
Abstract
Background
The optimal technique to cure strangulated inguinal hernia remains controversial. The use of mesh in cases of strangulated hernia is still debated due to the potential risk of infection.
Objective
This systematic review aimed to determine whether or not the mesh repair technique is associated with a higher risk of surgical site infection than non-mesh techniques for strangulated inguinal hernias in adults.
Methods
An electronic search of the relevant literature was performed on 15 December 2012 using the following databases: MEDLINE, the Cochrane Library, Scopus, Embase, and the Web of Science. Articles reporting a comparison between the mesh repair technique and a non-mesh technique to treat strangulated inguinal hernias in adults, and published in the English or French language in a peer-reviewed journal, were considered for analysis. The quality of randomized controlled trials (RCTs) was assessed using the Jadad scoring system. To assess the quality of non-randomized trials, we used the Methodological Index for Non-Randomized Studies (MINORS).
Results
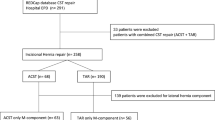
A total of 232 papers was found in the initial search; nine were included in the meta-analysis. The wound infection rate in the mesh repair technique group was lower than in the control group, with a trend towards significance (odds ratio [OR] 0.46, 95 % confidence interval [CI] 0.20–1.07; p = 0.07). The hernia recurrence rate was lower in the mesh repair group (OR 0.2, 95 % CI 0.05–0.78; p = 0.02).
Conclusion
The mesh repair technique is a good option for the treatment of strangulated inguinal hernias in adults, giving an acceptable wound infection rate and fewer recurrences than non-mesh repair. Our study does not allow us to recommend the use of mesh in cases of bowel resection. We emphasize that, except the two RCTs, the results are predicated on patient selection bias by careful surgeons. Further RCTs are required to obtain more powerful evidence-based data.









Similar content being viewed by others


References
Li J, Ji Z, Li Y (2014) Comparison of laparoscopic versus open procedure in the treatment of recurrent inguinal hernia: a meta-analysis of the results. Am J Surg 207(4):602–612
Karatepe O, Adas G, Battal M et al (2011) The comparison of preperitoneal and Lichtenstein repair for incarcerated groin hernias: a randomised controlled trial. Int J Surg 6:189–192
Papaziogas B, Lazaridis C, Makris J et al (2005) Tension-free repair versus modified Bassini technique (Andrews technique) for strangulated inguinal hernia: a comparative study. Hernia 9:156–159
Simons MP, Aufenacker T, Bay-Nilsen M et al (2009) European hernia society guidelines on the treatment of inguinal hernia in adult patients. Hernia 13:343–403
Nieuwenhuizen J, Van Ramshorst GH, Ten Brinke JG et al (2011) The use of mesh in acute hernia: frequency and outcome in 99 cases. Hernia 15:297–300
Derici H, Unalp H, Nazli O et al (2010) Prosthetic repair of incarcerated inguinal hernias: is it a reliable method? Langenbecks Arch Surg 395:575–579
Atila K, Guler S, Inal A (2010) Prosthetic repair of acutely incarcerated groin hernias: a prospective clinical observational cohort study. Langenbecks Arch Surg 395:563–568
Amid PK, Shulman AG, Lichtenstein IL (1996) Open “tension free” repair of inguinal hernias: the Lichtenstein technique. Eur J Surg 162(6):447–453
Pélissier E, Palot JP, Ngo P (2007) Traitement chirurgical des hernies inguinales par voie inguinale. In: Encycl Med Chir. (Elsevier Masson, Paris), Techniques chirurgicales - Appareil digestif, 40–110, p.16
Beattle AD (1963) Inguinal hernia repair: analysis of personal series of 481 cases carried out by modified Bassini technic. Ann Surg 157:244–253
Glassow F (1996) The Shouldice hospital technique. Int Surg 71:148–153
Taylor SG, O’Dwier PG (1999) Chronic groin sepsis following tension-free inguinal hernioplasty. Br J Surg 86:562–565
Jadad AR, Moore RA, Caroll D et al (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 17:1–12
Slim K, Nini E, Forestier D et al (2003) Methodological Index for Non-Randomized Studies (minors): development and validation of new instrument. ANZ J Surg 73:712–716
Topcu O, Kurt A, Soylu S et al (2013) Polypropylene mesh repair of incarcerated and strangulated hernias: a prospective clinical study. Surg Today 43:1140–1144
Elsebae MMA, Nasr M, Said M (2008) Tension-free repair versus Bassini technique for strangulated inguinal hernia: a controlled randomized study. Int J Surg 6:302–305
Bessa SS, Katri KM, Abdel-Salam WN et al (2007) Early results from the use of the Lichtenstein repair in the management of strangulated groin hernia. Hernia 11:239–242
Wysocki A, Kulawik J, Poźniczek M et al (2006) Is the Lichtenstein operation of strangulated groin hernia a safe procedure? World J Surg 30:2065–2070. doi:10.1007/s00268-005-0416-z
Videhult P, Magnusson J, Thorell A (2009) Low wound infection risk when using surgical meshes in incarcerated inguinal hernia. Meta-analysis of seven prospective studies with 311 patients. Lakartidningen 106:2218–2220
Conflict of interest
The authors declared no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hentati, H., Dougaz, W. & Dziri, C. Mesh Repair Versus Non-Mesh Repair for Strangulated Inguinal Hernia: Systematic Review with Meta-Analysis. World J Surg 38, 2784–2790 (2014). https://doi.org/10.1007/s00268-014-2710-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-014-2710-0