer Res 14:1368–1376
Cho EY, Chang MH, Choi YL et al (2011) Potential candidate biomarkers for heterogeneity in triple-negative breast cancer (TNBC). Cancer Chemother Pharmacol 68:753–761
Uhm JE, Park YH, Yi SY et al (2009) Treatment outcomes and clinicopathologic characteristics of triple-negative breast cancer patients who received platinum-containing chemotherapy. Int J Cancer 124:1457–1462
Sedlmayer F, Sautter-Bihl ML, Budach W et al (2013) DEGRO practical guidelines: radiotherapy of breast cancer I: radiotherapy following breast conserving therapy for invasive breast cancer. Strahlenther Onkol 189:825–833
Bartelink H, Maingon P, Poortmans P et al (2015) Whole-breast irradiation with or without a boost for patients treated with breast-conserving surgery for early breast cancer: 20-year follow-up of a randomised phase 3 trial. Lancet Oncol 16:47–56
Reitsamer R, Sedlmayer F, Kopp M et al (2006) The Salzburg concept of intraoperative radiotherapy for breast cancer: results and considerations. Int J Cancer 118:2882–2887
Sedlmayer F, Fastner G, Merz F et al (2007) IORT with electrons as boost strategy during breast conserving therapy in limited stage breast cancer: results of an ISIORT pooled analysis. Strahlenther Onkol 183:32–34
Krengli M, Calvo FA, Sedlmayer F et al (2013) Clinical and technical characteristics of intraoperative radiotherapy. Analysis of the ISIORT-Europe database. Strahlenther Onkol 189:729–737
Fastner G, Sedlmayer F, Merz F et al (2013) IORT with electrons as boost strategy during breast conserving therapy in limited stage breast cancer: long term results of an ISIORT pooled analysis. Radiother Oncol 108:279–286
Kaplan EL, Meier P (1958) Nonparametric-Estimation from Incomplete Observations. J Am Stat Assoc 53:457–481
Voduc KD, Cheang MC, Tyldesley S et al (2010) Breast cancer subtypes and the risk of local and regional relapse. J Clin Oncol 28:1684–1691
Millar EK, Graham PH, O’Toole SA et al (2009) Prediction of local recurrence, distant metastases, and death after breast-conserving therapy in early-stage invasive breast cancer using a five-biomarker panel. J Clin Oncol 27:4701–4708
Elsawaf Z, Sinn HP, Rom J et al (2013) Biological subtypes of triple-negative breast cancer are associated with distinct morphological changes and clinical behaviour. Breast 22:986–992
Luporsi E, Andre F, Spyratos F et al (2012) Ki-67: level of evidence and methodological considerations for its role in the clinical management of breast cancer: analytical and critical review. Breast Cancer Res Treat 132:895–915
Vaidya JS, Baldassarre G, Massarut S (2009) Beneficial effects of intraoperative radiotherapy on tumor microenvironment could improve outcomes (Int J Radiat Oncol Biol Phys 2008;72:1575–1581). Int J Radiat Oncol Biol Phys 74:976
Belletti B, Vaidya JS, D’Andrea S et al (2008) Targeted intraoperative radiotherapy impairs the stimulation of breast cancer cell proliferation and invasion caused by surgical wounding. Clin Cancer Res 14:1325–1332
Herskind C, Griebel J, Kraus-Tiefenbacher U et al (2008) Sphere of equivalence—a novel target volume concept for intraoperative radiotherapy using low-energy X rays. Int J Radiat Oncol Biol Phys 72:1575–1581
Pogoda K, Niwinska A, Murawska M et al (2013) Analysis of pattern, time and risk factors influencing recurrence in triple-negative breast cancer patients. Med Oncol 30:388
Montagna E, Bagnardi V, Rotmensz N et al (2012) Breast cancer subtypes and outcome after local and regional relapse. Ann Oncol 23:324–331
Nguyen PL, Taghian AG, Katz MS et al (2008) Breast cancer subtype approximated by estrogen receptor, progesterone receptor, and HER-2 is associated with local and distant recurrence afte breast-conserving therapy. J Clin Oncol 26:2373–2378
Moran MS (2015) Radiation therapy in the locoregional treatment of triple-negative breast cancer. Lancet Oncol 16:e113–e122
Zaky SS, Lund M, May KA et al (2011) The negative effect of triple-negative breast cancer on outcome after breast-conserving therapy. Ann Surg Oncol 18:2858–2865
Cortazar P, Zhang L, Untch M et al (2014) Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 384:164–172
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
G. Fastner, C. Hauser-Kronberger, A. Moder, R. Reitsamer, F. Zehentmayr, P. Kopp, C. Fussl, T. Fischer, H. Deutschmann, and F. Sedlmayer state that there are no conflicts of interest.
The accompanying manuscript does not include studies on humans or animals.
Rights and permissions
About this article

Cite this article
Fastner, G., Hauser-Kronberger, C., Moder, A. et al. Survival and local control rates of triple-negative breast cancer patients treated with boost-IOERT during breast-conserving surgery. Strahlenther Onkol 192, 1–7 (2016). https://doi.org/10.1007/s00066-015-0895-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-015-0895-2
Keywords
- Triple-negative breast neoplasms
- Intraoperative radiotherapy
- Breast conserving surgery
- Electrons
- Recurrence