
Abstract
Introduction Beside (cost-)effectiveness, the feasibility of an intervention is important for successful implementation in daily practice. This study concerns the process evaluation of a newly developed participatory return-to-work (RTW) program for workers without an employment contract, sick-listed due to musculoskeletal disorders. The program consisted of a stepwise process, guided by an independent RTW coordinator, aimed at making a consensus-based RTW plan with the possibility of a temporary (therapeutic) workplace. The aims of this study were to describe the reach and extent of implementation of the new program, the satisfaction and experiences of all stakeholders, and the perceived barriers and facilitators for implementation of the program in daily practice. Methods Temporary agency workers and unemployed workers, sick-listed for 2–8 weeks due to musculoskeletal disorders were eligible for this study. Data were collected from the workers; their insurance physicians and labour experts at the Dutch Social Security Agency; RTW coordinators; and case managers from participating vocational rehabilitation agencies. Data collection took place using professionals’ reports, standardized matrices, questionnaires at baseline and at 3-month follow-up, and group interviews with the professionals. Results Of the 79 workers who were allocated to the participatory RTW program group, 72 workers actually started with the intervention. Overall, implementation of the program was performed according to protocol. However, offering of suitable temporary workplaces was delayed with 44.5 days. Results showed satisfaction with the RTW coordinator among the workers and three quarters of the labour experts experienced a minor or major contribution of the presence of the RTW coordinator. Several barriers for implementation were identified, such as the administrative time-investment, unclear information about the program, no timely offering of temporary (therapeutic) workplaces, and the need for additional support in case of complex health problems. Conclusions This study indicates overall feasibility for implementation of the participatory RTW program in daily practice. However, to overcome important barriers, more attention should be paid to improve timely offering of suitable temporary workplaces, to describe more clearly the program goals and the professional’s roles, and to offer additional support for workers suffering from complex multi-causal health problems. Trial registration NTR1047.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In the setting of occupational health care (OHC) research the (cost-)effectiveness of many interventions most often has been studied using a randomized controlled trial (RCT) without evaluating the feasibility of implementation of such an intervention in daily practice. However, success of an intervention does not only depend on the effectiveness of the intervention. Feasibility, i.e. how successfully and how easily the intervention can be implemented in daily practice, is also of crucial importance. The feasibility of successful implementation is determined by multiple factors that can be present on client level, OHC professional level, organisation level, population level, and/or public level [1–3]. The feasibility of an intervention can be evaluated with a process evaluation alongside an RCT [4].
Although, the number of feasibility studies alongside RCTs is still limited in OHC research, some feasibility studies were recently published [5, 6]. These studies demonstrate the importance and added value of investigating implementation and feasibility aspects of newly developed OHC interventions, for example adequate communication between (occupational) health care providers, required time investment, and timing of the start of the intervention.
The above-mentioned process evaluations in the OHC field focused on a (participatory) RTW program aimed at sick-listed employees, i.e. workers with relative permanent employment relationships. However, there is a more vulnerable group within the working population, namely workers without an employment contract and workers with flexible labour agreements, e.g. temporary agency workers. These workers have an increased risk for (long-term) work disability [7, 8], and possibilities for RTW are limited, since in most cases they have no workplace to return to when sick-listed [8–10]. Furthermore, vocational rehabilitation and RTW guidance for this group is unsatisfactory [8]. Hence, the fact that their situation is different, compared to sick-listed regular employees, may have a different influence on the feasibility of an OHC intervention. For example, in the Netherlands an employer is obligated to support a sick-listed employee in his/her RTW process. However, there are no legislative mandates for employers to facilitate RTW of a sick-listed worker without an employment contract, e.g. offering a suitable workplace for (therapeutic) work resumption. Also, when looking at OHC, for sick-listed workers without an employment contract this is performed by an insurance physician of the Social Security Agency (SSA) who has no (direct) contact with an employer/workplace. In contrast, sick-listed employees are guided by an occupational physician who works in close contact with the employer/workplace. Furthermore, workers without an employment contract have a greater distance to the labour market due to a larger proportion of workers with lower credentials, lower income, more females, more (partly) occupationally disabled, and more immigrants [11–13].
This present paper describes the process evaluation of a newly developed participatory RTW program for temporary agency workers and unemployed workers, sick-listed due to musculoskeletal disorders (MSD). This new participatory RTW program was based on a successful RTW intervention for sick-listed employees with low back pain [14, 15] and specifically tailored for the new target group using the Intervention Mapping (IM) protocol [8]. The newly developed participatory RTW program consisted of a stepwise process to identify and solve obstacles for RTW and was aimed at making a consensus-based RTW plan to facilitate (therapeutic) RTW. Because of this specific target group referral to a vocational rehabilitation agency for finding a temporary (therapeutic) workplace was added as an additional (optional) step to the RTW program, compared to the earlier developed participatory RTW programs [14, 16, 17].
The aims of this study were: (1) to describe the reach of the participatory RTW program, (2) to describe to which extent the RTW program was implemented as planned, i.e. performed according to the protocol, (3) to describe the identified obstacles and solutions for RTW, (4) to describe the satisfaction and experiences of the sick-listed workers, the OHC professionals, and the case managers of the contracted vocational rehabilitation agencies, and (5) to describe perceived barriers and facilitators for implementation of the participatory RTW program in daily practise.
Methods
This process evaluation was carried out alongside a RCT on the cost-effectiveness of the newly developed participatory RTW program for temporary agency workers and unemployed workers sick-listed due to MSD, named the STEP-UP project [9]. The Medical Ethics Committee of the VU University Medical Centre (Amsterdam, the Netherlands) approved the study design and all participants signed informed consent.
This process evaluation was (partly) conducted based on the RE-AIM framework, which consists of five dimensions (Reach, Efficacy/Effectiveness, Adoption, Implementation, and Maintenance) to evaluate interventions [18]. The effectiveness of the participatory RTW program on RTW was not evaluated in this feasibility study; these results will be become available in the near future. Effects/outcomes perceived by the participants and health care professionals like perceived usefulness and impact and satisfaction regarding the participatory RTW program were however evaluated in this process evaluation.
Study Population
The population in this study consisted of temporary agency workers and unemployed workers, sick-listed due to MSD, OHC professionals of the SSA (insurance physicians, labour experts, and RTW coordinators), and case managers of the contracted vocational rehabilitation agencies in the eastern part of the Netherlands.
Participants
Temporary agency workers and unemployed workers between 18 and 64 years of age, and sick-listed between 2 and 8 weeks with MSD as principal health complaint for the sickness benefit claim were eligible for participation. Sick-listed workers were excluded in case of: (1) an accepted sickness benefit claim and being sick-listed for more than 8 weeks, (2) not being able to complete questionnaires written in the Dutch language, (3) a conflict with the SSA regarding a sickness benefit claim or a long term disability claim, (4) a legal conflict, e.g. about an injury compensation claim, (5) an episode of sickness absence due to MSD within 1 month before the current sickness benefit claim, (6) a revision or ending of a long-term disability benefit within 1 month before the current sickness benefit claim, or (7) pregnancy until 3 months after delivery. The insurance physicians of the SSA prevented workers from starting with the participatory RTW program in case of a serious psychiatric disorder, a serious cardio-vascular disease, or a terminal disease. The recruitment procedure has been described in detail elsewhere [9].
Occupational Health Care Professionals
The OHC professionals in this study were recruited from the five participating SSA front offices and consisted of insurance physicians, labour experts, and specifically for this study trained RTW coordinators. They all received purposely developed instruction and coaching sessions and were offered personal guidance with the first cases to facilitate working with the participatory RTW program. Next, each SSA front office was asked to form at least two ‘participatory RTW program’ teams, i.e. ‘STEP-UP teams’, consisting of an insurance physician, a labour expert, and a RTW coordinator. Furthermore, the involved staff and management of the SSA agreed to support and facilitate working with the newly developed participatory RTW program.
(Case Managers of) Vocational Rehabilitation Agencies
The vocational rehabilitation agencies were certified commercially operating agencies that agreed to support the participatory RTW program. Each agency appointed a case manager who had contact with the RTW coordinator.
Participatory RTW Program
The participatory RTW program consisted of a step-by-step process to identify and solve obstacles for RTW, aimed at making a consensus-based implementation plan to facilitate (therapeutic) RTW. Involved in this stepwise process were the sick-listed worker, an insurance physician of the SSA, a labour expert of the SSA, and an independent RTW coordinator of the SSA who guided the stepwise process to achieve consensus and to guarantee equality between the sick-listed worker and the labour expert of the SSA. The first step consisted of a (combined) consult with the insurance physician (within 14 days after allocation) and the labour expert (within 14 days after the consult with the insurance physician) to check the eligibility of the sickness benefit claim, and to make a (medical) problem analysis with advising about (functional) limitations for RTW, including the prognosis regarding recovery of health and work ability. In the second step two separate meetings took place between the sick-listed worker and the RTW coordinator, and between the labour expert and the RTW coordinator, respectively, to identify and prioritize obstacles for RTW. This prioritizing of obstacles for RTW was based on frequency (how often do they occur?) and severity (how large is the perceived impact on functioning in daily life and/or work?). Next, in the third step, the sick-listed worker, the labour expert and the RTW coordinator had a joint meeting to brainstorm possible solutions for RTW. This resulted in the fourth step: making of a consensus-based RTW plan describing the prioritised obstacles for RTW, the consensus-based solutions, the person(s) responsible for implementation of each selected solution, and when it should be realized (within 21 days after the consult with the insurance physician). Next, step five was optional and consisted of offering the possibility of a temporary (therapeutic) workplace to create an actual RTW perspective. If chosen for this option, one of the participating vocational rehabilitation agencies was contracted by the RTW coordinator to find a (therapeutic) workplace matching with the formulated consensus-based RTW plan. The aim of this temporary (therapeutic) workplace was to create an opportunity to practice (new) work skills and get work experience. After contracting by the RTW coordinator, the vocational rehabilitation agency had 4 weeks to offer at least two suitable temporary (therapeutic) workplaces. Placement was for a maximum of 3 months. The vocational rehabilitation agencies were asked to use their existing network/contacts with employers to find temporary (therapeutic) workplaces. If necessary, the case manager of the vocational rehabilitation agency offered support to the worker and/or the employer to facilitate working at the temporary workplace. The employers benefited financially because the sick-listed worker received on going supportive sickness benefit from the SSA during the placement in a temporary (therapeutic) workplace, i.e. the employer did not have to page wages. Otherwise, the employer had to make some time investment to guide the sick-listed worker in his/her new work environment and work tasks. If the primary contracted vocational rehabilitation agency did not succeed in offering a suitable temporary workplace within 28 days after referral the other participating vocational rehabilitation agencies could also be contracted. Furthermore, a financial reward was given by the SSA to the vocational rehabilitation agency for placement in a suitable temporary (therapeutic) workplace. Finally, in the sixth step, 6 weeks after the brainstorm session, the RTW coordinator evaluated actual realization of the RTW implementation plan, i.e. realization of the selected solutions, including the contribution to RTW [8, 9].
Data Collection
The data for this study were collected using questionnaires (at baseline and 3-month follow-up) and standardized matrices (resulting from the brainstorm session and consensus meeting with the RTW coordinator). In addition, data were also obtained from a computerized support system specially made for the involved SSA professionals in this study to facilitate following the participatory RTW protocol, from the client files at the SSA, and from the SSA database records after 1-year follow-up. Finally, 3 months after allocation of the last sick-listed worker to the intervention group, i.e. after all 79 participants in the intervention group had had the opportunity to receive the participatory RTW program, group interviews were held with the insurance physicians, the labour experts, the RTW coordinators, management and staff members of the SSA, and representatives of the participating vocational rehabilitation agencies.
Outcome Measures
Reach
Reach was addressed at participant’s level and project level. At participant’s level, reach was defined as the number of workers who participated in the research. The number of approached sick-listed workers for this study; the number of workers who were eligible for participation; and the number of workers who actually participated in the study were registered. All participants completed a baseline questionnaire, providing background information. At project level, reach was defined as the number of settings (SSA front offices and vocational rehabilitation agencies) and the representatives of these settings (OHC professionals and case managers, respectively) who participated in the research. The number of OHC professionals and the (case managers of the) vocational rehabilitation agencies who were eligible and actually participated in the study was registered. On both levels reasons for non-participation were registered.
Implementation of the Participatory RTW Program According to the Protocol
Timeline and Content of the Participatory RTW Program
To determine whether the RTW program was implemented according to the protocol the content of the applied program (i.e. which steps were realized?) and the timeline (i.e. start and duration between the performed steps) was evaluated for each participant. This was primarily reported by the RTW coordinator using the questionnaire at 3-month follow-up. The information given by the RTW coordinator was compared to and, if necessary, supplemented by information from the client files at the SSA and the SSA database records after 1 year of follow-up. Finally, if information was still missing additional data were collected from the professionals reports stored in the computerized support system designed for this study. In case of non-compliance the reason for this was registered in the questionnaire sent to the OHC professionals at 3-month follow-up and in the reports in the computerized support system.
Obstacles and Solutions for RTW (step 2, 3 and 4)
The identified and prioritized obstacles for RTW, the proposed solutions, and the consensus-based RTW plan were registered in standardized matrices by the RTW coordinator. To classify the obstacles and solutions for RTW the Ergonomic Abstract classification scheme was used [5, 19, 20]. In accordance with this classification scheme the categories consisted of: workplace and equipment, work design and organization, environment, task-related factors, performance-related factors, economic impact of the system, and other fields.
(Therapeutic) Workplace (step 5)
The realisation of temporary (therapeutic) workplaces, including the type of work offered, was registered in the case manager reports of the vocational rehabilitation agencies. If placement in a temporary workplace was not realised, the case manager of the agency registered the reason for this.
Satisfaction, Perceived Usefulness, and Impact of the Participatory RTW Program
Satisfaction, perceived usefulness, and the impact on RTW of the participatory RTW program were evaluated using questionnaires at 3-month follow-up from all involved stakeholders, i.e. the worker, the insurance physician, the labour expert, the RTW coordinator, and, if applicable, the case-manager of the contracted vocational rehabilitation agency. Whether the workers felt that they were taken seriously by the insurance physician, the labour expert, and the RTW coordinator was evaluated using the short version of the Patient Satisfaction Occupational Health Services Questionnaire, based on a five-point scale ranging from no agreement to full agreement [21].
Barriers and Facilitators for Adoption and Implementation of the Participatory RTW Program
In the 3-month follow-up questionnaire the involved OHC professionals and case managers of the vocational rehabilitation agencies were asked about their experienced barriers and facilitators for implementation. In addition, when all participants in the intervention group had had the opportunity to receive the new participatory RTW program, i.e. 3 months after inclusion of the last intervention group participant, group interviews were held among the staff, management and involved OHC professionals of the SSA, and the case managers of the vocational rehabilitation agencies. To ask their view on the applicability of the program in daily practise, focusing on important barriers and facilitators for implementation. The content of these group interviews was based on the principles of context analysis as proposed by Grol and Wensing [22, 23] and consisted of four themes: the innovation itself, the users, the target group, and the context.
Data Analysis
The data were analyzed by means of descriptive statistics. SPSS 15 and Excel 2003 were used. The Ergonomic Abstract classification scheme [19, 20] was used to classify the obstacles and solutions for RTW as registered in the standardized matrices. Two researchers (KMB and SJV) performed the classification of the obstacles and solutions independently. Disagreements between the researchers were discussed to achieve consensus, and, if necessary, a third researcher (JRA) was consulted. The group interviews were tape-recorded and transcribed. All mentioned barriers and facilitators for implementation were extracted from the transcripts and coded. These coded snippets were classified by two researchers (KMB and SJV) independently based on the principles of context analysis [22, 23]. Disagreements between the researchers were discussed to achieve consensus and, if necessary, a third researcher (JRA) was consulted [24].
Results
Reach
Participant’s Level
Figure 1 shows the flow diagram of the sick-listed workers in the study. Between February 2007 and July 2008, 3807 temporary agency workers and unemployed workers, sick-listed for 1–2 weeks due to MSD, received a letter with a screening questionnaire from the insurance physician of the SSA on behalf of the researchers. Based on the returned screeners, 784 sick-listed workers were eligible for participation. They were contacted by telephone to provide additional information about the study and to check eligibility. The main reasons for non-participation were non-response on the screener (n = 2249), not interested in participation (n = 466), and not meeting the inclusion criteria (n = 308). After the telephone contact an intake meeting was planned with 266 sick-listed workers. The main reasons for not planning an intake were not meeting the inclusion criteria (n = 327) and not willing to participate (n = 191). Finally, 163 sick-listed workers were enrolled in the study. The remaining 103 workers were not enrolled due to several reasons (Fig. 1).

Flow diagram of sick-listed workers in the STEP-UP study
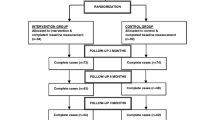
Randomization and allocation to the participatory RTW program group or usual care group was performed after informed consent and baseline measurement. Obviously, the present paper only reports on the participants allocated to the intervention group. Finally, after enrolment, seven sick-listed workers did not start with the participatory RTW program. The main reason for not starting was full recovery from MSD before start of the program (n = 3). Figure 2 shows the flow diagram of the sick-listed workers in the RTW program after allocation. The baseline characteristics of the participants who started with the participatory RTW program (n = 72) are shown in Table 1. These participants did not significantly differ from the sick-listed workers who did not start with the RTW program.

Flow diagram of sick-listed workers in the RTW program after allocation
Project Level
The board of five front offices of the SSA in the eastern part of the Netherlands was approached for participation and responded positive. The OHC professionals from these SSA offices were invited for training in working with the participatory RTW program. In total, 29 insurance physicians, 24 labour experts, and 30 case managers from the five SSA front offices completed the instruction and coaching program. Next, each SSA office was asked to form two ‘participatory RTW program’ teams. Finally, seven insurance physicians, eight labour experts, and nine RTW coordinators responded positively and formed ‘STEP-UP’ teams at the SSA offices. The main reason for not willing to participate in the study was the (perceived) time investment. During the study one insurance physician and one labour expert started working elsewhere and were replaced by a new professional, who received a syllabus with detailed information about the participatory RTW program and was offered personal guidance with the first cases to facilitate working with the participatory RTW program.
The four commercially operating vocational rehabilitation agencies that participated were: Olympia, Adeux, Capability, and Randstad Rentrée. Each agency appointed a case manager for the participatory RTW program.
Implementation of the Participatory RTW Program According to the Protocol
Timeline and Content of the Participatory RTW Program
Table 2 shows the timeline of the RTW program. The first four steps of the RTW program were performed according to the timeline of the protocol. In the fifth step of the RTW program delay appeared. The median duration between contracting the primary vocational rehabilitation agency and placement in a matching (therapeutic) workplace was 72.5 days (IQR 46.3–96.0), compared to 28 days as dictated by the protocol. The most mentioned reasons for this delay were: (1) no results by the primary vocational rehabilitation agency within 28 days after referral whereupon the other vocational rehabilitation agencies were also contracted, and (2) the summer vacancies wherein professionals or participants were not available in time.
After the first consult with the insurance physician (step one), according to the protocol, participation in the RTW program stopped for 34 sick-listed workers because of: full work ability established by the insurance physician with ending of sickness benefit (claim closure) (n = 23), absence of work ability on medical grounds for at least 3 months (n = 10), and full recovery from MSD with ending of sickness benefit (claim closure) (n = 1). In total, 38 of the 72 sick-listed workers (53%) participated in the meetings with the RTW coordinator, i.e. the inventory of obstacles for RTW (step two), the brainstorm session to think about solutions (step three), and the making of a consensus-based RTW plan (step four). Figure 2 shows the flow diagram of the sick-listed workers in the RTW program after allocation.
Obstacles and Solutions for RTW (step 2, 3 and 4)
In total, 98 obstacles for RTW were identified and prioritized. Most of these obstacles were related to the physical workload (27%), commuting (16%), low level of education and/or work (15%), job design (13%), and work schedule (8%). The most frequently mentioned solution in the brainstorm meetings was to find (other) physically less demanding work. Table 3 shows examples of identified obstacles for RTW and proposed solutions to achieve RTW.
The RTW coordinators reported that 65% of the sick-listed workers actively cooperated in the participatory RTW program, whereas 32% of the sick-listed workers were passively cooperative. Only one sick-listed worker did not cooperate. According to the RTW coordinators and the insurance physicians they mostly advised the sick-listed workers physically less demanding work and other less demanding tasks in previous work. The sick-listed workers reported they got advised mostly: decrease of physical workload, change of workplace, and other less demanding tasks in previous work.
The mean duration of a meeting with the RTW coordinator was 71 min and the mean number of meetings was 2.4 during the RTW program. The mean total time investment for performing the RTW program for the RTW coordinator was 3 h and 54 min.
(Therapeutic) Workplace (step 5)
In total, 30 sick-listed workers were referred to a vocational rehabilitation agency. Of these 30 workers, 15 were offered two (therapeutic) workplaces, seven workers were offered three (therapeutic) workplaces, seven workers were offered no workplace at all, and for one worker this remained unknown. The reasons for not offering a workplace were: sick-listed worker refused to participate (n = 1), sick-listed worker found suitable work on own initiative (n = 1), increased work disability (n = 1), priority given to medical treatment of sick-listed worker (n = 1), and unknown (n = 3). Subsequently, 19 of the 30 sick-listed workers were actually placed in a temporary (therapeutic) workplace. Two vocational rehabilitation agencies were not able to offer suitable (therapeutic) workplaces. One agency placed one sick-listed worker in a (therapeutic) workplace and one agency (Olympia) placed 18 sick-listed workers in a temporary (therapeutic) workplace. In the view of the RTW coordinator almost all of the sick-listed workers (97%) had sufficient say in choosing a suitable temporary workplace. Table 4 shows the type of realised temporary (therapeutic) workplaces.
Furthermore, four sick-listed workers found a suitable workplace on own initiative and three workers were placed in a temporary (therapeutic) workplace through the personal network of their labour expert. In total, 26 of the 38 sick-listed workers who completed the consensus based RTW plan (68%) returned to work.
Satisfaction, Perceived Usefulness, and Impact of the Participatory RTW Program
Meetings
The majority of the sick-listed workers felt taken seriously during the meetings with the OHC professionals. Figure 3 shows the extent to which the sick-listed worker felt taken seriously by the RTW coordinator. Three quarters of the labour experts experienced a minor or major contribution of the presence of the RTW coordinator in the meetings to the sense of security and the sense of support of the sick-listed worker, and the perceived equality between the sick-listed workers and the labour expert (Table 5).

Taken seriously by the RTW coordinator (RTWC) during the meetings from the perspective of the worker (n = 47)
The satisfaction score for the meeting with the insurance physician was 7.3 (SD 2.1) on a 1–10 scale. The majority of sick-listed workers were satisfied with the OHC professionals (63% with the insurance physician, 66% with the labour expert, and 72% with the RTW coordinator).
Consensus-Based RTW Plan, (Therapeutic) Workplace and Computerized Support System
Table 6 shows the satisfaction and the perceived usefulness with regard to the consensus-based RTW plan and the temporary (therapeutic) workplace, including the perceived impact on RTW. Approximately a third of the labour experts were dissatisfied with the resulting consensus-based RTW plan and the finding of temporary (therapeutic) workplaces. Most of the sick-listed workers and the labour experts had a positive or neutral opinion about their satisfaction with and the usefulness of the consensus-based RTW plan and the temporary (therapeutic) workplace, and the impact of those on RTW. Most of the case managers from the vocational rehabilitation agencies experienced a facilitating impact on RTW of both the consensus-based RTW plan (67%) and the offering of a (therapeutic) workplace (55%).
The majority of the OHC professionals (86% of the insurance physicians, 71% of the labour experts, and 90% of the RTW coordinators) used the computerized support system. Most OHC professionals were satisfied with the computerized support system with respect to the support in working with the RTW program and support in communication between all involved professionals.
Barriers and Facilitators for Adaptation and Implementation of the Participatory RTW Program
Questionnaires
After each participatory RTW program, the OHC professionals and, if applicable, the case manager of the vocational rehabilitation agency were asked to evaluate the process of implementation by assessing various factors as neutral, impeding, or facilitating.
The main facilitating factors were: time investment, expected effectiveness, confidence of the sick-listed worker in the professionals, commitment of the sick-listed worker and the RTW coordinator regarding the placement in a temporary workplace, sufficient say of the sick-listed worker and the labour expert regarding choosing a suitable temporary workplace, and possibility of a suitable temporary (therapeutic) workplace.
The main impeding factors were: insufficient disease insight of sick-listed workers according to the insurance physician, no timely offering of a suitable temporary (therapeutic) workplace, and commitment of the sick-listed worker regarding the temporary workplace.
Group Interviews
Three months after inclusion of the last participant in the participatory RTW program group, representatives of the staff, management and involved OHC professionals of the SSA, and the case managers of the participating vocational rehabilitation agencies were asked to evaluate the overall implementation. In total 9 involved professionals took part in the group interviews. The following themes were discussed: the innovation itself, the users, the target group, and the context.
Examples of barriers mentioned at the innovation level were: the administrative burden, i.e. the time it took to fill in all the forms, difficulty to distinguish between the role of the RTW coordinator and the role of the labour expert, placement in a (therapeutic) workplace perceived as the main goal of the RTW program instead of making a consensus-based RTW plan, and no possibility to punish the sick-listed worker in case of noncompliance with the RTW action plan, e.g. imposing a benefit sanction. Examples of the mentioned facilitators at the innovation level were: focus on early restoring of activities including RTW, much attention paid to active involvement of the sick-listed worker, and the possibility of a temporary workplace, i.e. the opportunity to attempt (therapeutic) work resumption.
At the user level examples of barriers were: unclear information about the main goals of the RTW program, perceived restriction of professional autonomy by following a protocol, and top down introduction of the program. Examples of the mentioned facilitators at the user level were: most SSA teams managed to plan the meetings in time, fast and mindful transfer of sick-listed workers between OHC professionals facilitated the focus on early restoring of activities including RTW, and using a computerized support system to ensure sufficient communication between the involved professionals.
At the target group level examples of barriers were: many sick-listed workers with complex, multi-causal health problems (e.g. not just MSD, but also psychosocial problems), and expectations of the sick-listed workers not always in accordance with the RTW program. An example of the mentioned facilitators at the target group level was that the sick-listed workers were positive about the presence of the RTW coordinator.
Examples of barriers at the context level were: less flexible consult planning opportunities at some of the SSA offices, and less support due to changes in management at the SSA during the study. An example of the mentioned facilitators at the context level was the financial incentive for both the participating vocational rehabilitation agencies and the employers to find and offer suitable (temporary) workplaces.
Discussion
This paper aimed to describe the implementation process, satisfaction and experiences with a newly developed participatory RTW programs reported by temporary agency workers and unemployed workers, sick-listed due to MSD, their OHC professionals at the SSA, and their case managers of the participating vocational rehabilitation agencies. Overall, implementation of the program was performed according to protocol and the results showed satisfaction with the RTW coordinator among workers. Three quarters of the labour experts experienced a minor or major contribution of the presence of the RTW coordinator. However, timely placement in a suitable temporary (therapeutic) workplace after referral to a vocational rehabilitation agency proved to be difficult.
Comparison with Other Studies
Comparison of the type of obstacles for RTW identified by workers on sick leave due to low back pain in previous studies shows that the obstacles related to physical workload and job design found in this study are comparable with earlier findings [6, 14]. However, in this study obstacles for RTW related to commuting and low level of education and/or work were also frequently mentioned. This difference could be associated with the different target group. Having a low level of education and/or work seems to be more common for temporary agency workers and unemployed workers than for workers with an employment contract. For example, the education level in the baseline characteristics found in a comparable study among employees on sick leave due to low back pain (21% low and 52% intermediate education) [25] was indeed higher than the education level found in this study (56% low and 36% intermediate education). These differences probably contribute to the finding that sick-listed workers without an employment contract encountered different obstacles in returning to work, compared to sick-listed employees.
The majority of the sick-listed workers were satisfied with the independent role of the RTW coordinator and three quarters of the labour experts experienced a minor or major contribution of the presence of the RTW coordinator in the meetings. However, a substantial number of the labour experts were dissatisfied with the resulting consensus-based RTW plan and the finding of suitable temporary workplaces. In addition, most professionals participating in the group interviews expressed difficulty to distinguish between the role of the RTW coordinator and the role of the labour expert. This limited satisfaction may be partly caused by the difficulties in finding and timely offering of suitable temporary workplaces. The unclear role of the RTW coordinator should be taken into account when implementing the participatory RTW program on a wider scale. It might be possible that the RTW coordinators in this study did not have all competences required for this role [26, 27] or that the professional’s roles and the program goals were not clearly enough described. This might affect the implementation of the program and can be improved when implementing the program on a wider scale.
In earlier studies a participatory RTW program seemed to be feasible for sick-listed workers with distress problems or with low back pain [5, 6, 14]. In the present study the OHC professionals and the case managers of the vocational rehabilitation agencies found the participatory RTW program less suitable for sick-listed workers with complex, multi-causal health problems. They preferred referral of workers with no co-morbidity. The combination of physical and psychosocial problems seemed to be difficult to handle. This might be caused by unclear information about the target group during the training of the OHC professionals. When implementing the RTW program in daily practice, attention should be paid to applying the RTW program to sick-listed workers with complex health problems. If necessary, additional support should be offered for workers suffering from these complex health problems.
The exclusion criteria in this study were comparable with the exclusion criteria used in earlier studies [5, 6, 14]. Sick-listed workers with a (legal) conflict regarding a sickness benefit claim, a long term disability claim or an injury compensation claim were excluded due to the fact that mediation in a (legal) conflict is not the aim of the participatory RTW program, i.e. instead of trying to reconcile between two contending parties the aim of the new RTW program is to reach consensus on how to achieve RTW. In addition, many of the sick-listed workers who participated in the study suffered from complex health problems, which is characteristic for this target group. Therefore, we believe that the sick-listed workers participating in this study are sufficiently representative with regard to the feasibility of the participatory RTW program in daily practice.
Strengths and Limitations of this Study
Since all stakeholders have different interests in the OHC field, a strength of this study is evaluating the experiences of all involved stakeholders (sick-listed workers, OHC professionals, and the case managers of the vocational rehabilitation agencies) with the RTW program.
Another strength of this study is that the performance of the program according to the protocol was measured using multiple sources, i.e. (1) several questionnaires, (2) the SSA database records and client files, and (3) the reports in the for this study newly developed computerized support system at the SSA, with subsequent comparison of these data. In addition, satisfaction and experiences with the participatory RTW program were also measured using multiple sources and mixed methods (questionnaires and group interviews).
A methodological limitation of this study is that selection bias might have occurred, because only interested sick-listed workers and professionals participated in the study.
In this study the difficulties regarding the performance of the selected vocational rehabilitation agencies may have been underestimated, i.e. how the vocational rehabilitation agencies actually cope with finding and offering a (therapeutic) workplace. A possible solution for this might have been to perform a pilot study to establish the working procedures of the involved vocational rehabilitation agencies, including the network of (willing) employers for suitable temporary workplaces, prior to the start of the RCT.
Practical Implications
This study indicates overall feasibility for implementation of the participatory RTW program in daily practice. However, the majority of the participating vocational rehabilitation agencies experienced difficulties in finding and timely offering of suitable (therapeutic) workplaces. The delay in finding suitable temporary workplaces might be due to the inexperience of the vocational rehabilitation agencies in working with the new RTW program and/or not having optimal working procedures for this. Therefore, more attention should be paid to improve the finding and timely offering of suitable temporary (therapeutic) workplaces. This could be improved by (more) stringent selection of the vocational rehabilitation agencies, by training the case managers of these agencies, and by creating a database of suitable temporary workplaces.
For broader implementation it also seems essential to pay more attention to describing more clearly the program goals and the professional’s roles. Moreover, it should be made clear that the program is also suitable for sick-listed workers with complex health problems, for whom additional support should be arranged. Furthermore, limiting the administrative time-investment is recommended.
Finally, we believe that the feasibility of the participatory RTW program is not significantly more difficult if not limited to those who are willing to participate, i.e. willing to provide informed consent. The group interviews with the OHC professionals revealed that the voluntary nature of the study could interfere with the obligations of the sick-listed worker to cooperate with regard to his/her recovery, (vocational) rehabilitation and RTW (as dictated by the Dutch Improved Gatekeeper Act). For instance, they missed the possibility to impose a benefit sanction in case of noncompliance with the RTW action plan. Therefore, it might even be easier to implement the new participatory RTW program in daily practice compared to this study.
Conclusions
This study indicates overall feasibility for implementation of the participatory RTW program in daily practice. However, more attention should be paid to improve the timely offering of suitable temporary workplaces. In addition, for broader implementation it seems essential to pay more attention to describing more clearly the program goals and the professional’s roles, and to offer additional support for workers suffering from complex health problems.
Abbreviations
- OHC:
-
Occupational health care
- RCT:
-
Randomized controlled trial
- RTW:
-
Return to work
- MSD:
-
Musculoskeletal disorders
- SSA:
-
Social Security Agency
References
Goldenhar LM, LaMontagne AD, Katz T, Heaney C, Landsbergis P. The intervention research process in occupational safety and health: an overview from the National Occupational Research Agenda Intervention Effectiveness Research team. J Occup Environ Med. 2001;43:616–22.
Grol R. Successes and failures in the implementation of evidence-based guidelines for clinical practice. Med Care. 2001;39:II46–54.
Young AE, Waisak R, Roessler RT, McPherson KM, Anema JR, van Poppel MNM. Return-to-work outcomes following work disability: stakeholder motivations, interests and concerns. J Occup Rehabil. 2005;15:543–56.
Oakley A, Strange V, Bonell C, Allen E, Stephenson J, RIPPLE study team. Process evaluation in randomized controlled trails of complex interventions. Br Med J. 2006;332:413–6.
Van Oostrom SH, van Mechelen W, Terluin B, de Vet HCW, Anema JR. A participatory workplace intervention for employees with distress and lost time: a feasibility evaluation within a randomized controlled trial. J Occup Rehabil. 2009;19:212–22.
Lambeek LC, van Mechelen W, Buijs PC, Loisel P, Anema JR. An integrated care program to prevent work disability due to chronic low back pain: a process evaluation within a randomized trail. BMC Musculoskelet Disord. 2009;10:147.
Vermeulen SJ, Tamminga SJ, Schellart AJM, Ybema JF, Anema JR. Return-to-work of sick-listed workers without an employment contract—what works? BMC Public Health. 2009;9:232.
Vermeulen SJ, Anema JR, Schellart AJM, Van Mechelen W, Van der Beek AJ. Intervention mapping for development of a participatory return-to-work intervention for temporary agency workers and unemployed workers sick-listed due to musculoskeletal disorders. BMC Public Health. 2009;9:216.
Vermeulen SJ, Anema JR, Schellart AJM, Van Mechelen W, Van der Beek AJ. Cost-effectiveness of a participatory return-to-work intervention for temporary agency workers and unemployed workers sick-listed due to musculoskeletal disorders: design of a randomized controlled trial. BMC Musculoskelet Disord. 2010;11:60.
Ydema JF, Evers M, Lagerveld S, van den Berg R, van Vuren T. TNO-rapport Werking Wet verbetering Poortwachter onder vangnetters. Eerste cohort, herhaalonderzoek eerste cohort en tweede cohort [TNO report Working improvement gatekeeper law among non-employees. First cohort, repeated research first cohort and second cohort]. Hoofddorp: TNO; 2006.
Benach J, Amable M, Muntander C, Benavides FG. The consequences of flexible work for health: are we looking at the right place? J Epidemiol Community Health. 2002;56:405–6.
Arents MR, Dorenbos I, Vogelaar B, Vrijhof B, Landheer W. Aard en oorzaken ziekteverzuim Uitzendbranche [Nature and causes sickness absence among temporary agency workers]. Rotterdam: ECORYS-NEI; 2003.
Veerman TJ. Vroegtijdige reïntegratie uitzendkrachten [Early return-to-work of temporary agency workers]. Leiden: Astri; 2005.
Anema JR, Steenstra IA, Urlings IJ, Bongers PM, de Vroome EM, van Mechelen W. Participatory ergonomics as a return-to-work intervention: a future challenge? Am J Ind Med. 2003;44:273–81.
Anema JR, Steenstra IA, Bongers PM, de Vet HCW, Knol DL, Loisel P, van Mechelen W. Multidisciplinary rehabilitation for subacute low back pain: graded activity or workplace intervention of both? A randomized controlled trial. Spine. 2007;32:291–8.
Van Oostrom SH, Anema JR, Terluin B, de Vet HCW, Knol D, van Mechelen W. Cost-effectiveness of a workplace intervention for sick-listed employees with common mental disorders: design of a randomized controlled trial. BMC Public Health. 2008;8:12.
Loisel P, Gosselin L, Durand P, Lemaire J, Poitras S, Abenhaim L. Implementation of a participatory ergonomics program in the rehabilitation of workers suffering from subacute back pain. Appl Ergonomics. 2001;32:53–60.
Glasgow RE. RE-AIMing research for application: ways to improve evidence for family medicine. J Am Board Fam Med. 2006;19:11–9.
Stapleton C. Classification scheme. In: Ergonomics abstracts, vol 32. London: Taylor & Francis Ltd; 2000 pp i–vii.
National Institute for Occupational Safety and Health. National Occupational Research Agenda (NORA). Cincinnati, OH: US Department of Health and Human Services; 1996.
Verbeek JH, de Boer AG, van der Weide WE, Piirainen H, Anema JR, van Amstel RJ, Hartog F. Patient satisfaction with occupational health physicians, development of a questionnaire. Occup Environ Med. 2005;62:119–23.
Grol R, Wensing M. What drives change? Barriers to and incentives for achieving evidence-based practice. Med J Aust. 2004;180(6 Suppl):S57–60.
Grol R, Wensing M. Implementatie: Effectieve verbetering van de patiëntenzorg [Implementation: effective improvement of patient care]. Maarssen: Elsevier gezondheidszorg; 2006.
Boeije HR. Analyseren in kwalitatief onderzoek [Analysis in qualitative research]. Hoofddorp: Boom Onderwijs; 2005.
Lambeek LC, van Mechelen W, Knol DL, Loisel P, Anema JR. Randomised controlled trial of integrated care to reduce disability from chronic low backpain in working, private life. Br Med J. 2010;340:c1035.
Pranksy G, Shaw WS, Loisel P, Hong QN, Désorcy B. Development and validation of competencies for return to work coordinators. J Occup Rehabil. 2010;20(1):41–8.
Shaw W, Hong QN, Pransky G, Loisel P. A literature review describing the role of return-to-work coordinators in trial programs and interventions designed to prevent workplace disability. J Occup Rehabil. 2008;18:2–15.
Acknowledgments
We would like to thank all involved workers, insurance physicians, labour experts, RTW coordinators, case managers of the vocational rehabilitation agencies, and the staff and management of the involved SSA for participation in this study. This study was financially supported by the Dutch Institute for Employee Benefit schemes (UWV).
Conflict of interest
The authors declare that they have no competing interests.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
van Beurden, K.M., Vermeulen, S.J., Anema, J.R. et al. A Participatory Return-to-Work Program for Temporary Agency Workers and Unemployed Workers Sick-Listed Due to Musculoskeletal Disorders: a Process Evaluation Alongside a Randomized Controlled Trial. J Occup Rehabil 22, 127–140 (2012). https://doi.org/10.1007/s10926-011-9314-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10926-011-9314-4