
Abstract
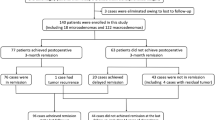
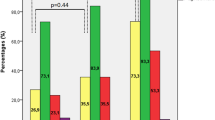
We report the outcomes of the endoscopic endonasal approach (EEA) for resection of growth hormone secreting pituitary adenomas using 2010 consensus criteria. We also assess outcomes with additional medical therapy and radiosurgery (RS) for patients not achieving remission with EEA alone. A retrospective review of 53 patients who had follow up endocrinologic data at least 3 months post-surgery was performed among patients who were treated by EEA between 1998 and 2012. Data were analyzed for remission using GH and IGF-I levels based on 2010 consensus criteria. We also analyzed the outcomes using 2000 consensus criteria for ease in comparison to prior studies of outcomes of surgery for acromegaly. In this series of mostly large (88.2 % macroadenomas), invasive (46.9 % Hardy–Wilson C, D, E) adenomas, there were 27 patients (50.9 %) who achieved remission after EEA only. For patients who had no remission with EEA alone, RS and/or medical therapy were used and 37 patients (69.8 %) achieved remission overall. Statistical analysis showed larger tumor size, Hardy Stages C, D, E and Knosp Scores 3, 4 to be predictive against remission for EEA only and EEA with other modalities. The volume of residual tumor after EEA was not found to be predictive of remission with additional therapies. We used stringent consensus criteria from 2010 in a series which included a high proportion of invasive GH secreting adenomas to show that EEA alone or combined with other modalities results in comparable remission rates to earlier studies which used less strict criteria, while retaining low complication rates.

Similar content being viewed by others
Abbreviations
- EEA:
-
Endoscopic endonasal approach
- RS:
-
Radiosurgery
- GH:
-
Growth hormone
- IGF-I:
-
Insulin growth factor-I
- GHRH:
-
Growth hormone releasing hormone
- CSF:
-
Cerebrospinal fluid
- ICA:
-
Internal carotid artery
- DI:
-
Diabetes insipidus
- CN:
-
Cranial nerve
References
Dekkers OM, Biermasz NR, Pereira AM, Romijn JA, Vandenbroucke JP (2008) Mortality in acromegaly: a metaanalysis. J Clin Endocrinol Metab 93:61–67
Chanson P, Salenave S, Kamenicky P, Cazabat L, Young J (2009) Pituitary tumours: acromegaly. Best Pract Res Clin Endocrinol Metab 23:555–574
Donangelo I, Melmed S (2005) Treatment of acromegaly: future. Endocrine 28:123–128
Melmed S, Colao A, Barkan A, Molitch M, Grossman AB, Kleinberg D, Clemmons D, Chanson P, Laws E, Schlechte J, Vance ML, Ho K, Giustina A, Acromegaly Consensus Group (2009) Guidelines for acromegaly management: an update. J Clin Endocrinol Metab 94:1509–1517
Ahmed S, Elsheikh M, Stratton IM, Page RC, Adams CB, Wass JA (1999) Outcome of transsphenoidal surgery for acromegaly and its relationship to surgical experience. Clin Endocrinol (Oxf) 50:561–567
Freda PU, Wardlaw SL, Post KD (1998) Long-term endocrinological follow-up evaluation in 115 patients who underwent transsphenoidal surgery for acromegaly. J Neurosurg 89:353–358
Campbell PG, Kenning E, Andrews DW, Yadla S, Rosen M, Evans JJ (2010) Outcomes after a purely endoscopic transsphenoidal resection of growth hormone-secreting pituitary adenomas. Neurosurg Focus 29:E5
Sherlock M, Woods C, Sheppard MC (2011) Medical therapy in acromegaly. Nat Rev Endocrinol 7:291–300
Castinetti F, Régis J, Dufour H, Brue T (2010) Role of stereotactic radiosurgery in the management of pituitary adenomas. Nat Rev Endocrinol 6:214–223
Abosch A, Tyrrell JB, Lamborn KR, Hannegan LT, Applebury CB, Wilson CB (1998) Transsphenoidal microsurgery for growth hormone-secreting pituitary adenomas: initial outcome and long-term results. J Clin Endocrinol Metab 83:3411–3418
Ross DA, Wilson CB (1988) Results of transsphenoidal microsurgery for growth hormone-secreting pituitary adenoma in a series of 214 patients. J Neurosurg 68:854–867
Tindall GT, Oyesiku NM, Watts NB, Clark RV, Christy JH, Adams DA (1993) Transsphenoidal adenomectomy for growth hormone-secreting pituitary adenomas in acromegaly: outcome analysis and determinants of failure. J Neurosurg 78:205–215
Kaltsas GA, Isidori AM, Florakis D (2001) Predictors of the outcome of surgical treatment in acromegaly and the value of the mean growth hormone day curve in assessing postoperative disease activity. J Clin Endocrinol Metab 86:1645–1652
Shimon I, Cohen ZR, Ram Z, Hadani M (2001) Transsphenoidal surgery for acromegaly: endocrinological follow-up of 98 patients. Neurosurgery 48:1239–1243
Rudnik A, Zawadzki T, Wojtacha M, Bazowski P, Gamrot J, Galuszka-Ignasiak B, Duda I (2005) Endoscopic transnasal transsphenoidal treatment of pathology of the sellar region. Minim Invasive Neurosurg 48:101–107
Frank G, Pasquini E, Farneti G, Mazzatenta D, Sciarretta V, Grasso V, Faustini Fustini M (2006) The endoscopic versus the traditional approach in pituitary surgery. Neuroendocrinology 83:240–248
Higgins TS, Courtemanche C, Karakla D, Strasnick B, Singh RV, Koen JL, Han JK (2008) Analysis of transnasal endoscopic versus transseptal microscopic approach for excision of pituitary tumors. Am J Rhinol 22:649–652
O’Malley BW Jr, Grady MS, Gabel BC, Cohen MA, Heuer GG, Pisapia J, Bohman LE, Leibowitz JM (2008) Comparison of endoscopic and microscopic removal of pituitary adenomas: single-surgeon experience and the learning curve. Neurosurg Focus 25:E10
Schaberg MR, Anand VK, Schwartz TH, Cobb W (2010) Microscopic versus endoscopic transnasal pituitary surgery. Curr Opin Otolaryngol Head Neck Surg 18:8–14
Gondim JA, Almeida JP, de Albuquerque LA, Gomes E, Schops M, Ferraz T (2010) Pure endoscopic transsphenoidal surgery for treatment of acromegaly: results of 67 cases treated in a pituitary center. Neurosurg Focus 29:E7
Hofstetter CP, Mannaa RH, Mubita L, Anand VK, Kennedy JW, Dehdashti AR, Schwartz TH (2010) Endoscopic endonasal transsphenoidal surgery for growth hormone-secreting pituitary adenomas. Neurosurg Focus 29:E6
Kabil MS, Eby JB, Shahinian HK (2005) Fully endoscopic endonasal vs. transseptal transsphenoidal pituitary surgery. Minim Invasive Neurosurg 48:348–354
Giustina A, Chanson P, Bronstein MD, Klibanski A, Lamberts S, Casanueva FF, Trainer P, Ghigo E, Ho K, Melmed S, Acromegaly Consensus Group (2010) A consensus on criteria for cure of acromegaly. J Clin Endocrinol Metab 95:3141–3148
Trainer PJ, Drake WM, Katznelson L, Freda PU, Herman-Bonert V, van der Lely AJ, Dimaraki EV, Stewart PM, Friend KE, Vance ML, Besser GM, Scarlett JA, Thorner MO, Parkinson C, Klibanski A, Powell JS, Barkan AL, Sheppard MC, Malsonado M, Rose DR, Clemmons DR, Johannsson G, Bengtsson BA, Stavrou S, Kleinberg DL, Cook DM, Phillips LS, Bidlingmaier M, Strasburger CJ, Hackett S, Zib K, Bennett WF, Davis RJ (2000) Treatment of acromegaly with the growth hormone-receptor antagonist pegvisomant. N Engl J Med 342:1171–1177
Carmichael JD, Bonert VS, Mirocha JM, Melmed S (2009) The utility of oral glucose tolerance testing for diagnosis and assessment of treatment outcomes in 166 patients with acromegaly. J Clin Endocrinol Metab 94:523–527
Wilson CB (1979) Neurosurgical management of large and invasive pituitary tumors. In: Tindall GT, Collins WF (eds) Clinical management of pituitary disorders. Raven Press, New York, pp 335–342
Knosp E, Steiner E, Kitz K, Matula C (1993) Pituitary adenomas with invasion of the cavernous sinus space: a magnetic resonance imaging classification compared with surgical findings. Neurosurgery 33:610–617
Hadad G, Bassagasteguy L, Carrau RL, Mataza JC, Kassam A, Snyderman CH, Mintz A (2006) A novel reconstructive technique after endoscopic expanded endonasal approaches: vascular pedicle nasoseptal flap. Laryngoscope 116:1882–1886
Kassam AB, Thomas A, Carrau RL, Snyderman CH, Vescan A, Prevedello D, Mintz A, Gardner P (2008) Endoscopic reconstruction of the cranial base using a pedicled nasoseptal flap. Neurosurgery 63:ONS44–ONS52
Prevedello DM, Thomas A, Gardner P, Snyderman CH, Carrau RL, Kassam AB (2007) Endoscopic endonasal resection of a synchronous pituitary adenoma and a tuberculum sellae meningioma: technical case report. Neurosurgery 60:E401
Paisley AN, Drake WM (2005) Treatment of pituitary tumors: pegvisomant. Endocrine 28:111–114
Esposito V, Santoro A, Minniti G, Salvati M, Innocenzi G, Lanzetta G, Cantore G (2004) Transsphenoidal adenomectomy for GH-, PRL- and ACTH-secreting pituitary tumours: outcome analysis in a series of 125 patients. Neurol Sci 25:251–256
Fahlbusch R, Buchfelder M (1988) Transsphenoidal surgery of parasellar pituitary adenomas. Acta Neurochir (Wien) 92:93–99
Ludecke DK, Abe T (2006) Transsphenoidal microsurgery for newly diagnosed acromegaly: a personal view after more than 1,000 operations. Neuroendocrinology 83:230–239
Mortini P, Losa M, Barzaghi R, Boari N, Giovanelli M (2005) Results of transsphenoidal surgery in a large series of patients with pituitary adenoma. Neurosurgery 56:1222–1233
Nomikos P, Buchfelder M, Fahlbusch R (2005) The outcome of surgery in 668 patients with acromegaly using current criteria of biochemical ‘cure’. Eur J Endocrinol 152:379–387
Gittoes NJ, Sheppard MC, Johnson AP, Stewart PM (1999) Outcome of surgery for acromegaly–the experience of a dedicated pituitary surgeon. QJM 92:741–745
Beauregard C, Truong U, Hardy J, Serri O (2003) Long-term outcome and mortality after transsphenoidal adenomectomy for acromegaly. Clin Endocrinol (Oxf) 58:86–91
Kim MS, Jang HD, Kim OL (2009) Surgical results of growth hormone-secreting pituitary adenoma. J Korean Neurosurg Soc 45:271–274
Kreutzer J, Vance ML, Lopes MB, Laws ER Jr (2001) Surgical management of GH-secreting pituitary adenomas: an outcome study using modern remission criteria. J Clin Endocrinol Metab 86(9):4072–4077
Trepp R, Stettler C, Zwahlen M, Seiler R, Diem P, Christ ER (2005) Treatment outcomes and mortality of 94 patients with acromegaly. Acta Neurochir (Wien) 147(3):243–251 discussion 250-1
De P, Rees DA, Davies N, John R, Neal J, Mills RG, Vafidis J, Davies JS, Scanlon MF (2003) Transsphenoidal surgery for acromegaly in wales: results based on stringent criteria of remission. J Clin Endocrinol Metab 88(8):3567–3572
Brzana JA, Yedinak CG, Delashaw JB, Gultelkin HS, Cook D, Fleseriu M (2011) Discordant growth hormone and IGF-1 levels post pituitary surgery in patients with acromegaly naïve to medical therapy and radiation: what to follow, GH or IGF-1 values? Pituitary [Epub ahead of print]
Alexopoulou O, Bex M, Abs R, T’Sjoen G, Velkeniers B, Maiter D (2008) Divergence between growth hormone and insulin-like growth factor-i concentrations in the follow-up of acromegaly. J Clin Endocrinol Metab 93:1324–1330
Machado EO, Taboada GF, Neto LV, van Haute FR, Corrêa LL, Balarini GA, Shrank Y, Goulart M, Gadelha MR (2008) Prevalence of discordant GH and IGF-I levels in acromegalics at diagnosis, after surgical treatment and during treatment with octreotide LAR. Growth Horm IGF Res 18(5):389–393
Bates AS, Evans AJ, Jones P, Clayton RN (1995) Assessment of GH status in acromegaly using serum growth hormone, serum insulin-like growth factor-1 and urinary growth hormone excretion. Clin Endocrinol (Oxf) 42(4):417–423
Jane JA Jr, Starke RM, Elzoghby MA, Reames DL, Payne SC, Thorner MO, Marshall JC, Laws ER Jr, Vance MD (2011) Endoscopic transsphenoidal surgery for acromegaly: remission using modern criteria, complications, and predictors of outcome. J Clin Endocrinol Metab 96(9):2732–2740
Feelders RA, Bidlingmaier M, Strasburger CJ, Janssen JA, Uitterlinden P, Hofland LJ, Lamberts SW, van der Lely AJ, de Herder WW (2005) Postoperative evaluation of patients with acromegaly: clinical significance and timing of oral glucose tolerance testing and measurement of (free) insulin-like growth factor I, acid labile subunit, and growth hormone-binding protein levels. J Clin Endocrinol Metab 90:6480–6489
Frank G, Pasquini E (2006) Endoscopic endonasal cavernous sinus surgery, with special reference to pituitary adenomas. Front Horm Res 34:64–82
Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau R (2005) Expanded endonasal approach: fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg Focus 19(1):E6
Barges-Coll J, Fernandez-Miranda JC, Prevedello DM, Gardner P, Morera V, Madhok R, Carrau RL, Snyderman CH, Rhoton AL Jr, Kassam AB (2010) Avoiding injury to the abducens nerve during expanded endonasal endoscopic surgery: anatomic and clinical case studies. Neurosurgery 67(1):144–154
Plockinger U (2012) Medical therapy of acromegaly. Int J Endocrinol 2012:268957
Petrossians P, Borges-Martins L, Espinoza C, Daly A, Betea D, Valdes-Socin H, Stevenaert A, Chanson P, Beckers A (2005) Gross total resection or debulking of pituitary adenomas improves hormonal control of acromegaly by somatostatin analogs. Eur J Endocrinol 152(1):61–66
Colao A, Attanasio R, Pivonello R, Cappabianca P, Cavallo LM, Lasio G, Lodrini A, Lombardi G, Cozzi R (2006) Partial surgical removal of growth hormone-secreting pituitary tumors enhances the response to somatostatin analogs in acromegaly. J Clin Endocrinol Metab 91(1):85–92
Karavitaki N, Turner HE, Adams CB, Cudlip S, Byrne JV, Fazal-Sanderson V, Rowlers S, Trainer PJ, Wass JA (2008) Surgical debulking of pituitary macroadenomas causing acromegaly improves control by lanreotide. Clin Endocrinol (Oxf) 8(6):970–975
Bevan JS (2005) Clinical review: the antitumoral effects of somatostatin analog therapy in acromegaly. J Clin Endocrinol Metab 90(3):1856–1863
Maiza JC, Vezzosi D, Matta M, Donadille F, Loubes-Lacroix F, Cournot M, Bennet A, Caron P (2007) Long-term (up to 18 years) effects on GH/IGF-1 hypersecretion and tumour size of primary somatostatin analogue (SSTa) therapy in patients with GH-secreting pituitary adenoma responsive to SSTa. Clin Endocrinol (Oxf) 67(2):282–289
Melmed S, Sternberg R, Cook D, Klibanski A, Chanson P, Bonert V, Vance ML, Rhew D, Kleinberg D, Barkan A (2005) A critical analysis of pituitary tumor shrinkage during primary medical therapy in acromegaly. J Clin Endocrinol Metab 90(7):4405–4410
Nakashima M, Takano K, Matsuno A (2009) Analyses of factors influencing the acute effect of octreotide in growth hormone-secreting adenomas. Endocr J 56(2):295–304
Neggers SJ, van der Lely AJ (2011) Combination treatment with somatostatin analogues and pegvisomant in acromegaly. Growth Horm IGF Res 21(3):129–133
Bates PR, Carson MN, Trainer PJ, Wass JA, UK National Acromegaly Register Study Group (UKAR-2) (2008) Wide variation in surgical outcomes for acromegaly in the UK. Clin Endocrinol (Oxf) 68(1):136–142
Acknowledgments
We appreciate Stephanie Henry, Juliana Kovacs, and Lois Burkhart for their assistance in administrative support. We also acknowledge Drs. Amin Kassam, Ricardo Carrau and Steve Hodak for their involvement in the primary clinical and surgical management of many of the patients reported in this study. This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Sue M. Challinor and Paul A. Gardner contributed equally to this work as principle investigators.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Shin, S.S., Tormenti, M.J., Paluzzi, A. et al. Endoscopic endonasal approach for growth hormone secreting pituitary adenomas: outcomes in 53 patients using 2010 consensus criteria for remission. Pituitary 16, 435–444 (2013). https://doi.org/10.1007/s11102-012-0440-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-012-0440-6