
Abstract
Background
Prescription of third-generation cephalosporins and fluoroquinolones has been linked to an increasing incidence of gram-negative bacteria producing extended-spectrum beta-lactamases, methicillin-resistant Staphylococcus aureus and nosocomial infection with Clostridium difficile. Antibiotic stewardship (ABS) programmes offer evidence-based tools to control antibiotic prescription rates and thereby influence the incidence of nosocomial infection and contain the development of multidrug-resistant bacteria, but there is limited experience with such programmes at community hospitals.
Methods
We implemented an ABS programme at a 200-bed community hospital and aimed at a > 30 % reduction of cephalosporin and fluoroquinolone consumption within 1 year. Pharmacy data were obtained to estimate hospital-wide drug use density expressed in WHO-ATC-defined daily doses (DDD) or hospital-adapted recommended daily doses (RDD) per 1,000 patient days. The effect of the ABS intervention on drug use density was analysed using interrupted time-series analysis for the periods between January 2011 and March 2013 as pre-intervention, and between April 2013 and March 2014 as post-intervention period. The CDI incidence was calculated based on microbiology laboratory data.
Results
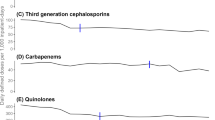
Cephalosporin use (measured in RDD/1,000 patient days) decreased by 33 %, and fluoroquinolone use decreased by 31 %, respectively. Interrupted time-series analysis confirmed significant changes in the drug use density trends for both cephalosporins and fluoroquinolones after the intervention as well as for total antibiotic use that decreased by 11 % while no significant effect was noted for CDI incidence rates.
Conclusion
ABS programmes can be effective in community hospitals and may help establish ecologically advantageous antibiotic strategies when needed.

Similar content being viewed by others


References
Dancer SJ, Kirkpatrick P, Corcoran DS, Christison F, Farmer D, Robertson C. Approaching zero: temporal effects of a restrictive antibiotic policy on hospital-acquired Clostridium difficile, extended-spectrum β-lactamase-producing coliforms and meticillin-resistant Staphylococcus aureus. Int J Antimicrob Agents. 2013;41:137–42.
Livermore DM, Hope R, Reynolds R, Blackburn R, Johnson AP, Woodford N. Declining cephalosporin and fluoroquinolone non-susceptibility among bloodstream Enterobacteriaceae from the UK: links to prescribing change?. Chemother: J. Antimicrob; 2013.
Aldeyab MA, Harbarth S, Vernaz N, Kearney MP, Scott MG, Darwish Elhajji FW et al. The impact of antibiotic use on the incidence and resistance pattern of extended-spectrum beta-lactamase-producing bacteria in primary and secondary healthcare settings. Br. J. Clin. Pharmacol. 2012;74:171–9.
Petrikkos G, Markogiannakis A, Papaparaskevas J, Papapareskevas J, Daikos GL, Stefanakos G, et al. Differences in the changes in resistance patterns to third- and fourth-generation cephalosporins and piperacillin/tazobactam among Klebsiella pneumoniae and Escherichia coli clinical isolates following a restriction policy in a Greek tertiary care hospita. Agents: Int. J. Antimicrob; 2007.
LeBlanc L, Pépin J, Toulouse K, Ouellette M-F, Coulombe M-A, Corriveau M-P, et al. Fluoroquinolones and risk for methicillin-resistant Staphylococcus aureus. Canada. Emerg. Infect. Dis. 2006;12:1398–405.
Kaier K, Hagist C, Frank U, Conrad A, Meyer E. Two time-series analyses of the impact of antibiotic consumption and alcohol-based hand disinfection on the incidences of nosocomial methicillin-resistant Staphylococcus aureus infection and Clostridium difficile infection. Epidemiol: Infect. Control Hosp; 2009.
Pépin J, Saheb N, Coulombe M-A, Alary M-E, Corriveau M-P, Authier S et al. Emergence of fluoroquinolones as the predominant risk factor for Clostridium difficile-associated diarrhea: a cohort study during an epidemic in Quebec. Clin. Infect. Dis. [Internet]. 2005;41:1254–60.
Talpaert MJ. Gopal Rao G, Cooper BS, Wade P. Impact of guidelines and enhanced antibiotic stewardship on reducing broad-spectrum antibiotic usage and its effect on incidence of Clostridium difficile infection. J Antimicrob Chemother. 2011;66:2168–74.
Meyer E, Schwab F, Schroeren-Boersch B, Gastmeier P. Dramatic increase of third-generation cephalosporin-resistant E. coli in German intensive care units: secular trends in antibiotic drug use and bacterial resistance 2001 to 2008. Crit Care. 2010;14:R113.
Mondain V, Lieutier F, Hasseine L, Gari-Toussaint M, Poiree M, Lions C, et al. A 6-year antifungal stewardship programme in a teaching hospital. Infection. 2013;41:621–8.
Dellit TH, Owens RC, McGowan JE, Gerding DN, Weinstein R a, Burke JP et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin. Infect. Dis. 2007;44:159–77.
Davey P, Brown E, Charani E, Fenelon L, Gould IM, Holmes A et al. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane database Syst. Rev. 2013 4:CD003543.
Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27–72.
Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG, McDonald LC, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the infectious diseases society of America (IDSA). Infect Control Hosp Epidemiol. 2010;31:431–55.
Borde JP, Batin N, Rieg S, Feik R, Reimling C, Kern WV et al. Adherence to an antibiotic stewardship bundle targeting Staphylococcus aureus blood stream infections at a 200-bed community hospital. Infection 2014.
Schmitt S, McQuillen DP, Nahass R, Martinelli L, Rubin M, Schwebke K, et al. Infectious diseases specialty intervention is associated with decreased mortality and lower healthcare costs. Dis: Clin. Infect; 2014.
Borde JP, Kaier K, Steib-Bauert M, Vach W, Geibel-Zehender A, Busch H, et al. Feasibility and impact of an intensified antibiotic stewardship programme targeting cephalosporin and fluoroquinolone use in a tertiary care university medical center. BMC Infect Dis. 2014;14:201.
Feazel LM, Malhotra A, Perencevich EN, Kaboli P, Diekema DJ, Schweizer ML. Effect of antibiotic stewardship programmes on Clostridium difficile incidence: a systematic review and meta-analysis. Chemother: J. Antimicrob; 2014.
S3-Leitlinie Strategien zur Sicherung rationaler Antibiotika-Anwendung im Krankenhaus AWMF-Registernummer 092/001, 2013.
http://www.antiinfektiva-surveillance.de/32-0-Allgemeine-Informationen.html.
Conflict of interest
On behalf of all the authors, the corresponding author states that there is no conflict of interest.
Ethical statement
The ethics committee was notified about the trial––formal approval was not required, because the project is based on epidemiological data. Research involving human subjects, human material, specific human or personalised data was not carried out.
Author information
Authors and Affiliations
Corresponding author
Additional information
K. Kaier and W. V. Kern have equally contributed.
Rights and permissions
About this article

Cite this article
Borde, J.P., Litterst, S., Ruhnke, M. et al. Implementing an intensified antibiotic stewardship programme targeting cephalosporin and fluoroquinolone use in a 200-bed community hospital in Germany. Infection 43, 45–50 (2015). https://doi.org/10.1007/s15010-014-0693-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-014-0693-2