
Abstract
Background
Nonalcoholic fatty liver disease (NAFLD) represents the most common cause of chronic liver disease in the USA. Biopsy has been the standard for determining fibrosis but is invasive, costly, and associated with risk. Previous studies report a calculated “NAFLD fibrosis scores” (cNFS) as a means to overcome the need for biopsy. We compared cNFS versus biopsy-pathological scoring for patients undergoing bariatric surgery.
Methods
We retrospectively reviewed patients with available preoperative labs and patient information undergoing Roux-en-Y gastric bypass (RYGBP) surgery at a single institution over a 5.5-year period. Biopsy samples were blind scored by a single hepatopathologist and compared with scores calculated using a previously reported cNFS.
Results
Of the 225 patients that met the inclusion criteria, the mean body mass index was 44.6 ± 5.4 kg/m2 and 85 % were female. Using the cNFS, 39.6 % of patients were categorized into low fibrosis, 52 % indeterminate, and 8.4 % high fibrosis groups. Analysis of fibrosis by pathology scoring demonstrated 2 of 89 (2.2 %) and 7 of 110 (3.4 %) had significant fibrosis in the low and intermediate groups, respectively. Conversely, in the high fibrosis group calculated by cNFS, only 6 of 19 (31.6 %) exhibited significant fibrosis by pathology scoring.
Conclusions
No definitive model for accurately predicting presence of NAFLD and fibrosis currently exits. Furthermore, under no circumstances should a clinical “NAFLD fibrosis score” replace liver biopsy at this time for RYGBP patients.



Similar content being viewed by others

References
Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology. 2007;45:846–54.
Bedogni G, Miglioli L, Masutti F, et al. Prevalence of and risk factors for nonalcoholic fatty liver disease: the Dionysos nutrition and liver study. Hepatology. 2005;42:44–52.
Fan JG, Zhu J, Li XJ, et al. Prevalence of and risk factors for fatty liver in a general population of Shanghai, China. J Hepatol. 2005;43:508–14.
Browning JD, Szczepaniak LS, Dobbins R, et al. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology. 2004;40:1387–95.
Pimentel SK, Strobel R, Goncalves CG, et al. Evaluation of the nonalcoholic fat liver disease fibrosis score for patients undergoing bariatric surgery. Arq Gastroenterol. 2010;47:170–3.
Dixon JB. Surgical treatment for obesity and its impact on non-alcoholic steatohepatitis. Clin Liver Dis. 2007;11:141–54. ix–x.
Ong JP, Elariny H, Collantes R, et al. Predictors of nonalcoholic steatohepatitis and advanced fibrosis in morbidly obese patients. Obes Surg. 2005;15:310–5.
Papadia FS, Marinari GM, Camerini G, et al. Liver damage in severely obese patients: a clinical–biochemical–morphologic study on 1,000 liver biopsies. Obes Surg. 2004;14:952–8.
Ong JP, Younossi ZM. Epidemiology and natural history of NAFLD and NASH. Clin Liver Dis. 2007;11:1–16. vii.
Tsai S, Choti MA, Assumpcao L, et al. Impact of obesity on perioperative outcomes and survival following pancreaticoduodenectomy for pancreatic cancer: a large single-institution study. J Gastrointest Surg. 2010;14:1143–50.
Qureshi K, Clements RH, Abrams GA. The utility of the "NAFLD fibrosis score" in morbidly obese subjects with NAFLD. Obes Surg. 2008;18:264–70.
Berker D, Koparal S, Isik S, et al. Compatibility of different methods for the measurement of visceral fat in different body mass index strata. Diagn Interv Radiol. 2010;16:99–105.
Gholam PM, Kotler DP, Flancbaum LJ. Liver pathology in morbidly obese patients undergoing Roux-en-Y gastric bypass surgery. Obes Surg. 2002;12:49–51.
Sanyal AJ, Banas C, Sargeant C, et al. Similarities and differences in outcomes of cirrhosis due to nonalcoholic steatohepatitis and hepatitis C. Hepatology. 2006;43:682–9.
Caldwell SH, Oelsner DH, Iezzoni JC, et al. Cryptogenic cirrhosis: clinical characterization and risk factors for underlying disease. Hepatology. 1999;29:664–9.
Bugianesi E, Leone N, Vanni E, et al. Expanding the natural history of nonalcoholic steatohepatitis: from cryptogenic cirrhosis to hepatocellular carcinoma. Gastroenterology. 2002;123:134–40.
Adams LA, Lymp JF, St Sauver J, et al. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology. 2005;129:113–21.
Dixon JB, Bhathal PS, O'Brien PE. Nonalcoholic fatty liver disease: predictors of nonalcoholic steatohepatitis and liver fibrosis in the severely obese. Gastroenterology. 2001;121:91–100.
Tai CM, Huang CK, Hwang JC, et al. Improvement of nonalcoholic fatty liver disease after bariatric surgery in morbidly obese Chinese patients. Obes Surg. 2012;22:1016–21.
Gunneson TJ, Menon KV, Wiesner RH, et al. Ultrasound-assisted percutaneous liver biopsy performed by a physician assistant. Am J Gastroenterol. 2002;97:1472–5.
Szymczak A, Simon K, Inglot M, et al. Safety and effectiveness of blind percutaneous liver biopsy: analysis of 1412 procedures. Hepat Mon. 2012;12:32–7.
Ratziu V, Charlotte F, Heurtier A, et al. Sampling variability of liver biopsy in nonalcoholic fatty liver disease. Gastroenterology. 2005;128:1898–906.
Tanwar S, Trembling PM, Guha IN, Parkes J, Kaye P, Burt AD, Ryder SD, et al. Validation of PIIINP for the detection and assessment of non-alcoholic steatohepatitis in patients with non-alcoholic fatty liver disease. Hepatology 2013; (in press).
Poynard T, Ratziu V, Charlotte F, et al. Diagnostic value of biochemical markers (NASH test) for the prediction of non alcoholo steato hepatitis in patients with non-alcoholic fatty liver disease. BMC Gastroenterol. 2006;6:34.
Younossi ZM, Jarrar M, Nugent C, et al. A novel diagnostic biomarker panel for obesity-related nonalcoholic steatohepatitis (NASH). Obes Surg. 2008;18:1430–7.
Moretto M, Kupski C, da Silva VD, et al. Effect of bariatric surgery on liver fibrosis. Obes Surg. 2012;22:1044–9.
Kumar R, Rastogi A, Sharma MK, Bhatia V, Tyagi P, Sharma P, Garg H, et al. Liver stiffness measurements in patients with different stages of nonalcoholic fatty liver disease: diagnostic performance and clinicopathological correlation. Dig Dis Sci 2013; (in press).
McPherson S, Stewart SF, Henderson E, et al. Simple non-invasive fibrosis scoring systems can reliably exclude advanced fibrosis in patients with non-alcoholic fatty liver disease. Gut. 2010;59:1265–9.
Ruffillo G, Fassio E, Alvarez E, et al. Comparison of NAFLD fibrosis score and BARD score in predicting fibrosis in nonalcoholic fatty liver disease. J Hepatol. 2011;54:160–3.
Alberti KG, Zimmet P, Shaw J. Metabolic syndrome—a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet Med. 2006;23:469–80.
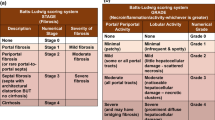
Kleiner DE, Brunt EM, Van Natta M, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41:1313–21.
Brunt EM. Grading and staging the histopathological lesions of chronic hepatitis: the Knodell histology activity index and beyond. Hepatology. 2000;31:241–6.
Conflict of Interest Disclosure Statement
The authors declare no conflict of interest.
Funding
No financial support was received for this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Simo, K.A., McKillop, I.H., McMillan, M.T. et al. Does a Calculated “NAFLD Fibrosis Score” Reliably Negate the Need for Liver Biopsy in Patients Undergoing Bariatric Surgery?. OBES SURG 24, 15–21 (2014). https://doi.org/10.1007/s11695-013-1044-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-013-1044-6