
ABSTRACT
BACKGROUND
Young adults with hypertension have the lowest prevalence of controlled blood pressure compared to middle-aged and older adults. Uncontrolled hypertension, even among young adults, increases future cardiovascular event risk. However, antihypertensive medication initiation is poorly understood among young adults and may be an important intervention point for this group.
OBJECTIVE
The purpose of this study was to compare rates and predictors of antihypertensive medication initiation between young adults and middle-aged and older adults with incident hypertension and regular primary care contact.
DESIGN
A retrospective analysis
PARTICIPANTS
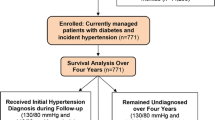
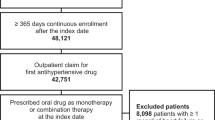
Adults ≥ 18 years old (n = 10,022) with incident hypertension and no prior antihypertensive prescription, who received primary care at a large, Midwestern, academic practice from 2008–2011.
MAIN MEASURES
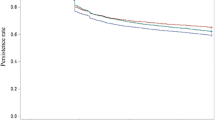
The primary outcome was time from date of meeting hypertension criteria to antihypertensive medication initiation, or blood pressure normalization without medication. Kaplan-Meier analysis was used to estimate the probability of antihypertensive medication initiation over time. Cox proportional-hazard models (HR; 95 % CI) were fit to identify predictors of delays in medication initiation, with a subsequent subpopulation analysis for young adults (18–39 years old).
KEY RESULTS
After a mean follow-up of 20 (±13) months, 34 % of 18–39 year-olds with hypertension met the endpoint, compared to 44 % of 40–59 year-olds and 56 % of ≥ 60 year-olds. Adjusting for patient and provider factors, 18–39 year-olds had a 44 % slower rate of medication initiation (HR 0.56; 0.47–0.67) than ≥ 60 year-olds. Among young adults, males, patients with mild hypertension, and White patients had a slower rate of medication initiation. Young adults with Medicaid and more clinic visits had faster rates.
CONCLUSIONS
Even with regular primary care contact and continued elevated blood pressure, young adults had slower rates of antihypertensive medication initiation than middle-aged and older adults. Interventions are needed to address multifactorial barriers contributing to poor hypertension control among young adults.


Similar content being viewed by others
REFERENCES
Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988–2008. JAMA. 2010;303:2043–50.
Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation. 2013;127:e6–245.
Centers for Disease Control and Prevention. Vital signs: prevalence, treatment, and control of hypertension—United States, 1999–2002 and 2005–2008. MMWR Morb Mortal Wkly Rep. 2011;60:103–8.
Campbell NR, So L, Amankwah E, Quan H, Maxwell C. Characteristics of hypertensive Canadians not receiving drug therapy. Can J Cardiol. 2008;24:485–90.
McCarron P, Smith GD, Okasha M, McEwen J. Blood pressure in young adulthood and mortality from cardiovascular disease. Lancet. 2000;355:1430–1.
Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560–72.
Bailey KR, Grossardt BR, Graves JW. Novel use of Kaplan-Meier methods to explain age and gender differences in hypertension control rates. Hypertension. 2008;51:841–7.
Hong SH, Wang J, Tak S. A patient-centric goal in time to blood pressure control from drug therapy initiation. Clin Transl Sci. 2013;6:7–12.
Ogedegbe G. Barriers to optimal hypertension control. J Clin Hypertens (Greenwich). 2008;10:644–6.
Khanna RR, Victor RG, Bibbins-Domingo K, Shapiro MF, Pletcher MJ. Missed opportunities for treatment of uncontrolled hypertension at physician office visits in the United States, 2005 through 2009. Arch Intern Med. 2012;172:1344–5.
Nguyen QC, Waddell EN, Thomas JC, Huston SL, Kerker BD, Gwynn RC. Awareness, treatment, and control of hypertension and hypercholesterolemia among insured residents of New York City, 2004. Prev Chronic Dis. 2011;8:A109.
Hyman DJ, Pavlik VN. Self-reported hypertension treatment practices among primary care physicians: blood pressure thresholds, drug choices, and the role of guidelines and evidence-based medicine. Arch Intern Med. 2000;160:2281–6.
Hill MN, Bone LR, Kim MT, Miller DJ, Dennison CR, Levine DM. Barriers to hypertension care and control in young urban black men. Am J Hypertens. 1999;12:951–8.
Huebschmann AG, Mizrahi T, Soenksen A, Beaty BL, Denberg TD. Reducing clinical inertia in hypertension treatment: a pragmatic randomized controlled trial. J Clin Hypertens (Greenwich). 2012;14:322–9.
Hatahet MA, Bowhan J, Clough EA. Wisconsin Collaborative for Healthcare Quality (WCHQ): lessons learned. WMJ. 2004;103:45–8.
Sheehy A, Pandhi N, Coursin DB, et al. Minority status and diabetes screening in an ambulatory population. Diabetes Care. 2011;34:1289–94.
WCHQ. Wisconsin Collaborative for Health Care Quality. Available at: http://www.wchq.org/. Accessed January 15, 2014.
Thorpe CT, Flood GE, Kraft SA, Everett CM, Smith MA. Effect of patient selection method on provider group performance estimates. Med Care. 2011;49:780–5.
Myers MG, Tobe SW, McKay DW, Bolli P, Hemmelgarn BR, McAlister FA. New algorithm for the diagnosis of hypertension. Am J Hypertens. 2005;18:1369–74.
Schmittdiel J, Selby JV, Swain B, et al. Missed opportunities in cardiovascular disease prevention?: low rates of hypertension recognition for women at medicine and obstetrics-gynecology clinics. Hypertension. 2011;57:717–22.
Tu K, Campbell NR, Chen ZL, Cauch-Dudek KJ, McAlister FA. Accuracy of administrative databases in identifying patients with hypertension. Open Med. 2007;1:e18–26.
Manson JM, McFarland B, Weiss S. Use of an automated database to evaluate markers for early detection of pregnancy. Am J Epidemiol. 2001;154:180–7.
O'Connor PJ, Sperl-Hillen JM, Johnson PE, Rush WA, Blitz G. Clinical Inertia and Outpatient Medical Errors. In: Henriksen K, Battles JB, Marks ES, Lewin DI, eds. Advances in Patient Safety: From Research to Implementation (Volume 2: Concepts and Methodology). Rockville, MD: Agency of Healthcare Research and Quality (US); 2005:293–308.
Borzecki AM, Wong AT, Hickey EC, Ash AS, Berlowitz DR. Identifying hypertension-related comorbidities from administrative data: what's the optimal approach? Am J Med Qual. 2004;19:201–6.
Hebert PL, Geiss LS, Tierney EF, Engelgau MM, Yawn BP, McBean AM. Identifying persons with diabetes using Medicare claims data. Am J Med Qual. 1999;14:270–7.
Marciniak MD, Lage MJ, Dunayevich E, et al. The cost of treating anxiety: the medical and demographic correlates that impact total medical costs. Depress Anxiety. 2005;21:178–84.
Chronic Conditions Data Warehouse. 2011 Chronic Condition Reference List. Available at: http://www.ccwdata.org/cs/groups/public/documents/document/ccw_conditionreferencelist2011.pdf. Accessed January 15, 2014.
Newton KM, Wagner EH, Ramsey SD, et al. The use of automated data to identify complications and comorbidities of diabetes: a validation study. J Clin Epidemiol. 1999;52:199–207.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27.
Foley RN, Murray AM, Li S, et al. Chronic kidney disease and the risk for cardiovascular disease, renal replacement, and death in the United States Medicare population, 1998 to 1999. J Am Soc Nephrol. 2005;16:489–95.
Starfield B, Weiner J, Mumford L, Steinwachs D. Ambulatory care groups: a categorization of diagnoses for research and management. Health Serv Res. 1991;26:53–74.
StataCorp. STATA Survival Analysis and Epidemiological Tables Reference Manual: Release 12. Statistical Software. College Station, TX: StataCorp LP; 2011.
Mickey RM, Greenland S. The impact of confounder selection criteria on effect estimation. Am J Epidemiol. 1989;129:125–37.
Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika. 1994;81:515–26.
Diao D, Wright JM, Cundiff DK, Gueyffier F. Pharmacotherapy for mild hypertension. Cochrane Database Syst Rev. 2012;8:CD006742.
Saydah S, Bullard KM, Imperatore G, Geiss L, Gregg EW. Cardiometabolic risk factors among US adolescents and young adults and risk of early mortality. Pediatrics. 2013;131:e679–86.
Jolles EP, Clark AM, Braam B. Getting the message across: opportunities and obstacles in effective communication in hypertension care. J Hypertens. 2012;30:1500–10.
de Burgos-Lunar C, Del Cura-Gonzalez I, Salinero-Fort MA, Gomez-Campelo P, Perez de Isla L, Jimenez-Garcia R. Delayed diagnosis of hypertension in diabetic patients monitored in primary care. Rev Esp Cardiol. 2013;66:700–6.
Degli Esposti E, Di Martino M, Sturani A, et al. Risk factors for uncontrolled hypertension in Italy. J Hum Hypertens. 2004;18:207–13.
Piette JD, Kerr EA. The impact of comorbid chronic conditions on diabetes care. Diabetes Care. 2006;29:725–31.
American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care. 2013;36(Suppl 1):S11–66.
Spatz ES, Ross JS, Desai MM, Canavan ME, Krumholz HM. Beyond insurance coverage: usual source of care in the treatment of hypertension and hypercholesterolemia. Data from the 2003–2006 National Health and Nutrition Examination Survey. Am Heart J. 2010;160:115–21.
Brummett BH, Babyak MA, Siegler IC, et al. Systolic blood pressure, socioeconomic status, and biobehavioral risk factors in a nationally representative US young adult sample. Hypertension. 2011;58:161–6.
Acknowledgements
Contributors
The authors gratefully acknowledge Katie Ronk, BS, for data preparation, and Jamie LaMantia, BS, and Colleen Brown, BA, for manuscript preparation.
Funders
Research reported in this manuscript was supported by the Clinical and Translational Science Award (CTSA) program, previously through the National Center for Research Resources (NCRR) under award number UL1RR025011, and now by the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health under award number U54TR000021. Heather Johnson is supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award number K23HL112907, and also by the University of Wisconsin Centennial Scholars Program of the University of Wisconsin School of Medicine and Public Health. Christie Bartels is supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under award number K23AR062381. Nancy Pandhi is supported by the National Institute on Aging of the National Institutes of Health under award number K08AG029527. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Additional funding for this project was provided by the University of Wisconsin Health Innovation Program and the University of Wisconsin School of Medicine and Public Health from The Wisconsin Partnership Program.
Prior Presentations
Some of the findings reported in the manuscript were presented in abstract form at the 2013 American Heart Association Quality of Care and Outcomes Research Scientific Sessions on 16 May 2013.
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(PDF 63 kb)
Rights and permissions
About this article
Cite this article
Johnson, H.M., Thorpe, C.T., Bartels, C.M. et al. Antihypertensive Medication Initiation Among Young Adults with Regular Primary Care Use. J GEN INTERN MED 29, 723–731 (2014). https://doi.org/10.1007/s11606-014-2790-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-014-2790-4