
Abstract
Purpose
Changes in metabolism, including high glucose serum levels, seem to influence the initiation of malignancy as well as recurrence. Therefore, limiting the energy supply in tumor cells with the antidiabetic drug metformin might be a useful approach to inhibit glioma cell progression. However, little is known about the effects of endocrine disorders (e.g., diabetes mellitus, corticosteroid therapy, and metformin therapy) on progression and survival in primary glioblastoma patients.
Patients and methods
Between 2006 and 2013, 276 patients with primary glioblastoma underwent radiation therapy at Heidelberg University Hospital and German Cancer Research Center. Clinical records as well as pretherapeutic and follow-up magnetic resonance (MR) images were assessed. Forty patients (14.5 %) were identified with a pretherapeutic history of diabetes, and 20 (50 %) of them were treated with metformin. Survival and correlations were calculated using t-test and log-rank, univariate and multivariate Cox proportional hazards ratio analyses.
Results
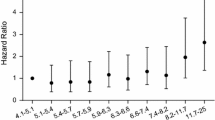
Persistent mild and excessive hyperglycemia were correlated with decreased survival. Corticosteroid therapy was associated with decreased progression-free and overall survival in the multivariate analysis. No negative influence of diabetes on progression and survival could be detected. Interestingly, diabetic patients with metformin therapy demonstrated prolonged progression-free intervals.
Conclusion
Corticosteroid therapy and hyperglycemia were strongly associated with impaired survival rates and serves as negative prognostic factors. Diabetes did not influence survival. Interestingly, our findings showed an association of metformin therapy and prolonged progression-free survival in glioblastoma patients with diabetes and therefore serve as a foundation for further preclinical and clinical investigations.
Zusammenfassung
Ziel
Veränderungen im körperlichen Metabolismus, darunter hohe Serumglukosespiegel, beeinflussen die Entstehung, das Wachstum und die rezidivierenden Eigenschaften maligner Tumore. Die Limitierung der Energieversorgung maligner Zellen mit dem Antidiabetikum Metformin könnte einen vielversprechenden Ansatz darstellen, das Glioblastomwachstum zu hemmen. Jedoch ist bis heute wenig über den Einfluss von endokrinen Dysfunktionen wie Diabetes mellitus, Kortikosteroidtherapie und dem Antidiabetikum Metformin auf die Progression und das Überleben bei Glioblastompatienten bekannt.
Patienten und Methoden
Zwischen 2006 und 2013 erhielten 276 Glioblastompatienten am Universitätsklinikum Heidelberg und am Deutschen Krebsforschungszentrum Heidelberg (DKFZ) eine Radiotherapie. Sowohl die klinischen Dokumente als auch die prä- und posttherapeutischen Magnetresonanztomogramme (MRT) wurden für diese Studie ausgewertet. Es konnten 40 Patienten (14,5 %) mit einer prätherapeutischen Diabetesdiagnose identifiziert werden, von den 20 (50 %) eine antidiabetische Therapie mit Metformin erhielten. Die Überlebensraten und Korrelationen mit klinischen Faktoren wurden mit Hilfe des t-Test, Log-rank-Test und der univariaten und multivariaten Cox-Regression berechnet.
Ergebnisse
Unsere Daten zeigen, dass milde und exzessive persistierende Hyperglykämien und eine Kortikosteroidtherapie in der multivariaten Analyse mit einem verminderten Überleben assoziiert waren. Diabetes selbst hatte keinen Einfluss auf die Progression oder das Überleben. Interessanterweise wiesen Diabetespatienten die eine Metformin-Therapie erhielten, ein signifikant verlängertes progressionfreies Intervall auf.
Schlussfolgerung
Zusammenfassend zeigen unsere Daten einen negativen prognostischen Einfluss der Hyperglykämie und Kortikosteroidtherapie auf das Überleben der Glioblastompatienten. Diabetes zeigte keinen Effekt auf das Überleben. Des Weiteren war eine Metformin-Therapie bei Diabetikern mit einem verlängerten progressionsfreien Intervall vergesellschaftet. Diese Ergebnisse sind von therapeutischem Interesse und dienen als Grundlage für weitere notwendige präklinische und klinische Untersuchungen.

Similar content being viewed by others


References
Louis DN, Ohgaki H, Wiestler OD et al (2007) The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol 114:97–109
Stupp R, Mason WP, van den Bent MJ et al (2005) Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352:987–996
Scott JN, Rewcastle NB, Brasher PM et al (1999) Which glioblastoma multiforme patient will become a long-term survivor? A population-based study. Ann Neurol 46:183–188
Chaichana KL, Pendleton C, Chambless L et al (2013) Multi-institutional validation of a preoperative scoring system which predicts survival for patients with glioblastoma. J Clin Neurosci 20:1422–1426
Adeberg S, Konig L, Bostel T et al (2014) Glioblastoma recurrence patterns after radiation therapy with regard to the subventricular zone. Int J Radiat Oncol Biol Phys 90:886–896
Combs SE, Edler L, Rausch R, Welzel T, Wick W, Debus J (2013) Generation and validation of a prognostic score to predict outcome after re-irradiation of recurrent glioma. Acta Oncol 52:147–152
Adeberg S, Bostel T, Konig L, Welzel T, Debus J, Combs SE (2014) A comparison of long-term survivors and short-term survivors with glioblastoma, subventricular zone involvement: a predictive factor for survival? Radiat Oncol 9:95
Schulz-Ertner D, Tsujii H (2007) Particle radiation therapy using proton and heavier ion beams. J Clin Oncol 25:953–964
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D (2011) Global cancer statistics. CA Cancer J Clin 61:69–90
Polednak AP (2006) Comorbid diabetes mellitus and risk of death after diagnosis of colorectal cancer: a population-based study. Cancer Detect Prev 30:466–472
Weiser MA, Cabanillas ME, Konopleva M et al (2004) Relation between the duration of remission and hyperglycemia during induction chemotherapy for acute lymphocytic leukemia with a hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone/methotrexate-cytarabine regimen. Cancer 100:1179–1185
Yancik R, Wesley MN, Ries LA, Havlik RJ, Edwards BK, Yates JW (2001) Effect of age and comorbidity in postmenopausal breast cancer patients aged 55 years and older. JAMA 285:885–892
Suba Z, Ujpal M (2006) [Correlations of insulin resistance and neoplasms]. Magy Onkol 50:127–135
Suba Z, Barabas J, Szabo G, Takacs D, Ujpal M (2005) Increased prevalence of diabetes and obesity in patients with salivary gland tumors. Diabetes Care 28:228
Nilsen TI, Vatten LJ (2001) Prospective study of colorectal cancer risk and physical activity, diabetes, blood glucose and BMI: exploring the hyperinsulinaemia hypothesis. Br J Cancer 84:417–422
Colangelo LA, Gapstur SM, Gann PH, Dyer AR, Liu K (2002) Colorectal cancer mortality and factors related to the insulin resistance syndrome. Cancer Epidemiol Biomarkers Prev 11:385–391
Krinsley JS (2004) Effect of an intensive glucose management protocol on the mortality of critically ill adult patients. Mayo Clin Proc 79:992–1000
van den Berghe G, Wouters P, Weekers F et al (2001) Intensive insulin therapy in critically ill patients. N Engl J Med 345:1359–1367
Woodworth GF, Chaichana KL, McGirt MJ et al (2007) Predictors of ambulatory function after surgical resection of intramedullary spinal cord tumors. Neurosurgery 61:99–105. (discussion -6)
Welch MR, Grommes C (2013) Retrospective analysis of the effects of steroid therapy and antidiabetic medication on survival in diabetic glioblastoma patients. CNS Oncol 2:237–246
Warburg O (1956) On the origin of cancer cells. Science 123:309–314
Warburg O, Wind F, Negelein E (1927) The metabolism of tumors in the body. J Gen Physiol 8:519–530
Guo D, Cloughesy TF, Radu CG, Mischel PS (2010) AMPK: a metabolic checkpoint that regulates the growth of EGFR activated glioblastomas. Cell Cycle 9:211–212
Jalving M, Gietema JA, Lefrandt JD et al (2010) Metformin: taking away the candy for cancer? Eur J Cancer 46:2369–2380
Jelluma N, Yang X, Stokoe D, Evan GI, Dansen TB, Haas-Kogan DA (2006) Glucose withdrawal induces oxidative stress followed by apoptosis in glioblastoma cells but not in normal human astrocytes. Mol Cancer Res 4:319–330
Sandulache VC, Hamblin JS, Skinner HD, Kubik MW, Myers JN, Zevallos JP (2014) Association between metformin use and improved survival in patients with laryngeal squamous cell carcinoma. Head Neck 36:1039–1043
Skinner HD, Crane CH, Garrett CR et al (2013) Metformin use and improved response to therapy in rectal cancer. Cancer Med 2:99–107
Skinner HD, McCurdy MR, Echeverria AE et al (2013) Metformin use and improved response to therapy in esophageal adenocarcinoma. Acta Oncol 52:1002–1009
Storozhuk Y, Hopmans SN, Sanli T et al (2013) Metformin inhibits growth and enhances radiation response of non-small cell lung cancer (NSCLC) through ATM and AMPK. Br J Cancer 108:2021–2032
Ling S, Feng T, Ke Q et al (2014) Metformin inhibits proliferation and enhances chemosensitivity of intrahepatic cholangiocarcinoma cell lines. Oncol Rep 31:2611–2618
Li H, Chen X, Yu Y et al (2014) Metformin inhibits the growth of nasopharyngeal carcinoma cells and sensitizes the cells to radiation via inhibition of the DNA damage repair pathway. Oncol Rep 32:2596–2604
Mohammed A, Janakiram NB, Brewer M et al (2013) Antidiabetic drug metformin prevents progression of pancreatic cancer by targeting in part cancer stem cells and mTOR signaling. Transl Oncol 6:649–659
Kalender A, Selvaraj A, Kim SY et al (2010) Metformin, independent of AMPK, inhibits mTORC1 in a rag GTPase-dependent manner. Cell Metab 11:390–401
Rozengurt E (2014) Mechanistic target of rapamycin (mTOR): a point of convergence in the action of insulin/IGF-1 and G protein-coupled receptor agonists in pancreatic cancer cells. Front Physiol 5:357
Isakovic A, Harhaji L, Stevanovic D et al (2007) Dual antiglioma action of metformin: cell cycle arrest and mitochondria-dependent apoptosis. Cell Mol Life Sci 64:1290–1302
Scheithauer BW, Fuller GN, VandenBerg SR (2008) The 2007 WHO classification of tumors of the nervous system: controversies in surgical neuropathology. Brain Pathol 18:307–316
Nathan DM, Buse JB, Davidson MB et al (2009) Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 32:193–203
Wen PY, Macdonald DR, Reardon DA et al (2010) Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J Clin Oncol 28:1963–1972
Shrieve DC, Alexander E 3rd, Black PM et al (1999) Treatment of patients with primary glioblastoma multiforme with standard postoperative radiotherapy and radiosurgical boost: prognostic factors and long-term outcome. J Neurosurg 90:72–77
Mirimanoff RO, Gorlia T, Mason W et al (2006) Radiotherapy and temozolomide for newly diagnosed glioblastoma: recursive partitioning analysis of the EORTC 26981/22981-NCIC CE3 phase III randomized trial. J Clin Oncol 24:2563–2569
Mayer A, Vaupel P, Struss HG, Giese A, Stockinger M, Schmidberger H (2014) Strong adverse prognostic impact of hyperglycemic episodes during adjuvant chemoradiotherapy of glioblastoma multiforme. Strahlenther Onkol 19:933–938
McGirt MJ, Chaichana KL, Gathinji M et al (2008) Persistent outpatient hyperglycemia is independently associated with decreased survival after primary resection of malignant brain astrocytomas. Neurosurgery 63:286–291. (discussion 91)
Derr RL, Ye X, Islas MU, Desideri S, Saudek CD, Grossman SA (2009) Association between hyperglycemia and survival in patients with newly diagnosed glioblastoma. J Clin Oncol 27:1082–1086
Adeberg S, Bernhardt D, Foerster R, Bostel T, Koerber SA, Mohr A, Koelsche C, Rieken S, Debus J (2015) The influence of hyperglycemia during radiotherapy on survival in patients with primary glioblastoma. Acta Oncol 20:1-7
Oudard S, Arvelo F, Miccoli L et al (1996) High glycolysis in gliomas despite low hexokinase transcription and activity correlated to chromosome 10 loss. Br J Cancer 74:839–845
Kwon T, Jeong IG, You D et al (2014) Obesity and prognosis in muscle-invasive bladder cancer: the continuing controversy. Int J Urol 21:1106–1112
Siegel EM, Ulrich CM, Poole EM, Holmes RS, Jacobsen PB, Shibata D (2010) The effects of obesity and obesity-related conditions on colorectal cancer prognosis. Cancer Control 17:52–57
Daniell HW (2010) Smoking, obesity, and statin therapy in the prognosis of prostate cancer. J Clin Oncol 28:e643. (author reply e5–6)
Sinicrope FA, Dannenberg AJ (2011) Obesity and breast cancer prognosis: weight of the evidence. J Clin Oncol 29:4–7
Del Barco S, Vazquez-Martin A, Cufi S et al (2011) Metformin: multi-faceted protection against cancer. Oncotarget 2:896–917
Giannarelli R, Aragona M, Coppelli A, Del Prato S (2003) Reducing insulin resistance with metformin: the evidence today. Diabetes Metab 29:6S28–6S35
Sato A, Sunayama J, Okada M, et al (2012) Glioma-initiating cell elimination by metformin activation of FOXO3 via AMPK. Stem cells Transl Med 1:811–824
Soritau O, Tomuleasa C, Aldea M et al (2011) Metformin plus temozolomide-based chemotherapy as adjuvant treatment for WHO grade III and IV malignant gliomas. J BUON 16:282–289
Ferla R, Haspinger E, Surmacz E (2012) Metformin inhibits leptin-induced growth and migration of glioblastoma cells. Oncol Lett 4:1077–1081
Dietrich J, Rao K, Pastorino S, Kesari S (2011) Corticosteroids in brain cancer patients: benefits and pitfalls. Expert Rev Clin Pharmacol 4:233–242
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
S. Adeberg, D. Bernhardt, S.B. Harrabi, T. Bostel, A. Mohr, C. Koelsche, C. Diehl, S. Rieken, and J. Debus state that there are no conflicts of interest.
All studies on humans described in the present manuscript were carried out with the approval of the responsible ethics committee and in accordance with national law and the Helsinki Declaration of 1975 (in its current, revised form). Informed consent was obtained from all patients included in studies.
Additional information
Presented in part at the 3rd ESTRO Forum, 24–28 April 2015, Barcelona, Spain
Rights and permissions
About this article

Cite this article
Adeberg, S., Bernhardt, D., Harrabi, S. et al. Metformin influences progression in diabetic glioblastoma patients. Strahlenther Onkol 191, 928–935 (2015). https://doi.org/10.1007/s00066-015-0884-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-015-0884-5