
Abstract
Background
Children with spastic diplegia frequently show excessive knee extension (stiff-knee gait) throughout swing phase, which may interfere with foot clearance. Abnormal rectus femoris activity is commonly associated with a stiff-knee gait. Rectus femoris transfer has been recommended to enhance knee flexion during swing. However, recent studies suggest the transfer does not generate a knee flexor moment but diminishes knee extension moment in swing and MRI studies show the transferred tendons can be constrained by scarring to underlying muscles. Thus, it is possible knee flexion would be improved by distal rectus release rather than transfer since it would not be adherent to the underlying muscles.
Questions/purposes
We therefore determined whether rectus femoris distal tendon resection improves knee ROM and kinematic characteristics of stiff-knee gait in patients with spastic diplegia.
Patients and Methods
We studied 45 patients who underwent rectus femoris distal tendon resection as a part of multilevel surgery. Rectus femoris procedures were indicated based on kinematic characteristics of stiff-knee gait. All patients were walkers and had a mean age at surgery of 13 years (range, 6–22 years). We obtained gait analyses before surgery and at mean 2-year followup. We based postoperative assessment on clinical evaluation and gait analysis data.
Results
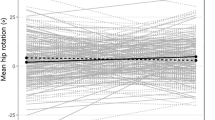
At followup, rectus femoris distal tendon resection was associated with improved knee ROM and timing of peak knee flexion in swing, and the absolute values of peak knee flexion became normal for those patients who showed abnormal preoperative values.
Conclusions
Kinematic parameters of stiff-knee gait improved after rectus femoris distal tendon resection. Given the preliminary nature of our report, we intend to study the same patients to assess outcomes at a longer followup.
Level of Evidence
Level IV, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.


Similar content being viewed by others

References
Asakawa DS, Blemker SS, Gold GE, Delp SL. In vivo motion of the rectus femoris muscle after tendon transfer surgery. J Biomech. 2002;35:1029–1037.
Asakawa DS, Blemker SS, Rab GT, Bagley A, Delp SL. Three-dimensional muscle-tendon geometry after rectus femoris tendon transfer. J Bone Joint Surg Am. 2004;86:348–354.
Davids JR, Õunpuu S, DeLuca PA, Davis RB. Optimization of walking ability of children with cerebral palsy. J Bone Joint Surg Am. 2003;85:2224–2234.
Gage JR, Perry J, Hicks RR, Koop S. Werntz JR. Rectus femoris transfer to improve knee function of children with cerebral palsy. Dev Med Child Neurol. 1987;29:159–166.
Gold GE, Asakawa DS, Blemker SS, Delp SL. Magnetic resonance imaging findings after rectus femoris transfer surgery. Skeletal Radiol. 2004;33:34–40.
Hemo Y, Aiona MD, Pierce RA, Dorociack R, Sussman M. Comparison of rectus femoris transposition with traditional transfer for the treatment of stiff knee gait in patients with cerebral palsy. J Child Orthop. 2007;1:37–41.
Kadaba MP, Ramakrishnan HK, Wootten ME. Measurement of lower extremity kinematics during level walking. J Orthop Res. 1990;8:383–392.
Moreau N, Tinsley S. Progression of knee joint kinematics in children with cerebral palsy with and without rectus femoris transfers: a long-term follow up. Gait Posture. 2005;22:132–137.
Õunpuu S, DeLuca P, Davis R, Romness M. Long-term effects of femoral derotation osteotomies: an evaluation using three-dimensional gait analysis. J Pediatr Orthop. 2002;22:139–145.
Õunpuu S, Muik E, Davis RB 3rd, Gage JR, DeLuca PA. Rectus femoris surgery in children with cerebral palsy. Part I. The effect of rectus femoris transfer location on knee motion. J Pediatr Orthop. 1993;13:325–330.
Õunpuu S, Muik E, Davis RB 3rd, Gage JR, DeLuca PA. Rectus femoris surgery in children with cerebral palsy. Part II. A comparison between the effect of transfer and release of the distal rectus femoris on knee motion. J Pediatr Orthop. 1993;13:331–335.
Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997;39:214–223.
Perry J. Distal rectus femoris transfer. Dev Med Child Neurol. 1987;29:153–158.
Riewald SA, Delp SL. The action of the rectus femoris muscle following distal tendon transfer: does it generate knee flexion moment? Dev Med Child Neurol. 1997;39:99–105.
Saraph V, Zwick E, Zwick G, Steinwender C, Steinwender G, Linhart W. Multilevel surgery in spastic diplegia: evaluation by physical examination and gait analysis in 25 children. J Pediatr Orthop. 2002;22:150–157.
Saw A, Smith PA, Sirirungruangsarn Y, Chen S, Hassani S, Harris G, Kuo KN. Rectus femoris transfer for children with cerebral palsy: long-term outcome. J Pediatr Orthop. 2003;23:672–678.
Sutherland DH, Davids JR. Common gait abnormalities of the knee in cerebral palsy. Clin Orthop Relat Res. 1993;288:139–147.
Sutherland DH, Larsen LJ, Mann R. Rectus femoris release in selected patients with cerebral palsy: a preliminary report. Dev Med Child Neurol. 1975;17:26–34.
Sutherland DH, Santi M, Abel MF. Treatment of stiff-knee gait in cerebral palsy: a comparison by gait analysis of distal rectus femoris transfer versus proximal rectus release. J Pediatr Orthop. 1990;10:433–441.
Waters RL, Garland DE, Perry J. Stiff-legged gait in hemiplegia: surgical correction. J Bone Joint Surg Am. 1979;61:927–933.
Acknowledgment
The authors thank Dr. Franck Fitoussi for assistance regarding the conception of the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing, arrangements, etc.) that might pose a conflict of interest in connection with the submitted article.
Each author certifies that his or her institution waived approval for the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
This work was performed at Robert Debre Hospital and Motion Analysis Laboratory at Bois Larris Rehabilitation Center.
About this article
Cite this article
Presedo, A., Megrot, F., Ilharreborde, B. et al. Rectus Femoris Distal Tendon Resection Improves Knee Motion in Patients With Spastic Diplegia. Clin Orthop Relat Res 470, 1312–1319 (2012). https://doi.org/10.1007/s11999-011-2019-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-011-2019-3