
Abstract
Background
Decompressive hemicraniectomy reduces mortality after space-occupying MCA infarction. Data on the general public’s opinion toward interventions that can save lives but leave the survivors impaired are lacking.
Methods
In this population-based epidemiological study in a German city, we surveyed 312 adults in a telephone interview. Here, we presented a scenario of a space-occupying MCA infarct. We evaluated probands’ attitude toward decompressive surgery in general, and toward outcome scenarios according to Rankin scale (RS) definitions.
Results
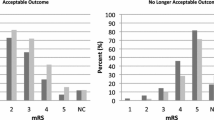
312 persons (157 women, 52 ± 20 years) were interviewed. 58 persons had difficulty comprehending the proposed scenario, most of them being of advanced age (79 ± 5 years). From the remaining 254 responders 5 (2%) persons favoured surgical intervention, 149 (58%) were undecided, and 100 (39%) were opposed to surgery. The number of individuals opting for surgery rose in scenarios with a better outcome: If very severe impairment was anticipated (RS 5), only 3 (1%) persons favored surgery. With severe (RS 4), moderate (RS3), and slight impairment (RS2) the numbers were at 16 (6%), 60 (24%), and 161 (63%), respectively. We found no association with age, sex, religion, education, self-estimated health status, or marital status.
Conclusions
Explaining complex medical situations to laypersons poses a major problem, particularly to those of old age. Only a minority favors life-saving medical interventions if survival is associated with deficits of unpredictable degree. The majority of persons does not favor intervention even if only moderate impairment is anticipated. Decompressive surgery may in fact be against the values of many individuals.

Similar content being viewed by others

References
Vahedi K, Hofmeijer J, Juettler E, et al. Early decompressive surgery in malignant infarction of the middle cerebral artery: a pooled analysis of three randomised controlled trials. Lancet Neurol. 2007;6:215–22.
Kakar V, Nagaria J, John Kirkpatrick P. The current status of decompressive craniectomy. Br J Neurosurg. 2009;23:147–57.
Hofmeijer J, Kappelle LJ, Algra A, et al. Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery infarction with Life-threatening Edema Trial [HAMLET]): a multicentre, open, randomised trial. Lancet Neurol. 2009;8:326–33.
Samsa GP, Matchar DB, Goldstein L, et al. Utilities for major stroke: results from a survey of preferences among persons at increased risk for stroke. Am Heart J. 1998;136:703–13.
Statistical Yearbook 2010 for the Federal Republic of Germany. Federal Statistical Office. Wiesbaden, 2010. www.destatis.de. Accessed 21 Sept 2011.
Nakagawa K, Bianchi MT, Nakagawa SS, et al. Aggressive care after a massive stroke in young patients: is that what they want? Neurocrit Care. 2010;13:118–22.
Flory J, Emanuel E. Interventions to improve research participants’ understanding in informed consent for research: a systematic review. JAMA. 2004;292:1593–601.
Eran A, Erdmann E, Er F. Informed consent prior to coronary angiography in a real world scenario: what do patients remember? PLoS ONE. 2010;5:e15164. doi:10.1371/journal.pone.0015164.
Sugarman J, McCrory DC, Hubal RC. Getting meaningful informed consent from older adults: a structured literature review of empirical research. J Am Geriatr Soc. 1998;46:517–24.
Huttner HB, Schwab S. Malignant middle cerebral artery infarction: clinical characteristics, treatment strategies, and future perspectives. Lancet Neurol. 2009;8:949–58.
van Swieten JC, Koudstaal PJ, Visser MC, et al. Interobserver agreement for the assessment of handicap in stroke patients. Stroke. 1988;19:604–7.
Puetz V, Campos CR, Eliasziw M, et al. Assessing the benefits of hemicraniectomy: what is a favourable outcome? Lancet Neurol. 2007;6:580.
Neudert C, Wasner M, Borasio GD. Individual quality of life is not correlated with health-related quality of life or physical function in patients with amyotrophic lateral sclerosis. J Palliat Med. 2004;7:551–7.
Bruno M-A, Bernheim J, Ledoux D, et al. A survey on self-assessed well being in a cohort of chronic locked-in syndrome patients: happy majority, miserable minority. BMJ Open. 2011;1:e000039. doi:10.1136/bmjopen-2010-000039.
von Steinbuechel N, Richter S, Morawetz C, et al. Assessment of subjective health and health-related quality of life in persons with acquired or degenerative brain injury. Curr Opin Neurol. 2005;18:681–91.
Owolabi MO. What are the consistent predictors of generic and specific post-stroke health-related quality of life? Cerebrovasc Dis. 2010;29:105–10.
Wilson JT, Hareendran A, Hendry A, et al. Reliability of the modified Rankin Scale across multiple raters: benefits of a structured interview. Stroke. 2005;36:777–81.
Zhao H, Collier JM, Quah DM, et al. The modified Rankin Scale in acute stroke has good inter-rater-reliability but questionable validity. Cerebrovasc Dis. 2010;29:188–193.
Larach DR, Larach DB, Larach MG. A life worth living: seven years after craniectomy. Neurocrit Care. 2009;11:106–11.
Kiphuth IC, Kohrmann M, Lichy C, et al. Hemicraniectomy for malignant middle cerebral artery infarction: retrospective consent to decompressive surgery depends on functional long-term outcome. Neurocrit Care. 2010;13:380–4.
Malmivaara K, Ohman J, Kivisaari R, et al. Cost-effectiveness of decompressive craniectomy in non-traumatic neurological emergencies. Eur J Neurol. 2011;18:402–9.
Vahedi K, Benoist L, Kurtz A, et al. Quality of life after decompressive craniectomy for malignant middle cerebral artery infarction. J Neurol Neurosurg Psychiatry. 2005;76:1181–2.
Skoglund TS, Eriksson-Ritzen C, Sorbo A, et al. Health status and life satisfaction after decompressive craniectomy for malignant middle cerebral artery infarction. Acta Neurol Scand. 2008;117:305–10.
Buchanan KM, Elias LJ, Goplen GB. Differing perspectives on outcome after subarachnoid hemorrhage: the patient, the relative, the neurosurgeon. Neurosurgery. 2000;46:831–8.
Rothwell PM, Slattery J, Warlow CP. A systematic review of the risks of stroke and death due to endarterectomy for symptomatic carotid stenosis. Stroke. 1996;27:260–5.
Novick G. Is there a bias against telephone interviews in qualitative research? Res Nurs Health. 2008;31:391–8.
Feveile H, Olsen O, Hogh A. A randomized trial of mailed questionnaires versus telephone interviews: response patterns in a survey. BMC Med Res Methodol. 2007;7:27.
Smith EM. Telephone interviewing in healthcare research: a summary of the evidence. Nurse Res. 2005;12:32–41.
Bowling A. Mode of questionnaire administration can have serious effects on data quality. J Public Health (Oxf). 2005;27:281–91.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Klein, A., Kuehner, C. & Schwarz, S. Attitudes in the General Population Towards Hemi-Craniectomy for Middle Cerebral Artery (MCA) Infarction. A Population-Based Survey. Neurocrit Care 16, 456–461 (2012). https://doi.org/10.1007/s12028-012-9677-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-012-9677-1