
Abstract
Familial microscopic hematuria (MH) of glomerular origin represents a heterogeneous group of monogenic conditions involving several genes, some of which remain unknown. Recent advances have increased our understanding and our ability to use molecular genetics for diagnosing such patients, enabling us to study their clinical characteristics over time. Three collagen IV genes, COL4A3, COL4A4, and COL4A5 explain the autosomal and X-linked forms of Alport syndrome (AS), and a subset of thin basement membrane nephropathy (TBMN). A number of X-linked AS patients follow a milder course reminiscent of that of patients with heterozygous COL4A3/COL4A4 mutations and TBMN, while at the same time a significant subset of patients with TBMN and familial MH progress to chronic kidney disease (CKD) or end-stage kidney disease (ESKD). A mutation in CFHR5, a member of the complement factor H family of genes that regulate complement activation, was recently shown to cause isolated C3 glomerulopathy, presenting with MH in childhood and demonstrating a significant risk for CKD/ESKD after 40 years old. Through these results molecular genetics emerges as a powerful tool for a definite diagnosis when all the above conditions enter the differential diagnosis, while in many at-risk related family members, a molecular diagnosis may obviate the need for another renal biopsy.
Similar content being viewed by others

Introduction
Microscopic hematuria (MH) of glomerular origin is a symptom of a heterogeneous group of conditions that can be either sporadic and acquired, or familial and inherited related to several genes, some of which remain unknown. As a safe general guideline, familial MH is best confirmed by demonstrating microhematuria in a number of first-degree relatives, each one tested positive at least twice at different intervals. Familial MH usually develops in early childhood and continues until late in life and until death, characterized by an unpredictable risk of progression to chronic kidney disease (CKD) or by age-dependent penetrance.
MH of hereditary or non-hereditary nature is a frequent finding in the general population, loosely defined as the presence of over 3–5 red blood cells per high power field in the light microscope. Glomerular origin MH can be distinguished from non-glomerular with the use of phase contrast urine microscopy. MH persists for life, sometimes intermittently; therefore the more often an individual is tested for hematuria, the more likely it is to be found.
It has been reported that the frequency of MH can be as high as 1%, although different reports have mentioned frequencies as high as 20% of the general population [1]. It is unknown what portion of MH in the general population is of hereditary nature. In this review, we focus on two major forms of MH, the heritable collagen IV nephropathies and the newly revisited C3 glomerulopathy caused by mutations in the CFHR5 gene. For reasons of completeness, we should mention that mutations in the MYH9 gene (nonmuscle myosin heavy chain IIA) define a spectrum of rare autosomal dominant macrothrombocytopenias that present as familial hematurias. There are four clinical entities: the May-Hegglin anomaly, and the Fechtner, Sebastian, and Epstein syndromes, which represent a variable expression of a single illness, and they share ultrastructural features with AS while they are associated with sensorineural deafness [2–4]. Hematuria may also be the presenting symptom of other non-glomerular capillary diseases, such as polycystic kidney disease, hypercalciuria, and other familial forms of urolithiasis.
An episode of macroscopic hematuria in childhood or adolescence, even painless, rarely passes unnoticed, and invariably leads to an urgent urology or nephrology consultation. The differential diagnosis is wide open, and IgA nephropathy (IgAN) may be the commonest cause. On the contrary, pure MH often remains unnoticed for a long time and initially not enough attention is paid to its presence. What is important to realize is that persistent MH, occasionally with episodes of macroscopic hematuria may be familial and hereditary and the investigation of a child or young adult with continuous MH may not be complete unless both parents and all siblings have had a morning specimen of urine examined with a microscope or a suitable urine tape, as a routine procedure. A careful family history is also essential. When these two steps are done, an increasing number of families with hereditary hematuria are encountered.
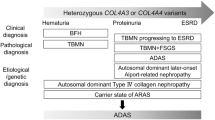
For patients with inherited continuous MH with or without episodes of macroscopic hematuria and a pathophysiology that centers on abnormalities in the structure of the glomerular basement membrane (GBM), the differential diagnosis includes: (1) the X-linked male Alport syndrome patients [5–9], (2) all related heterozygous female carriers of an X-linked mutation that invariably exhibit lifelong MH [6, 7, 9–11], (3) the autosomal recessive male and female Alport patients [6, 7, 12], (4) all male and female COL4A3/A4 heterozygous carriers that exhibit thin basement membrane nephropathy (TBMN) with lifelong MH [6, 7, 13–15], and (5) since 2009 the newly described CFHR5 nephropathy with normal GBM and isolated C3 mesangial deposits, a hereditary nephritis related to a loss-of-function mutation in one of the genes of complement Factor H family, CFHR5, which has a pivotal role in the regulation of the alternate complement pathway [16, 17]. Yet other causes may exist, as in our center alone we have over 35 families with apparent hereditary hematuria where no definite cause has yet been identified. IgAN, currently the most common glomerulonephritis presents with episodes of macroscopic hematuria after upper respiratory tract infections (URTI), followed for long periods of time by MH. There is usually no family history but familial clustering has been observed, although no specific genes have been cloned. A recent study of a large IgAN family localized a novel susceptibility locus to chromosome 2q36 but no gene has yet been cloned [18]. Also, genome-wide association studies using sporadic cases mapped five susceptibility genes, three in the major histocompatibility complex, one on chromosome 22q12, and a common deletion of genes CFHR1-CFHR3 at chromosome 1q32 that are known to be implicated in complement regulation [19].
What is of great interest is the currently unpredictable long-term progression of these hematuric patients to proteinuria, CKD and ESKD, most probably owing to the negative contribution of various unknown modifying factors, presumably of genetic and/or environmental nature. Equally interesting is the fact that the underlying pathophysiology of these microhematuria is not always clear. Unfortunately, and until very recently, these young familial hematuric patients were not routinely submitted to an early renal biopsy to include electron microscopy. Instead, a "wait-and-see" approach until proteinuria developed was followed by many experts [20]. The recent recognition of the pure isolated C3 nephropathy and the additional possibility of TBMN may now help to shift the clinician’s decision towards an earlier renal biopsy in combination with molecular genetics studies.
Molecular biology of collagen IV nephropathies
Most Alport cases (85%) are caused by mutations in the X-linked gene, COL4A5, which encodes the α5 chain of type IV collagen, the most abundant structural protein in the GBM. The remaining 15% of cases are caused by autosomal recessive mutations in the genes that encode the α3 and α4 chains of the type IV collagen, COL4A3/COL4A4 [21, 22]. Collagen type IV, as all collagens, is a trimer formed by combinations of three of the six alpha chains, α1-α6. Genes COL4A1 and COL4A2 map to chromosome 13q34, COL4A3 and COL4A4 map to chromosome 2q36–q37, and COL4A5 and COL4A6 map to Xq22-23. All six genes are encoded in nearly 50 exons and close to 1,600 amino acids, and consist of an N-terminal 7S domain, a C-terminal non-collagenous (NC1) domain and a large collagenous domain in between, containing the characteristic Gly-X-Y repeat, common to all collagens. All six alpha chains contain 22–26 natural interruptions of the Gly-X-Y repeats, spread throughout their central collagenous domain. These are presumably regions of specific function and/or ligand binding sequences, of significance to its structural role in the basement membrane. Although there are many possible combinations among the six alpha chains, only three are biologically compatible and found in basement membranes. These are composed of α1α1α2, α3α4α5, and α5α5α6. Type IV collagen participates in forming networks interacting with additional important components of the basement membranes, such as laminin and nidogen [23, 24]. As a component of the glomerular filtration barrier, along with the endothelial cells and the podocytes, basement membranes play a crucial role as a selective filter, based on molecular size and charge. A damage of the basement membrane or inherited defects such as mutations in type IV collagen lead to the abnormal passage of red blood cells in the urine.
Clinical signs, GBM histology, and genetics of X-linked Alport syndrome
X-linked Alport syndrome is one of the most severe inherited glomerulopathies, characterized by alternating thinning and thickening of the GBM as well as splitting and lamellation of the lamina densa. At a young age, affected hemizygote males and heterozygous female carriers may present initially with uniform thinning of the GBM, which in males progresses rapidly with age to a more severe thickened and lamelated picture accompanied by the onset of proteinuria, hypertension, and renal failure, usually reaching ESKD between adolescence and the third decade of life. About 82% of patients develop sensorineural hearing loss and about 44% develop ocular abnormalities [25].
Over the past two decades, after clinical and molecular investigation of hundreds of X-linked Alport cases, much experience has been accumulated regarding the important correlation of genotype to phenotype. Based on the age at onset of ESKD and the rate of clinical progression, two forms of X-linked Alport are usually recognized [26], the classical, well-recognized "juvenile" type and the "adult" type. In the former, ESKD ensues rapidly in men at about 20 years of age. In the "adult" type, the age at ESKD extends to the late 20s or even the 30s, 40s, and 50s, especially in patients inheriting some milder COL4A5 missense mutations (see below). In young adult males who carry milder missense mutations, areas of thickening and thinning may coexist or only thinning may be present, with or without splitting, making a definite histological diagnosis of Alport syndrome occasionally difficult. Many researchers have stressed this [8, 27–30]. One could point out that this clinical presentation resembles the one exemplified by some heterozygous carriers of mutations in the autosomal COL4A3/COL4A4 genes that suffer from TBMN and late onset proteinuria, CKD, and ESKD.
There are five studies, one in entire Europe with the European Community Alport Syndrome Concerted Action study (ECASCA) [10], and one each in Germany [26], Slovenia [7], China [31], and very recently in the USA [32], describing the whole spectrum of clinical phenotypes from over 500 COL4A5 mutations and confirm that the position and type of each mutation may dictate to a large extent the severity of Alport and how soon ESKD may ensue. Gross et al. (2002) [26] proposed the following classification of phenotypes of X-linked Alport patients: (a) type S (Severe), characterized by juvenile-onset ESKD (∼20 years of age), 80% incidence of hearing loss and 40% incidence of ocular lesions. This classical picture is caused by large rearrangements, premature stop, frameshift, donor splice site, and mutations in the NC1-domain (b) type MS (Moderate–Severe), including patients that progress to ESKD at age ∼26 and present lower frequencies of the extrarenal manifestations, implicating non-glycine missense mutations, glycine substitutions in exons 21–47, in-frame and acceptor splice site mutations, and (c) type M (Moderate), associated with glycine substitutions in exons 1–20 and characterized by late-onset ESKD (after the age of 30), 70% hearing loss, and less than 30% ocular lesions. Bekheirnia et al. (2010) [32], in a cohort of US patients with X-linked Alport, support the proposition of Gross et al. (2002) [26] that the most aggressive phenotypes are caused by truncating mutations, large and small deletions and splice mutations.
A prime example of a COL4A5 mutation that is associated with a mild hematuric phenotype is a substitution of glycine at position 624 by aspartate (G624D). This mutation probably represents a recurrently mutated position or it may be an example of a trans-national founder mutation. It was firstly described by Martin et al. (1998) [33] in a single family with a mild presentation and by Barker et al. (2001) [34] in a separate family. More recently, Slajpah et al. (2007) [7] reported mutation G624D in a total of 13 patients (nine females, four males) belonging to six small unrelated Slovenian kindreds. One family was diagnosed with adult-onset Alport based on EM findings and five were diagnosed as benign familial hematuria (BFH) until molecular genetics settled the diagnosis. They appear to be the first to propose that "adolescence ESKD and BFH may represent two opposite poles of the spectrum of hereditary COL4A5 nephropathies" [7], thus resembling the TBMN nephropathy resulting from COL4A3 and COL4A4 heterozygous mutations, confirmed recently in a large cohort from our center [15, 35].
We had a similar experience with two Greek families, one from Athens and one from Thessaloniki, who segregated this same mutation, G624D [36]. Male patients presented with late-onset renal failure, very likely a characteristic of this mutation. In family GR4209, a male patient reached ESKD at the age of 39 with sensorineural deafness. Another affected male showed hematuria and proteinuria accompanied by sensorineural deafness but his serum creatinine was normal at 1.03 mg/dl, at the age of 30. In the other family, GR4211, two brothers inherited the mutation. One reached ESKD at 50 years old without deafness, while his renal biopsy showed FSGS with uniform thinning of the GBM that included focal splitting. His two daughters have documented MH in their twenties. His brother is proteinuric with mildly reduced GFR and no deafness at 55 years old. The clinical and renal biopsy findings, including EM, in both families differ from classic, adolescence, and adult type X-linked Alport. Affected males developed ESKD late in life, after ages 39 to 50, or not at all, resembling the female carriers of X-linked COL4A5 nephropathy or the heterozygous carriers of mutations in COL4A3/COL4A4. In at least one renal biopsy that included EM there was TBMN and also FSGS [36].
Interestingly, we identified another similar COL4A5 mutation in two Cypriot families also associated with mild disease. This mutation, P628L in exon 25, is located very close to the G624D and affects a Y-position proline, which is substituted by leucine. This mutation also demonstrates a milder phenotypic expression. Among eight men carrying the mutation, five developed ESKD at ages 30, 34, 37, 45, and 57 years old. The 57-year-old patient also had diabetes. Another patient exhibited keratoconus. Three men had CKD of mild degree. Sensorineural deafness was found in a man with ESKD and in another with mild CKD who at the age of 48 maintains a serum creatinine of 2.5 mg/dl. His renal biopsy shows TBMN with FSGS. Six female carriers exhibit MH and two have additional non-nephrotic proteinuria. A recent biopsy of a 19-year-old female demonstrated TBMN in the presence of early FSGS. The progression to ESKD in the affected males is slow and delayed, very similar to patients carrying mutation G624D. Mutations G624D and P628L are very near the 12th natural interruption of the Gly-X-Y repeats in the COL4A5 chain, an observation that might offer an explanation for the associated milder phenotypes. Both mutations occurred on either side of a G1G natural interruption. Mutation G624D converts the G1G interruption into a G4G interruption, allowing the assumption that the destabilization of the collagen triple helix is not as dramatic as when a similar substitution occurs elsewhere in the collagenous domain. Similarly, mutation P628L represents a substitution of a hydroxyproline residue at the Y position of a tripeptide unit right after the G1G interruption. It can be hypothesized that some mutations, such as these near natural interruptions, do not disrupt drastically the zipper-like formation of the triple helix, which commences at the C-terminal end, or interfere less with the binding of putative ligands in the matrix milieu (Fig. 1) [36].

Schematic representation of the collagen IV triple helical molecule. The vertical lines along the triple helix represent the positions of the natural Gly-X-Y interruptions. Note that mutations G624D and P628L occurred near the 12th interruption of the α5 chain. Essentially, the G624D mutation converted the G1G interruption into a G4G one, while the P628L may affect the folding of the triple helix as it zippers from the C-terminal towards the N-terminal. Mutation F222C, substituting a cysteine for phenylalanine, occurred in the second natural interruption of a G4G type [38]
Along the same line, a recent case report described a male patient with a COL4A5 mutation that substitutes glycine with valine at amino acid residue 1000 (G1000V) [37]. The patient, aged 38, presented with only BFH, which segregated in the family. Based on all the above, one expects that many more similar families may exist worldwide remaining unnoticed, largely because older affected males with MH are not considered to result from X-linked COL4A5 mutations and are therefore not investigated accordingly. A careful consideration of the inheritance pattern by drawing a detailed pedigree can always help. A male-to-male transmission certainly excludes X-linked inheritance while a negative epidermal BM immunostaining for the α5 chain confirms X-linked AS. Unfortunately, a normal skin immunostaining does not exclude AS. A wider family history of sensorineural deafness and ocular abnormalities supports this diagnosis but cannot confirm it unequivocally, especially in smaller pedigrees [4]. In these, and many similar cases, the differential diagnosis based on clinical symptoms only will not resolve it and molecular investigation can be of great help.
On the opposite end, Becknell et al. [38] reported on a large American family with mutation F222C in the COL4A5 gene, where male patients presented with a novel severe glomerulopathy that rapidly progressed to ESKD at ages 10–22 years old. The mutation was within a G4G interruption of the collagenous domain, substituting a conserved phenylalanine residue, thereby attributing an unknown functional role. Interestingly, the authors emphasize the absence of typical AS clinical and biopsy findings. The symptoms included proteinuria and variable hematuria while the biopsy showed global and segmental glomerulosclerosis, mesangial hypercellularity and GBM immune complex deposition, quite unusual for AS. There were no typical Alport biopsy findings such as GBM alternate thinning and thickening nor any GBM splitting and lamellation (Fig. 1).
Finally, it should be mentioned that according to the recent report by Hanson et al. (2010) [9], even in the presence of an incomplete picture and only two diagnostic criteria for Alport syndrome, mutations can be found in the COL4A5 gene in up to 64% of the patients. This supports our hypothesis that patients with milder phenotypes might harbor such mutations and deserve molecular investigation.
Thin basement membrane nephropathy (TBMN) and phenotypic heterogeneity
The term TBMN has been used to describe the histological EM situation where the GBM demonstrates pure thinning of the GBM, compared to normal. The normal GBM thickness varies from 300–400 nm, and this variation is attributed to individual variability, age, gender, and the center performing the measurement. Until recently, TBMN was invariably considered to lead to familial BMH [8, 30], with a positive family history and no episodes of macroscopic hematuria. Ocular abnormalities, hearing loss and renal impairment were classically considered to be absent from the syndrome of BFH and long-term prognosis was deemed excellent. Universal thinning of the GBM is characteristic of the heterozygous carriers of COL4A3/COL4A4 mutations. In contrast, the much rarer homozygous or compound heterozygous of such mutations in the COL4A3/COL4A4 genes develop the classical autosomal recessive Alport syndrome course with early proteinuria and hypertension, reaching ESKD by late adolescence and the early 20s.
Since the first report by Lemmink et al. (1997) [39] that described the first COL4A4 mutation in a patient with TBMN, numerous publications supported the essential synonymy between TBMN due to heterozygous mutations in COL4A3/COL4A4 genes and BFH [7, 13, 40–49]. However, some previous investigations that had not attracted the proper attention had alerted to the fact that not all patients with heterozygous COL4A3/COL4A4 mutations would follow a benign course. Instead, they reported on patients who started off with TBMN on biopsy and MH and slowly progressed to proteinuria, hypertension, and chronic or ESKD [13, 50–54]. In some of those works, the authors invoked the association with another glomerulonephritis, such as IgAN, FSGS, minimal change disease, mesangioproliferative glomerulonephritis and others ([55] and references therein).
In 2007, we presented the largest series of patients with three founder heterozygous mutations in either the COL4A3 or the COL4A4 where a significant percentage had demonstrated the dual diagnosis of TBMN and FSGS, with progression to renal failure and ESKD. Specifically, those data along with additional unpublished results show that in our cohort of 180 Cypriot patients, nearly 50% proceed to CKD/ESKD while 13% of all develop ESKD, usually after 50 years old [15, 35, 56]. In detail, of 90 patients over 50 years old, 48 have CKD (53%), while 23 of the 48 have ESKD (23/90, a percentage of 25%) (Fig. 2, Table 1). These findings have recently been supported by another independent brief report [57], and certainly cast serious doubt on the commonly used term of "benign familial hematuria" with excellent prognosis. It is more than obvious nowadays that not all COL4A3/COL4A4 mutation carriers will enjoy a good prognosis for life and after the age of 30–40s. A closer follow-up is necessary in order to identify early enough those predisposed to adverse progression. Based on these findings and considering that a great many of our patients carry a common founder mutation, we hypothesize that modifier genes, perhaps in addition to unknown environmental factors, contribute to this inter- and intra-familial variability and unpleasant progression. It is worth mentioning that among the 180 patients in this TBMN cohort, 134 bear mutation G1334E, thereby minimizing genetic background variability ([15] and unpublished results).

Prevalence of symptoms amongst 180 TBMN mutation carriers, according to age. Under the age of 30, only microhematuria was encountered. After the age of 30, proteinuria complicated by CKD and ESKD developed in a significant degree (updated from [15], used with permission)
It is evident that familial hematuria encompasses a wide spectrum of COL4 mutations, affecting the α3, α4, and α5 chains and a renal biopsy with molecular genetic analysis are always important to establish and define accurately the underlying pathophysiology. Once the molecular diagnosis is confirmed in a pedigree, molecular genetics and DNA testing may avert the need for further renal biopsies in affected relatives. Above all, however, it is the realization that truly long-term follow-up with regular check-ups is necessary to ensure that the patient receives the best possible care. The appearance of only low-grade proteinuria is not a comforting sign and it is a warning that progression to a more severe phenotype, affecting renal function, may follow.
CFHR5 nephropathy/Isolated C3 glomerulonephritis
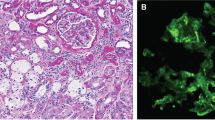
A recent genetic discovery in familial hematuria has been the description of heritable C3 glomerulonephritis as a result of mutations in the CFHR5 gene (CFHR5 nephropathy), by a large collaborative effort [16]. The CFHR5 gene belongs to a family of five genes (CFHR 1–5) clustered on chromosome 1q32, encoding for proteins that take part in the alternative complement pathway regulation. Complement factor H (CFH) and CFH-related proteins 1–5 share a subset of homologous domains, about 60 amino acids long, the sequence consensus repeats. CFHR5 binds C3b and it has been localized at the glomerular deposits of patients with glomerulonephritis, demonstrating a deposition pattern similar to C3 [58, 59].
This new hereditary form of MH had been described before but its hereditary nature and pathophysiological connection to the complement alternate pathway system had not been recognized [60–62]. Similarly, as regards its histology, mesangial C3 glomerulopathy has been known at least since 1980 from published reports in Europe and Japan, while more recently, loss-of-function mutations in important regulatory proteins such as CFH, complement factor I and membrane cofactor protein, have been detected in patients with inherited nephropathies characterized by isolated C3 mesangial deposits [63–68]. As the pathological pattern of glomerular inflammation is associated with dysregulation of the alternative complement pathway, there is no requirement for antibody-antigen complex to start the activation of C3 cascade and essentially no immunoglobulins are detected in the damaged glomerulus.
CFHR5 nephropathy is an autosomal dominant disease and is clinically characterized by continuous MH while some 25% of the patients also present with synpharyngitic macroscopic hematuria in childhood and adolescence associated with infection and pyrexia. Based on a recent description of a large patient cohort, in addition to hematuria, 80% of patients, particularly males, develop proteinuria, hypertension and chronic or ESKD, a progression that seems to start slightly earlier than in TBMN patients and follows a faster course [16, 17]. The main finding in 17 available renal biopsies was mild increase in mesangial matrix and cells, with isolated C3 deposits in the mesangium and the sub-endothelial area, and no immunoglobulin deposition. GBMs were of normal thickness.
Until the end of 2010, we screened genetically 163 at-risk subjects from 16 affected Cypriot families. Of these, 105 (64%) carry a common mutation, a duplication of exons 2–3 [16]. Of these 105 mutation carriers (MC), nine subjects (8.5%) at various ages (12–88 years old) have as of yet no urinary abnormalities, a clear indication of reduced penetrance. The great majority (62 patients, or 59%), only show MH, while 34 patients have developed additional proteinuria. Of these 34 proteinuric patients, 30 have gone on to develop renal failure and 18 have reached ESKD. Of great interest is the striking gender difference, because 15 of the 18 patients with ESKD are males (83%) and only three are females (17%) (Fig. 3, Table 2). Eleven patients received 13 renal transplants with excellent survival between 1 and 23 years.

Prevalence of symptoms among 100 CFHR5 mutation carriers, according to age. Under the age of 30, only microhematuria was encountered. After the age of 30, proteinuria complicated by CKD and ESKD developed in a significant degree (especially in males) (updated from [17], used with permission)
It is of great interest that nearly all male patients who have reached ESKD have exhibited in childhood and adolescence additional episodes of macroscopic hematuria after infections of the URTI. The clinical picture at the time is very similar to IgA nephropathy, a fact that on several occasions caused debate as to whether the renal biopsy had actually failed to demonstrate the anticipated IgG/IgA deposits. In one affected family in particular, where a daughter first exhibited episodes of macroscopic hematuria following a URTI, no renal biopsy was carried out, and a report was sent to the referring physician describing it as a classical case of IgG/IgA Berger’s disease. The situation became more complex when her younger brother, 9 years later, also developed episodes of macroscopic hematuria at 19 years old, associated with a URTI. The diagnosis of probable familial Berger’s disease changed to CFHR5 nephropathy when the molecular test in 2009 proved positive. Their father carried the CFHR5 mutation and had MH that he was not aware of. It is also likely that some cases that initially are thought to have TBMN, without a biopsy, and test negative for COL4A3/COL4A4 mutations, actually may turn out to have C3 nephropathy. We had one such family in our cohort.
It is of interest that so far all patients described are of Greek-Cypriot origin and they all carry the same founder mutation, a duplication of CFHR5 exons 2–3 [16, 17]. This facilitates tremendously the diagnosis by a simple polymerase chain reaction amplification test, thereby also obviating the need for a renal biopsy to other family members who present with suspicious similar symptoms. One anticipates that since the histological changes of pure C3 nephropathy have been described in patients from several countries all over the world, the Greek-Cypriot mutation or other similar CFHR5 mutations will be discovered in these patients in the next few years. To date, however, the prevalence of this disease in populations outside Cyprus is unknown.
Conclusions
Pure familial MH in early childhood cannot distinguish between the Alport syndrome, either X-linked or autosomal recessive, the TBMN phenotype, the CFHR5 nephropathy and the several other, yet unknown causes of familial hematuria. A detailed family history is essential, looking particularly at (a) the pattern of inheritance, (b) the age at which other family members developed proteinuria, CKD, and ESKD, and (c) the presence of sensorineural deafness and/or ocular defects. Investigations should start with the usual tests for kidney function, urine analysis for additional proteinuria, and molecular genetics aimed at identifying either a COL4, or CFHR5 gene mutation. These investigations should be extended to the parents, siblings, and more distant relatives. In our opinion, in established familial cases, an early renal biopsy including EM is always useful and desirable and should be encouraged in at least one affected family member with MH. In addition to the histological evaluation, a kidney biopsy may direct the line of molecular investigations, in view of the genetic heterogeneity underlining familial MH. A successful molecular diagnosis reduces or abolishes the need for additional diagnostic biopsies. Unfortunately, there is no consensus among nephrologists regarding the need of an early renal biopsy in patients with familial hematuria. Some are advocates of a biopsy even in the presence of isolated continuous MH while others are opposed to it until proteinuria develops [69–71]. In a relevant algorithm by Kashtan [4], a kidney biopsy is recommended before molecular testing and after a α5(IV) positive skin biopsy.
As regards the limitations of the biopsy, it is emphasized by Haas (2009) [8] that EM alone cannot distinguish between TBMN, the heterozygous carrier state of XLAS, autosomal recessive Alport syndrome and early stages of XLAS. This is where the molecular approach can prove instrumental in the differential diagnosis, and especially so when previous studies have established the affected haplotype or the responsible germinal mutation. It is worth emphasizing that in cases where familial hematuria is diagnosed and a mutation is found, the first and easiest non-invasive investigative test for the next patient who comes down with additional proteinuria or other relevant symptoms should be a molecular analysis to confirm or exclude the familial condition. An algorithm for the series of molecular tests based on present-day knowledge of the genetics of familial hematuria is proposed in Fig. 4.

Algorithm for molecular testing of patients belonging to families segregating glomerular microscopic hematuria. A kidney or a skin biopsy may be performed before or after the molecular analysis depending on the clinical status or disease progression of the patient, for histological evaluation. An early biopsy may also help direct molecular testing. In most, but certainly not all, families where a diagnosis has been established by molecular means, a simple molecular testing of the subject under study, for detecting the responsible affected haplotype or germinal mutation, might be adequate. A molecular diagnosis will acquire a superb position in CFHR5 and collagen IV nephropathies diagnosis and treatment if early intervention proves decisive for disease prevention
Correct family counseling, excellent medical care, and good long-term follow-up are top priorities. Classical adolescent Alport syndrome or Alport syndrome reaching ESKD later in the late 30s is now well known and accepted, but it is important to emphasize the accumulating evidence according to which single amino acid substitutions in the COL4A5 gene, such as the G624D and P628L, may not always lead to early renal failure. Instead, a mild hematuric syndrome may persist late in life with minimal proteinuria and renal impairment. Clinicians should be aware that a subset of patients with familial hematuria, thin membranes, and late-onset ESKD may also be explained by COL4A5 mutations. This X-linked disease status may not satisfy the classical Alport syndrome clinical diagnosis but rather an X-linked TBMN diagnosis. It is presently unknown how widespread this is but several reports already have introduced this notion [7, 36, 37].
Available evidence since the original work by Lemmink et al. (1996) [39] indicates that most patients with microhematuria and TBMN result from heterozygous COL4A3/COL4A4 mutations and the first 3–4 decades of life are indeed characterized by pure ΜΗ alone. From then on, however, some 50% of these patients will follow a different course, progressing into proteinuria and CKD. Recent data on a large Cypriot cohort [15] confirm that not all TBMN cases will follow a benign course and regular annual check ups, to include tests for proteinuria should alert patients and physicians to the possibility of progression into CKD and eventually ESKD. A renal biopsy should be seriously considered at this stage and appropriate measures such as statins, ACE inhibitors, and possibly cyclosporin should be entertained to arrest the evolution of the disease. It is fair to say that apart from the large patient cohort from Cyprus, in several reports by other investigators, the majority of TBMN patients follow a benign course. There might be genetic and/or environmental factors to explain these disparate findings and hopefully future work and longer follow-up in other populations in view of our results, will enlighten this issue and provide the correct answers.
The list of causes of familial MH is still incomplete and good family studies, careful renal biopsies and molecular genetics are needed to solve the puzzle of the remaining causes of familial hematurias. In this respect, the identification of the CFHR5 mutation is a recent development that provides an insight into a histological finding known but not understood for over 40 years. At the same time, it provides possibilities for more specific and efficient therapies for patients who were programmed to end in ESKD. This advance also opens up possibilities for more research in the CFHR5 gene, the alternate complement pathway and the entire complement system which may be associated with other forms of isolated C3 glomerulonephritis, atypical hemolytic uremic syndrome, dense deposit disease and other forms of yet unknown familial GN [72].
References
Fogazzi GB, Edefonti A, Garigali G, Giani M, Zolin A, Raimondi S, Mihatsch MJ, Messa P (2008) Urine erythrocyte morphology in patients with microscopic haematuria caused by a glomerulopathy. Pediatr Nephrol 23:1093–1100
Heath KE, Campos-Barros A, Toren A, Rozenfeld-Granot G, Carlsson LE, Savige J, Denison JC, Gregory MC, White JG, Barker DF, Greinacher A, Epstein CJ, Glucksman MJ, Martignetti JA (2001) Nonmuscle myosin heavy chain IIA mutations define a spectrum of autosomal dominant macrothrombocytopenias: May-Hegglin anomaly and Fechtner, Sebastian, Epstein, and Alport-like syndromes. Am J Hum Genet 69:1033–1045
Seri M, Pecci A, Di Bari F, Cusano R, Savino M, Panza E, Nigro A, Noris P, Gangarossa S, Rocca B, Gresele P, Bizzaro N, Malatesta P, Koivisto PA, Longo I, Musso R, Pecoraro C, Iolascon A, Magrini U, Rodriguez Soriano J, Renieri A, Ghiggeri GM, Ravazzolo R, Balduini CL, Savoia A (2003) MYH9-related disease: May-Hegglin anomaly, Sebastian syndrome, Fechtner syndrome, and Epstein syndrome are not distinct entities but represent a variable expression of a single illness. Medicine (Baltimore) 82:203–215
Kashtan CE (2009) Familial hematuria. Pediatr Nephrol 24:1951–1958
Alport AC (1927) Hereditary familial congenital haemorrgagic nephritis. BMJ 1:504–506
Kashtan CE (2005) Familial hematurias: what we know and what we don’t. Pediatr Nephrol 20:1027–1035
Slajpah M, Gorinsek B, Berginc G, Vizjak A, Ferluga D, Hvala A, Meglic A, Jaksa I, Furlan P, Gregoric A, Kaplan-Pavlovcic S, Ravnik-Glavac M, Glavac D (2007) Sixteen novel mutations identified in COL4A3, COL4A4, and COL4A5 genes in Slovenian families with Alport syndrome and benign familial hematuria. Kidney Int 71:1287–1295
Haas M (2009) Alport syndrome and thin glomerular basement nephropathy: a practical approach to diagnosis. Arch Pathol Lab Med 133:224–232
Hanson H, Storey H, Pagan J, Flinter F (2011) The value of clinical criteria in identifying patients with X-linked Alport syndrome. Clin J Am Soc Nephrol 6:198–203
Jais JP, Knebelmann B, Giatras I, De Marchi M, Rizzoni G, Renieri A, Weber M, Gross O, Netzer KO, Flinter F, Pirson Y, Dahan K, Wieslander J, Persson U, Tryggvason K, Martin P, Hertz JM, Schröder C, Sanak M, Carvalho MF, Saus J, Antignac C, Smeets H, Gubler MC (2003) X-linked Alport syndrome: natural history and genotype-phenotype correlations in girls and women belonging to 195 families: a "European Community Alport Syndrome Concerted Action" study. J Am Soc Nephrol 14:2603–2610
Kashtan CE (2007) Alport syndrome and the X chromosome: implications of a diagnosis of Alport syndrome in females. Nephrol Dial Transplant 22:1499–1505
Longo I, Scala E, Mari F, Caselli R, Pescucci C, Mencarelli MA, Speciale C, Giani M, Bresin E, Caringella DA, Borochowitz ZU, Siriwardena K, Winship I, Renieri A, Meloni I (2006) Autosomal recessive Alport syndrome: an in-depth clinical and molecular analysis of five families. Nephrol Dial Transplant 21:665–671
Longo I, Porcedda P, Mari F, Giachino D, Meloni I, Deplano C, Brusco A, Bosio M, Massella L, Lavoratti G, Roccatello D, Frasca G, Mazzucco G, Muda AO, Conti M, Fasciolo F, Arrondel C, Heidet L, Renieri A, De Marchi M (2002) COL4A3/COL4A4 mutations: from benign familial hematuria to autosomal dominant or recessive Alport syndrome. Kidney Int 61:1947–1956
Savige J, Rana K, Tonna S, Buzza M, Dagher H, Wang YY (2003) Thin basement membrane nephropathy. Kidney Int 64:1169–1178
Pierides A, Voskarides K, Athanasiou Y, Ioannou K, Damianou L, Arsali M, Zavros M, Pierides M, Vargemezis V, Patsias C, Zouvani I, Kyriacou K, Deltas C (2009) Clinico-pathological correlations in 127 patients in 11 large pedigrees, segregating one of three heterozygous mutations in the COL4A3/ COL4A4 genes associated with familial haematuria and significant late progression to proteinuria and chronic kidney disease from focal segmental glomerulosclerosis. Nephrol Dial Transplant 24:2721–2729
Gale DP, de Jorge EG, Cook HT, Martinez-Barricarte R, Hadjisavvas A, Adam G, McLean AG, Pusey CD, Pierides A, Kyriacou K, Athanasiou Y, Voskarides C, Deltas C, Palmer A, Frémeaux-Bacchi V, Cordoba SR, Maxwell PH, Pickering MC (2010) Complement factor H-related protein 5 (CFHR5) nephropathy: an endemic cause of renal disease in Cyprus. Lancet 376:794–801
Athanasiou Y, Voskarides K, Gale D, Damianou L, Patsias C, Zavros M, Maxwell P, Cook T, Demosthenous P, Hatjisavvas A, Kyriacou K, Zouvani I, Pierides M, Deltas C (2011) Familial C3 glomerulopathy associated with CFHR5 mutations: clinical characteristics of 91 patients in 16 pedigrees. Clin J Am Soc Nephrol. Clin J Am Soc Nephrol 6:1436–1446
Paterson AD, Liu XQ, Wang K, Magistroni R, Song X, Kappel J, Klassen J, Cattran D, St George-Hyslop P, Pei Y (2007) Genome-wide linkage scan of a large family with IgA nephropathy localizes a novel susceptibility locus to chromosome 2q36. J Am Soc Nephrol 18:2408–2415
Gharavi AG, Kiryluk K, Choi M, Li Y, Hou P, Xie J, Sanna-Cherchi S, Men CJ, Julian BA, Wyatt RJ, Novak J, He JC, Wang H, Lv J, Zhu L, Wang W, Wang Z, Yasuno K, Gunel M, Mane S, Umlauf S, Tikhonova I, Beerman I, Savoldi S, Magistroni R, Ghiggeri GM, Bodria M, Lugani F, Ravani P, Ponticelli C, Allegri L, Boscutti G, Frasca G, Amore A, Peruzzi L, Coppo R, Izzi C, Viola BF, Prati E, Salvadori M, Mignani R, Gesualdo L, Bertinetto F, Mesiano P, Amoroso A, Scolari F, Chen N, Zhang H, Lifton RP (2011) Genome-wide association study identifies susceptibility loci for IgA nephropathy. Nat Genet 43:321–327
Coppo R, Gianoglio B, Porcellini MG, Maringhini S (1998) Frequency of renal diseases and clinical indications for renal biopsy in children (report of the Italian National Registry of Renal Biopsies in Children). Group of Renal Immunopathology of the Italian Society of Pediatric Nephrology and Group of Renal Immunopathology of the Italian Society of Nephrology. Nephrol Dial Transplant 13:293–297
Mochizuki T, Lemmink HH, Mariyama M, Antignac C, Gubler MC, Pirson Y, Verellen-Dumoulin C, Chan B, Schröder CH, Smeets HJ, Reeders ST (1994) Identification of mutations in the α3(IV) and α4(IV) collagen genes in autosomal recessive Alport syndrome. Nat Genet 8:77–81
Hudson BG, Tryggvason K, Sundaramoorthy M, Neilson EG (2003) Alport’s syndrome, Goodpasture’s syndrome, and type IV collagen. N Engl J Med 348:2543–2556
LeBleu VS, Macdonald B, Kalluri R (2007) Structure and function of basement membranes. Exp Biol Med (Maywood) 232:1121–1129
Khoshnoodi J, Pedchenko V, Hudson BG (2008) Mammalian collagen IV. Microsc Res Tech 71:357–1370
Jais JP, Knebelmann B, Giatras I, De Marchi M, Rizzoni G, Renieri A, Weber M, Gross O, Netzer KO, Flinter F, Pirson Y, Verellen C, Wieslander J, Persson U, Tryggvason K, Martin P, Hertz JM, Schröder C, Sanak M, Krejcova S, Carvalho MF, Saus J, Antignac C, Smeets H, Gubler MC (2000) X-Linked Alport syndrome: natural history in 195 families and genotype–phenotype correlations in males. J Am Soc Nephrol 11:649–657
Gross O, Netzer KO, Lambrecht R, Seibold S, Weber M (2002) Meta-analysis of genotype-phenotype correlation in X-linked Alport syndrome: impact on clinical counseling. Nephrol Dial Transplant 17:1218–1227
Habib R, Gubler MC, Hinglais N, Noel LH, Droz D, Levy M, Mahieu P, Foidart JM, Perrin D, Bois E, Grunfeld JP (1982) Alport syndrome: experience at Hôpital Necker. Kidney Int 11:S20–S28
Cangiotti AM, Sessa A, Meroni M, Montironi R, Ragaiolo M, Mambelli M, Cinti S (1996) Evolution of glomerular basement membrane lesions in a male patient with Alport syndrome: ultrastructural and morphometric study. Nephrol Dial Transplant 11:1829–1834
Moghal NE, Milford DV, White RHR, Raafat F, Higgins R (1999) Coexistence of thin membrane and Alport nephropathies in families with hematuria. Pediatr Nephrol 13:778–781
Thorner PS (2007) Alport syndrome and thin basement membrane nephropathy. Nephron Clin Pract 106:82–88
Wei G, Zhihong L, Huiping C, Caihong Z, Zhaohong C, Leishi L (2006) Spectrum of clinical features and type IV collagen alpha-chain distribution in Chinese patients with Alport syndrome. Nephrol Dial Transplant 21:3146–3154
Bekheirnia MR, Reed B, Gregory MC, McFann K, Shamshirsaz AA, Masoumi A, Schrier RW (2010) Genotype-phenotype correlation in X-linked Alport syndrome. J Am Soc Nephrol 21:876–883
Martin P, Heiskari N, Zhou J, Leinonen A, Tumelius T, Hertz JM, Barker D, Gregory M, Atkin C, Styrkarsdottir U, Neumann H, Springate J, Shows T, Pettersson E, Tryggvason K (1998) High mutation detection rate in the COL4A5 collagen gene in suspected Alport syndrome using PCR and direct DNA sequencing. J Am Soc Nephrol 9:2291–2301
Barker DF, Denison JC, Atkin CL, Gregory MC (2001) Efficient detection of Alport syndrome COL4A5 mutations with multiplex genomic PCR-SSCP. Am J Med Genet 98:148–160
Voskarides K, Damianou L, Neocleous V, Zouvani I, Christodoulidou S, Hadjiconstantinou V, Ioannou K, Athanasiou Y, Patsias C, Alexopoulos E, Pierides A, Kyriacou K, Deltas C (2007) COL4A3/COL4A4 mutations producing focal segmental glomerulosclerosis and renal failure in thin basement membrane nephropathy. J Am Soc Nephrol 18:3004–3016
Demosthenous P, Voskarides K, Stylianou K, Hadjigavriel M, Arsali M, Patsias C, Georgaki E, Zirogiannis P, Stavrou C, Daphnis E, Pierides A, Deltas C, the Hellenic Nephrogenetics Research Consortium (2011) X-linked Alport syndrome in Hellenic families: phenotypic heterogeneity and mutations near interruptions of the collagen domain in COL4A5. Clin Genet. doi:10.1111/j.1399-0004.2011.01647.x
Kaneko K, Tanaka S, Hasui M, Nozu K, Krol RP, Iijima K, Sugimoto K, Takemura T (2010) A family with X-linked benign familial hematuria. Pediatr Nephrol 25:545–548
Becknell B, Zender GA, Houston R, Baker PB, McBride KL, Luo W, Hains DS, Borza DB, Schwaderer AL (2011) Novel X-linked glomerulopathy is associated with a COL4A5 missense mutation in a non-collagenous interruption. Kidney Int 79:120–127
Lemmink HH, Nillesen WN, Mochizuki T, Schroder CH, Brunner HG, van Oost BA, Monnens LA, Smeets HJ (1996) Benign familial. hematuria due to mutation of the type IV collagen α4 gene. J Clin Invest 98:1114–1118
Buzza M, Dagher H, Wang YY, Wilson D, Babon JJ, Cotton RG, Savige J (2001) COL4A4 mutation in thin basement membrane disease previously described in Alport syndrome. Kidney Int 60:480–483
Ozen S, Ertoy D, Heidet L, Cohen-Solal L, Ozen H, Besbas N, Bakkaoglu A, Antignac C (2001) Benign familial hematuria associated with a novel COL4A4 mutation. Pediatr Nephrol 16:874–877
Badenas C, Praga M, Tazon B, Heidet L, Arrondel C, Armengol A, Andrés A, Morales E, Camacho JA, Lens X, Dávila S, Milà M, Antignac C, Darnell A, Torra R (2002) Mutations in the COL4A4 and COL4A3 genes cause familial benign hematuria. J Am Soc Nephrol 13:1248–1254
Buzza M, Dagher H, Wang YY, Wilson D, Babon JJ, Cotton RG, Savige J (2003) Mutations in the COL4A4 gene in thin basement membrane disease. Kidney Int 63:447–453
Gross O, Netzer KO, Lambrecht R, Seibold S, Weber M (2003) Novel COL4A4 splice defect and in-frame deletion in a large consanguine family as a genetic link between benign familial haematuria and autosomal Alport syndrome. Nephrol Dial Transplant 18:1122–1127
Tazon Vega B, Badenas C, Ars E, Lens X, Mila M, Darnell A, Torra R (2003) Autosomal recessive Alport’s syndrome and benign familial hematuria are collagen type IV diseases. Am J Kidney Dis 42:952–959
Wang YY, Rana K, Tonna S, Llin T, Sin L, Savige J (2004) COL4A3 mutations and their clinical consequences in thin basement membrane nephropathy (TBMN). Kidney Int 65:786–790
Rana K, Tonna S, Wang YY, Sin L, Lin T, Shaw E, Mookerjee I, Savige J (2007) Nine novel COL4A3 and COL4A4 mutations and polymorphisms identified in inherited membrane diseases. Pediatr Nephrol 22:652–657
Baek JI, Choi SJ, Park SH, Choi JY, Kim CD, Kim YL, Kim UK (2009) Identification of novel variants in the COL4A4 gene in Korean patients with thin basement membrane nephropathy. Indian J Med Res 129:525–533
Endreffy E, Ondrik Z, Iványi B, Maróti Z, Bereczki C, Haszon I, Györke Z, Worum E, Németh K, Rikker C, Ökrös Z, Túri S (2011) Collagen type IV nephropathy: genetic heterogeneity examinations in affected Hungarian families. Mol Cell Probes 25:28–34
Nieuwhof CMG, de Heer F, de Leeuw P, van Breda Vriesman PJC (1997) Thin GBM nephropathy: premature glomerular obsolescence is associated with hypertension and late onset renal failure. Kidney Int 51:1596–1601
Nogueira M, Cartwright J Jr, Horn K, Doe N, Shappell S, Barrios R, Coroneos E, Truong LD (2000) Thin basement membrane disease with heavy proteinuria or nephrotic syndrome at presentation. Am J Kidney Dis 35:E15
van Paasen P, van Breda Vriesman PJC, van Rie H, Tervaert JWC (2004) Signs and symptoms of thin basement membrane nephropathy: a prospective regional study on primary glomerular disease – The Limburg Renal Registry. Kidney Int 66:909–913
Norby SM, Cosio FG (2005) Thin basement membrane nephropathy associated with other glomerular diseases. Semin Nephrol 25:176–179
Haas M (2006) Thin glomerular basement membrane nephropathy: incidence in 3471 consecutive renal biopsies examined by electron microscopy. Arch Pathol Lab Med 130:699–706
Gregory MC (2005) The clinical features of thin basement membrane nephropathy. Semin Nephrol 25:140–145
Deltas C (2009) Thin basement membrane nephropathy: is there genetic predisposition to more severe disease? Pediatr Nephrol 24:877–879
Hoefele J, Lange-Sperandio B, Ruessmann D, Glöckner-Pagel J, Alberer M, Benz MR, Nagel M, Weber LT (2010) Novel heterozygous COL4A3 mutation in a family with late-onset ESKD. Pediatr Nephrol 25:1539–1542
McRae JL, Cowan PJ, Power DA, Mitchelhill KI, Kemp BE, Morgan BP, Murphy BF (2001) Human factor H-related protein 5 (FHR-5) A new complement-associated protein. J Biol Chem 276:6747–6754
Murphy B, Georgiou T, Machet D, Hill P, McRae J (2002) Factor H-related protein-5: a novel component of human glomerular immune deposits. Am J Kidney Dis 39:24–27
Sirbat D, Saudax E, Hurault de Ligny B, Bene MC, Raspiller A (1983) A new etiology of episcleritis: nephropathies with IgA and/or isolated C3 deposits. J Fr Ophthalmol 6:921–925
Grekas D, Morley AR, Wilkinson R, Kerr DNS (1984) Isolated C3 deposition in patients without systemic disease. Clin Nephrol 21:270–274
Manno C, Proscia AR, Laraia E, Gianarande M, Di Cario M, Salvatore C, Tasc A, Schena FP, Rita S (1990) Clinicopathological features in patients with isolated C3 mesangial proliferative glomerulonephritis. Nephrol Dial Transplant 5(s):78–80
Gallego N, Teruel JL, Mampaso F, Gonzalo A, Ortuno J (1991) Acute interstitial nephritis superimposed on glomerulonephritis: report of a case. Pediatr Nephrol 5:229–231
Calls Ginesta J, Almirall J, Torras A, Darnell A, Revert L (1995) Long-term evolution of patients with isolated C3 mesangial glomerulonephritis. Clin Nephrol 43:221–225
Yagi K, Yanagida H, Sugimoto K, Kuwajima H, Tabata N, Morita K, Okada M, Takemura T (2005) Clinicopathologic features, outcome and therapeutic interventions in four children with glomerulonephritis. Pediatr Nephrol 20:1273–1278
Abrera-Abeleda MA, Nishimura C, Smith JLH, Sethi S, McRae JL, Murphy BF, Silvestri G, Skerka C, Jozsi M, Zipfel PF, Hageman GS, Smith RJH (2006) Variations in the complement regulatory genes factor H (CFH) and factor H related 5 (CFHR5) are associated with membranoproliferative glomerulonephritis type II (dense deposit disease). J Med Genet 43:582–589
Servais A, Fremeaux-Bacchi V, Lequintrec M, Salomon R, Blouin J, Knebelmann B, Grunfeld J-P, Lesavre P, Noel L-H, Fakhouri F (2007) Primary glomerulonephritis with isolated C3 deposits: a new entity which shares common genetic risk factors with haemolytic uraemic syndrome. J Med Genet 44:193–199
Habbig S, Mihatsch MJ, Heinen S, Beck B, Emmel M, Skerka Ch, Kirschfink M, Hoppe B, Zipfel PF, Licht Ch (2009) C3 deposition glomerulopathy due to a functional factor H defect. Kidney Int 75:1230–1234
Kim BS, Kim YK, Shin YS, Kim YO, Song HC, Kim YS, Choi EJ (2009) Natural history and renal pathology in patients with isolated microscopic hematuria. Korean J Intern Med 24:356–361
Fuiano G, Mazza G, Comi N, Caglioti A, De Nicola L, Iodice C, Andreucci M, Andreucci VE (2000) Current indications for renal biopsy: a questionnaire-based survey. Am J Kidney Dis 35:448–457
Parone DB, Meyer LE (1981) The effect of biopsy on therapy in renal disease. Arch Intern Med 141:1039–1041
Maga TK, Nishimura CJ, Weaver AE, Frees KL, Smith RJ (2010) Mutations in alternative pathway complement proteins in American patients with atypical hemolytic uremic syndrome. Hum Mutat 31:E1445–E1460
Acknowledgements
The authors thank the patients and relatives who participated in the numerous studies that made this research possible. This work was supported by the Medical and Public Health Services of the Cyprus Ministry of Health and by grants from the Cyprus Research Promotion Foundation ΠΕΝΕΚ ΕΝΙΣΧ/0505/02, ΠΕΝΕΚ/ΕΝΙΣΧ/0308/08, NEW INFRASTRUCTURE/STRATEGIC/0308/24, and through the University of Cyprus Articles 3/311 and 3/346 to CD.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Deltas, C., Pierides, A. & Voskarides, K. The role of molecular genetics in diagnosing familial hematuria(s). Pediatr Nephrol 27, 1221–1231 (2012). https://doi.org/10.1007/s00467-011-1935-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-011-1935-5