
Abstract
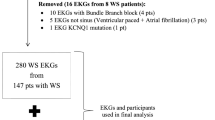
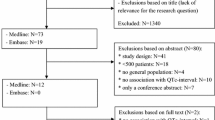
QT prolongation is an independent risk factor for cardiovascular mortality in adults. However, there is little information available on pediatric patients with QT prolongation and their outcomes. Herein, we evaluated the prevalence of QT prolongation in pediatric patients identified by an institution-wide QT alert system, and the spectrum of their phenotype. Patients with documented QT prolongation on an ECG obtained between November 2010 and June 2011 were included. There were 1303 pediatric ECGs, and 68 children had electrographically isolated QT prolongation. Comprehensive review of medical records was performed with particular attention to QT-prolonging clinical, laboratory, and medication data, which were summarized into a pro-QTc score. Overall, 68 (5 %) pediatric patients had isolated QT prolongation. The mean age of this pediatric cohort was 9 ± 6 years, and the average QTc was 494 ± 42 ms. All children had 1 or more QT-prolonging risk factor(s), most commonly QT-prolonging medications. One patient was identified with congenital long QT syndrome (LQTS), which was not previously diagnosed. In one-year follow-up, only one pediatric death (non-cardiac) occurred (1.5 %). Potentially QT-offending/pro-arrhythmic medications were changed in 80 % of pediatric patients after the physician received the QT alert. Children with QT prolongation had very low mortality and minimal polypharmacy. Still, medications and other modifiable conditions were the most common causes of QT prolongation. Children with a prolonged QTc should be evaluated for modifiable QT-prolonging factors. However, if no risk factors are present or the QTc does not attenuate after risk factor modification/removal, the child should be evaluated for congenital LQTS.



Similar content being viewed by others

Abbreviations
- ECG:
-
Electrocardiogram
- LQTS:
-
Long QT syndrome
References
Casale PN, Devereux RB, Alonso DR, Campo E, Kligfield P (1987) Improved sex-specific criteria of left-ventricular hypertrophy for clinical and computer interpretation of electrocardiograms: validation with autopsy findings. Circulation 75:565–572
CredibleMeds (2014) QT-drug list. Available from www.crediblemeds.org
De Bruin ML, Langendijk PN, Koopmans RP, Wilde AA, Leufkens HG, Hoes AW (2007) In-hospital cardiac arrest is associated with use of non-antiarrhythmic QTc-prolonging drugs. Br J Clin Pharmacol 63:216–223
Drew BJ, Ackerman MJ, Funk M et al (2010) Prevention of torsade de pointes in hospital settings a scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation 121:1047–1060
Haugaa KH, Bos JM, Tarrell RF, Morlan BW, Caraballo PJ, Ackerman MJ (2013) Institution-wide QT alert system identifies patients with a high risk of mortality. Mayo Clin Proc 88:315–325
Hobbs JB, Peterson DR, Moss AJ et al (2006) Risk of aborted cardiac arrest or sudden cardiac death during adolescence in the long-QT syndrome. J Am Med Assoc 296:1249–1254
Johnson JN, Grifoni C, Bos JM et al (2011) Prevalence and clinical correlates of QT prolongation in patients with hypertrophic cardiomyopathy. Eur Heart J 32:1114–1120
Montanez A (2004) Prolonged QTc interval and risks of total cardiovascular mortality and sudden death in the general population: a review and qualitative overview of the prospective cohort studies. Arch Intern Med 164:1796
Punn R, Lamberti JJ, Balise RR, Seslar SP (2011) QTc prolongation in children following congenital cardiac disease surgery. Cardiol Young 21:400–410
Rautaharju PM, Surawicz B, Gettes LS et al (2009) AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part IV: the ST segment, T and U waves, and the QT interval: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: endorsed by the International Society for Computerized Electrocardiology. Circulation 119:e241–e250
Roden DM (2004) Drug-induced prolongation of the QT interval. N Engl J Med 350:1013–1022
Schwartz PJ, Stramba-Badiale M, Crotti L et al (2009) Prevalence of the congenital long-QT syndrome. Circulation 120:1761–1767
Sokolow M, Lyon TR (2001) The ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Ann Noninvasive Electrocardiol 6:343–368 (Reprinted)
Soliman EZ, Howard G, Cushman M et al (2012) Prolongation of QTc and risk of stroke the REGARDS (REasons for Geographic and Racial Differences in Stroke) Study. J Am Coll Cardiol 59:1460–1467
Van Dorn CS, Johnson JN, Taggart NW, Thorkelson L, Ackerman MJ (2011) QTc values among children and adolescents presenting to the emergency department. Pediatrics 128:E1395–E1401
Zhang YY, Post WS, Blasco-Colmenares E, Dalal D, Tomaselli GF, Guallar E (2011) Electrocardiographic QT interval and mortality a meta-analysis. Epidemiology 22:660–670
Acknowledgments
This work was supported by the Mayo Clinic Windland Smith Rice Comprehensive Sudden Cardiac Death Program.
Ethical standard
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflict of interest
Dr. Ackerman is a consultant for Boston Scientific, Gilead Sciences, Medtronic, and St. Jude Medical. Dr. Ackerman and Mayo Clinic receive royalties from Transgenomic’s FAMILION-LQTS and FAMILION-CPVT genetic tests. The other authors have no conflicts of interest to disclose. None of the disclosures pertain to this study, and none of the companies provided financial support for this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Anderson, H.N., Bos, J.M., Haugaa, K.H. et al. Phenotype of Children with QT Prolongation Identified Using an Institution-Wide QT Alert System. Pediatr Cardiol 36, 1350–1356 (2015). https://doi.org/10.1007/s00246-015-1164-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-015-1164-y