
Abstract
Introduction
Most anxiolytics and sedative regimens in the intensive care unit (ICU) impair intellectual function, reducing patient autonomy, and often add to patient morbidity. Using an ICU-validated cognitive assessment tool Adapted Cognitive Exam (ACE), we performed a comparison between dexmedetomidine (DEX) and propofol (PRO) to evaluate which sedative regimen offered the least decrement in intellectual capacity.
Methods
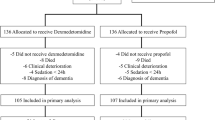
This was a prospective, randomized, double-blinded study of 30 awake and intubated brain-injured (BI, n = 18) and non-BI (12) ICU patients. Each patient received fentanyl/PRO and fentanyl/DEX titrated to a calm, awake state using a crossover design. Cognitive testing was performed at each study period using the validated 100-point Hopkins ACE cognitive battery.
Findings
Sedation with PRO diminished adjusted ACE scores (100-point exam) by a mean of −12.4 (95% CI −8.3 to −16.5, p < 0.001) while DEX, in contrast, improved ACE scores (6.8, 95% CI 1.2–12.4, p < 0.018). The difference in the change of ACE score between DEX versus PRO, our primary endpoint, was 19.2 (95% CI 12.3–26.1 p < 0.001) in favor of an improved ACE score on DEX. Patients with BI required less sedative, but effects of PRO and DEX on cognition were not changed. No serious adverse events occurred. Modest bradycardia was noted post hoc with DEX (−7.7 bpm, p < 0.01).
Interpretation
ICU patients may be offered sedation without necessarily compromising arousal or cognition. Alleviation of anxiety and agitation can singly and effectively improve mental engagement and performance if overt forebrain dysfunction is avoided. Higher ACE scores with DEX may be a consequence of the intellect-sparing yet calming effect of this drug.


Similar content being viewed by others


References
Riker RR, Shehabi Y, Bokesch PM, Ceraso D, Wisemandle W, Koura F, Whitten P, Margolis BD, Byrne DW, Ely EW, Rocha MG, SEDCOM (Safety, Efficacy of Dexmedetomidine Compared With Midazolam) Study Group (2009) Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA 301:489–499
Pandharipande PP, Pun BT, Herr DL, Maze M, Girard TD, Miller RR, Shintani AK, Thompson JL, Jackson JC, Deppen SA, Stiles RA, Dittus RS, Bernard GR, Ely EW (2007) Effect of sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically ventilated patients: the MENDS randomized controlled trial. JAMA 298:2644–2653
Payen JF, Chanques G, Mantz J, Hercule C, Auriant I, Leguillou JL, Binhas M, Genty C, Rolland C, Bosson JL (2007) Current practices in sedation and analgesia for mechanically ventilated critically ill patients: a prospective multicenter patient-based study. Anesthesiology 106:687–695
Ouimet S, Kavanagh BP, Gottfried SB, Skrobik Y (2007) Incidence, risk factors and consequences of ICU delirium. Intensive Care Med 33:66–73
Kress JP, Pohlman AS, O’Connor MF, Hall JB (2000) Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med 342:1471–1477
Hogarth DK, Hall J (2004) Management of sedation in mechanically ventilated patients. Curr Opin Crit Care 10:40–46
Robinson BR, Mueller EW, Henson K, Branson RD, Barsoum S, Tsuei BJ (2008) An analgesia-delirium-sedation protocol for critically ill trauma patients reduces ventilator days and hospital length of stay. J Trauma 65:517–526
Jacobi J, Fraser GL, Coursin DB, Riker RR, Fontaine D, Wittbrodt ET, Chalfin DB, Masica MF, Bjerke HS, Coplin WM, Crippen DW, Fuchs BD, Kelleher RM, Marik PE, Nasraway SA Jr, Murray MJ, Peruzzi WT, Lumb PD (2002) Task force of the American College of Critical Care Medicine (ACCM) of the Society of Critical Care Medicine (SCCM), American Society of Health-System Pharmacists (ASHP), American College of Chest Physicians Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med 30:119–141
Cook D (2001) Patient autonomy versus parentalism. Crit Care Med 29:N24–N25
Stocchetti N, Pagan F, Calappi E, Canavesi K, Beretta L, Citerio G, Cormio M, Colombo A (2004) Inaccurate early assessment of neurological severity in head injury. J Neurotrauma 21:1131–1140
Mirski MA, Muffelman B, Ulatowski JA, Hanley DF (1995) Sedation for the critically ill neurologic patient. Crit Care Med 23:2038–2053
Shehabi Y, Grant P, Wolfenden H, Hammond N, Bass F, Campbell M, Chen J (2009) Prevalence of delirium with dexmedetomidine compared with morphine based therapy after cardiac surgery: a randomized controlled trial (DEXmedetomidine COmpared to Morphine-DEXCOM Study). Anesthesiology 111:1075–1084
Sessler CN, Gosnell MS, Grapp MJ, Brophy GM, O’Neal PV, Keane KA, Tesoro EP, Elswick RK (2002) The Richmond Agitation-Sedation Scale, validity and reliability in adult intensive care unit patients. Am J Resp Crit Care Med 166:1338–1344
Lewin JJ, LeDroux, Thompson, Griswold, Bishop, Mirski MA (2008) Measurement of cognition in intubated & non-intubated critically ill patients: validity and reliability of the Johns Hopkins Adapted Cognitive Exam (ACE). Crit Care Med (suppl):A125
Mirski MA, Lewin JJ III (2009) Sedation and pain management in the ICU. In: Vincent J-L (ed) Yearbook of intensive care medicine. Springer, Heidelberg, pp 881–905
Ely EW, Inouye SK, Bernard GR, Gordon S, Francis J, May L, Truman B, Speroff T, Gautam S, Margolin R, Hart RP, Dittus R (2001) Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU). JAMA 286:2703–2710
Soja SL, Pandharipande PP, Fleming SB, Cotton BA, Miller LR, Weaver SG, Lee BT, Ely EW (2008) Implementation, reliability testing, and compliance monitoring of the confusion assessment method for the intensive care unit in trauma patients. Intensive Care Med 34:1263–1268
Martin E, Ramsay G, Mantz J, Sum-Ping ST (2003) The role of the alpha2-adrenoceptor agonist dexmedetomidine in postsurgical sedation in the intensive care unit. J Intensive Care Med 18:29–41
Gepts E, Camu F, Cockshott ID, Douglas EJ (1987) Disposition of propofol administered as constant rate intravenous infusions in humans. Anesth Analg 66:1256–1263
Vree TB, de Grood P-MRM, van Beem HBH, Booij LHDJ (1997) Disposition and renal clearance of propofol and its glucuronide metabolites after a short intravenous infusion of propofol. Clin Drug Invest 13:145–151
De Wolf AM, Fragen RJ, Avram MJ, Fitzgerald PC, Rahimi-Danesh F (2001) The pharmacokinetics of dexmedetomidine in volunteers with severe renal impairment. Anesth Analgesia 93:1205–1209
Dyck JB, Maze M, Haack C, Vuorilehto L, Shafer SL (1993) Computer-controlled infusion of intravenous dexmedetomidine hydrochloride in adult human volunteers. Anesthesiology 78:821–828
Diggle PJ, Heagerty P, Liang K-Y, Zeger SL (2002) Analysis of longitudinal data, 2nd edn. Oxford University Press, New York
Thomason JW, Shintani A, Peterson JF, Pun BT, Jackson JC, Ely EW (2005) Intensive care unit delirium is an independent predictor of longer hospital stay: a prospective analysis of 261 non-ventilated patients. Crit Care 9:R375–R381
Smith C, McEwan AI, Jhaveri R, Wilkinson M, Goodman D, Smith LR, Canada AT, Glass PS (1994) The interaction of fentanyl on the Cp50 of propofol for loss of consciousness and skin incision. Anesthesiology 81:820–828
Kazama T, Ikeda K, Morita K (1997) Reduction by fentanyl of the Cp50 values of propofol and hemodynamic responses to various noxious stimuli. Anesthesiology 87:213–227
Hendrickx JF, Eger EI 2nd, Sonner JM, Shafer SL (2008) Is synergy the rule? A review of anesthetic interactions producing hypnosis and immobility. Anesth Analg 107:494–506
Garcia R, Benet M, Arnau C, Cobo E (2004) Efficiency of the cross-over design: an empirical estimation. Stat Med 23:3773–3780
Veselis RA, Reinsel RA, Feshchenko VA, Wroński M (1997) The comparative amnestic effects of midazolam, propofol, thiopental, and fentanyl at equisedative concentrations. Anesthesiology 87:749–764
Weinbroum AA, Halpern P, Rudick V, Sorkine P, Freedman M, Geller E (1997) Midazolam versus propofol for long-term sedation in the ICU: a randomized prospective comparison. Intensive Care Med 23:1258–1263
Pandharipande P, Shintani A, Peterson J, Pun BT, Wilkinson GR, Dittus RS, Bernard GR, Ely EW (2006) Lorazepam is an independent risk factor for transitioning to delirium in intensive care unit patients. Anesthesiology 104:21–26
Pandharipande P, Cotton BA, Shintani A, Thompson J, Pun BT, Morris JA Jr, Dittus R, Ely EW (2008) Prevalence and risk factors for development of delirium in surgical and trauma intensive care unit patients. J Trauma 65:34–41
Acknowledgments
The authors would like to acknowledge the support of the Johns Hopkins & Bayview pharmacists Laura Wachter, Annette Rowden, Henry Choi, and Jim Monolakis, the neuroscience ICU nurses, especially Gail Biba, Patricia Trionfo, Theresa Blair, and Chris Boileau, and DSMB Committee Chair—Dr. Brent Petty.
Conflict of interest statement
ANIST was an investigator-initiated research study funded in part from a grant from Hospira. There was no input as to hypothesis, trial design, data acquisition, or analysis from the study sponsor. Partial support also was courtesy of The Gannaway Fund, an internal institutional philanthropic gift fund for research.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Mirski, M.A., Lewin, J.J., LeDroux, S. et al. Cognitive improvement during continuous sedation in critically ill, awake and responsive patients: the Acute Neurological ICU Sedation Trial (ANIST). Intensive Care Med 36, 1505–1513 (2010). https://doi.org/10.1007/s00134-010-1874-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-010-1874-9