
Abstract
Background
Hematoma expansion after acute intracerebral hemorrhage occurs most frequently in patients presenting within 3 h of symptom onset. However, the majority of patients present outside this window or with an unknown onset time. We investigated the prevalence of hematoma expansion in these patients and assessed the accuracy of the CT angiography (CTA) spot sign for identifying risk of hematoma expansion.
Methods
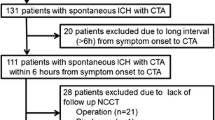
We analyzed 391 consecutive patients undergoing CTA and a followup CT. CTA spot sign readings were performed by two experienced readers and hematoma expansion was assessed by means of semi-automated software.
Results
Hematoma expansion occurred in 18 % of patients. When stratified by time from symptom onset to initial CT, hematoma expansion rates were: 39 % within 3 h; 11 % between 3 and 6 h, 11 % beyond 6 h (but with known onset), and 20 % in patients with unknown symptom onset. Of patients who developed hematoma expansion, only 38 % presented within 3 h. The accuracy of the spot sign in predicting hematoma expansion was 0.67 for patients presenting within 3 h, 0.83 between 3 and 6 h, 0.88 after 6 h, and 0.76 for patients presenting with an unknown onset time.
Conclusions
A substantial number of patients destined to suffer from hematoma expansion present either late or with an unknown symptom onset time. The CTA spot sign accurately identifies patients destined to expand regardless of time from symptom onset, and may therefore open a path to offer clinical trials and novel therapies to the many patients who do not present acutely.

Similar content being viewed by others

References
Qureshi AI, Tuhrim S, Broderick JP, Batjer HH, Hondo H, Hanley DF. Spontaneous intracerebral hemorrhage. N Engl J Med. 2001;344:1450–60.
van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9:167–76.
Broderick JP, Brott TG, Duldner JE, Tomsick T, Huster G. Volume of intracerebral hemorrhage. A powerful and easy-to-use predictor of 30-day mortality. Stroke. 1993;24:987–93.
Davis SM, Broderick J, Hennerici M, et al. Hematoma growth is a determinant of mortality and poor outcome after intracerebral hemorrhage. Neurology. 2006;66:1175–81.
Dowlatshahi D, Demchuk AM, Flaherty ML, et al. Defining hematoma expansion in intracerebral hemorrhage: relationship with patient outcomes. Neurology. 2011;76:1238–44.
Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. 2005;352:777–85.
Mayer SA, Brun NC, Begtrup K, et al. Efficacy and safety of recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. 2008;358:2127–37.
Anderson CS, Huang Y, Wang JG, et al. Intensive blood pressure reduction in acute cerebral haemorrhage trial (INTERACT): a randomised pilot trial. Lancet Neurol. 2008;7:391–9.
Delcourt C, Huang Y, Wang J, et al. The second (main) phase of an open, randomised, multicentre study to investigate the effectiveness of an intensive blood pressure reduction in acute cerebral haemorrhage trial (INTERACT2). Int J Stroke. 2010;5:110–6.
Qureshi AI, Palesch YY. Antihypertensive treatment of acute cerebral hemorrhage (ATACH) II: design, methods, and rationale. Neurocrit Care. 2011;15:559–76.
Aviv RI, Gladstone D, Goldstein J, et al. Contrast extravasation predicts hematoma growth: where to now? AJNR Am J Neuroradiol. 2008;29:E80.
Goldstein JN, Fazen LE, Snider R, et al. Contrast extravasation on CT angiography predicts hematoma expansion in intracerebral hemorrhage. Neurology. 2007;68:889–94.
Wada R, Aviv RI, Fox AJ, et al. CT angiography “spot sign” predicts hematoma expansion in acute intracerebral hemorrhage. Stroke. 2007;38:1257–62.
Demchuk AM, Dowlatshahi D, Rodriguez-Luna D, et al. Prediction of haematoma growth and outcome in patients with intracerebral haemorrhage using the CT-angiography spot sign (PREDICT): a prospective observational study. Lancet Neurol. 2012;11:307–14.
Kim J, Smith A, Hemphill JC 3rd, et al. Contrast extravasation on CT predicts mortality in primary intracerebral hemorrhage. AJNR Am J Neuroradiol. 2008;29:520–5.
Li N, Wang Y, Wang W, et al. Contrast extravasation on computed tomography angiography predicts clinical outcome in primary intracerebral hemorrhage: a prospective study of 139 cases. Stroke. 2011;42:3441–6.
Delgado Almandoz JE, Yoo AJ, Stone MJ, et al. Systematic characterization of the computed tomography angiography spot sign in primary intracerebral hemorrhage identifies patients at highest risk for hematoma expansion: the spot sign score. Stroke. 2009;40:2994–3000.
Delgado Almandoz JE, Yoo AJ, Stone MJ, et al. The spot sign score in primary intracerebral hemorrhage identifies patients at highest risk of in-hospital mortality and poor outcome among survivors. Stroke. 2010;41:54–60.
Brott T, Broderick J, Kothari R, et al. Early hemorrhage growth in patients with intracerebral hemorrhage. Stroke. 1997;28:1–5.
Brouwers HB, Biffi A, Ayres AM, et al. APOE genotype predicts hematoma expansion in lobar intracerebral hemorrhage. Stroke. 2012;43:1490–5.
Mayer SA. Ultra-early hemostatic therapy for intracerebral hemorrhage. Stroke. 2003;34:224–9.
Wardlaw JM. Prediction of haematoma expansion with the CTA spot sign: a useful biomarker? Lancet Neurol. 2012;11:294–5.
Mayer SA, Davis SM, Skolnick BE, et al. Can a subset of intracerebral hemorrhage patients benefit from hemostatic therapy with recombinant activated factor VII? Stroke. 2009;40:833–40.
Acknowledgments
All funding entities had no involvement in study design, data collection, analysis and interpretation, writing of the manuscript, and in the decision to submit for publication. The project described was supported by the Grant Numbers R01NS073344, R01NS059727, and 5K23NS059774 from the National Institutes of Health—National Institute of Neurological Disorders and Stroke (NIH–NINDS) and the American Heart Association Grant Number 0755984T. Dr. Brouwers was supported by the NIH–NINDS SPOTRIAS fellowship grant P50NS051343. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Neurological Disorders and Stroke or the National Institutes of Health.
Disclosures
H.B. Brouwers, none; G.J. Falcone, none; K.A. McNamara, none; A.M. Ayres, none; A. Oleinik, none; K. Schwab, none; J.M. Romero, Imaging Committee DIAS trial/advisory board Lundbeck pharmaceuticals; A. Viswanathan, none; S.M. Greenberg, Research Grant NIH, Honoraria: Medtronic, Pfizer, Consultant/advisory board: Hoffman-La Roche, Janssen Alzheimer Immunotherapy, Bristol-Myers Squibb Company; J. Rosand, Research Grant NIH and American Heart Association; J.N. Goldstein, Research Grant NIH–NINDS, Consultant/advisory board CSL Behring.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Brouwers, H.B., Falcone, G.J., McNamara, K.A. et al. CTA Spot Sign Predicts Hematoma Expansion in Patients with Delayed Presentation After Intracerebral Hemorrhage. Neurocrit Care 17, 421–428 (2012). https://doi.org/10.1007/s12028-012-9765-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-012-9765-2