
Abstract
Topiramate is known to be efficacious in migraine prophylaxis, but its optimal dose has not been systematically studied in the Asian population. Here, we show that a fixed low dose of topiramate 25 mg/day is efficacious in migraine prophylaxis and also attest to advantages in terms of medication cost savings and more favourable side effect profile.
Similar content being viewed by others


Introduction
Migraine is a common neurological illness worldwide leading to significant effects on morbidity, productivity and quality of life [1]. Prevention of migraine attacks is an important clinical strategy.
The anticonvulsant topiramate is known in the Western setting to be effective in migraine prevention [2–4]. These previous studies, of which Asians form the minority, have employed dosages at or above 100 mg/day for prophylaxis. However, there is evidence that lower dosages of topiramate may be effective in migraine prevention, particularly in the Asian population [5–7]. This may have important clinical implications in terms of cost and side effects. To our knowledge, three previous studies comprising Koreans, Chinese and Indians, have addressed the use of topiramate in the Asian patients [5–7]. Two studies had employed dosages of at or above 50 mg/day [5, 6], while the third, utilizing a variable titration method, had suggested that daily dosages as low as 25 mg may be effective [7]. In addition, two other studies involving Iranian patients have utilized topiramate dosages up to 50 mg/day and concluded it to be as effective as propanolol and sodium valproate in migraine prophylaxis [8, 9], providing further evidence of its efficacy in Asians. In this study, we sought to further clarify dosage issues in a prospective dosing study of migraine patients in the multiracial Asian setting.
Methods
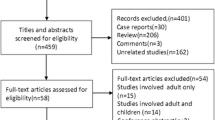
With local ethical committee (Singapore General Hospital Institutional Review Board) approval, we prospectively screened 82 patients having migraine with or without aura, as defined by the International Classification of Headache Disorders 2nd Edition [10]. In particular, we had ensured that patients included should have at least four headache episodes in the preceding 4 weeks, with each episode at least four of ten in severity on the visual analogue scale (VAS). Otherwise, subjects were considered screen failures. Of these, 42 were excluded: 7 patients became un-contactable prior to randomization, 23 were screen failures and 12 had withdrawn consent during the study.
A total of 40 patients (age range 18–64, mean age 38, 30 females, 10 males) were randomized into the study. There were 22 Chinese, 6 Malays, 8 Indians and 4 Eurasians. Patients were recruited in a consecutive fashion from a headache specialist clinic in a tertiary general hospital. Each was briefed upon randomization on how to record symptoms and side effects into the headache diary.
Each patient had kept a headache diary 4 weeks prior to randomization, documenting baseline migraine attacks over this period. Patients documented frequency as the number of days with headache in the preceding 4 weeks, duration of the most severe attack in a day in hours, and severity measured as the worst period during an attack on a VAS from 0 to 10 cm. During the entire treatment period, they were allowed symptomatic medications such as paracetamol, but triptans and opioids were disallowed. However, any prior use of prophylactic medication of any class at any time documented was an exclusion criterion. We excluded all subjects with history suggesting analgesic overuse. This was defined as usage of triptans >3 days a week, simple analgesics >4 days a week or narcotic analgesics >2 days a week.
Each patient was randomized to receive 25, 50, 75 or 100 mg of topiramate as an evening dose, with 10 patients in each arm. For the 50 mg arm, patients started on 25 mg for 1 week before continuing with 50 mg for the rest of the study. Similarly, for the 75 mg arm, patients started with 25 mg for 1 week, 50 mg for the second week, and 75 mg for the subsequent weeks. The dose escalation was in a similar manner for the 100 mg arm. The end-point of the study was 12 weeks after achieving the intended topiramate dosage for that particular treatment arm, and patients returned for follow-up every 4 weeks after starting treatment. Comparisons were made between migraine attacks at baseline and the 4-week period prior to the end-point (Fig. 2). It should be noted that upward titration of dosages were gradual and necessary to minimize side effects and drop outs. For the 50, 75 and 100 mg arms, each patient would have received a total of 12 weeks of the intended dose of that particular arm before study end-point was achieved.
Statistical calculations were performed with SPSS for Windows package, employing the Wilcoxon Signed Rank, Kruskal–Wallis and Pearson’s correlation tests. A p value < 0.05 was regarded as statistically significant.
Results
Of the 40 patients who had completed the trial, no significant differences in baseline headache frequency, duration and severity was found between the four treatment arms.
Overall, we found that topiramate significantly reduced headache frequency (headache days) comparing baseline to end-point (Wilcoxon Signed Rank test, Z = −3.47, p = 0.001). However, no significant differences were found for headache duration (Wilcoxon Signed Rank test, Z = −0.23, p = 0.82) or severity (Wilcoxon Signed Rank test, Z = −0.31, p = 0.76).
In terms of side effects, paresthesia was by far the most commonly encountered in 55% of patients. However, its incidence was highly correlated with increasing dosage (Pearson’s correlation, r = 0.96, p < 0.001).
Figure 1 summarizes overall headache parameters comparing baseline to study end-point. Figure 2 provides a flow diagram of the study protocol. Side effects encountered are shown in Table 1. Table 2 depicts numerical data of headache parameters.

Overall headache parameters comparing baseline (time point 1) to study end-point (time point 2)

Flow diagram showing protocol from screening to end of study
Discussion
To our knowledge, this is the first fixed dose ranging study designed specifically to address this issue employing a simple and straightforward clinical approach. Here, we show that a low daily dose of 25 mg of topiramate was equally effective as 50, 75 and 100 mg in reducing headache frequency. Two early published studies on topiramate prophylaxis have been conducted in the Western population. The first study [1] assessed topiramate against placebo had found responder rates (50% reduction in headache frequency) at 39% (50 mg/day), 49% (100 mg/day) and 47% (200 mg/day). However, it is comparable to our study only for headache days, which were significantly reduced for the 100 and 200 mg/day groups only. Another study [2], employing a similar placebo-controlled protocol, reported fairly similar findings. However, headache days were not an outcome measure in this particular study.
Our findings can be compared to a previous study comprising only Chinese patients [7], which found that some patients appeared to benefit with doses as low as 25 mg/day, despite the mean dose being 80 mg for that entire study which had employed a physician-led upward dose titration depending on clinical response. As the end results of this and our study were contributed by Chinese patients, it is likely that differences in outcomes were due to methodological variation. It should be noted that this study was based on an escalating dose titration determined by the treating physician depending on clinical response, and concomitant prophylactic medications were allowed. A second Asian study comprising Indian patients had employed topiramate at 50 mg/day in a 4-week crossover protocol [6]. In this study, topiramate was administered at a fixed dose of 50 mg/day for only 4 weeks in a crossover design with lamotrigine. These vital differences likely contributed to incomparable findings with our study. To this end, we are of the opinion that a fixed daily dosing regimen would offer maximal practicality and convenience both for the patient and the treating physician.
In terms of adverse events, paresthesia was by far the most common. Its incidence was increased with higher dosages, as previously noted in other studies [11, 12]. The other adverse events occurred in fairly similar frequencies across the four dosing groups. Hence, lower dosages may potentially benefit patients in terms of better compliance as a result of lower side effect occurrences. In addition, lower dosage requirements may also imply cost savings for the patient. As Asians display clinically different pharmacology compared to Western patients, its is likely that our findings of lower dosage requirements can be explained by these physiological factors [13, 14].
In conclusion, our novel findings highlighting efficacy of a fixed low dose of topiramate of 25 mg/day in migraine prophylaxis also attest to advantages in terms of reduced cost and favourable side effect profile.
References
Terwindt GM, Ferrari MD, Tijhuis M, Groenen SM, Picavet HS, Launer LJ (2000) The impact of migraine on quality of life in the general population: the GEM study. Neurology 55:624–629 1:STN:280:DC%2BD3cvpslKhtA%3D%3D, 10980723
Silvestrini M, Bartolini M, Coccia M, Baruffaldi R, Taffi R, Provinciali L (2003) Topiramate in the treatment of chronic migraine. Cephalalgia 23:820–824 10.1046/j.1468-2982.2003.00592.x, 1:STN:280:DC%2BD3svkvFOiug%3D%3D, 14510929
Silberstein SD, Neto W, Schmitt J, Jacobs D, MIGR-001 Study Group (2004) Topiramate in migraine prevention: results of a large controlled trial. Arch Neurol 61:490–495 10.1001/archneur.61.4.490, 15096395
Brandes JL, Saper JR, Diamond M, Couch JR, Lewis DW, Schmitt J, Neto W, Schwabe S, Jacobs D, MIGR-002 Study Group (2004) Topiramate for migraine prevention: a randomised controlled trial. JAMA 291:565–573 10.1001/jama.291.8.965
Lee ST, Chu K, Park JE, Park HJ, Park JH, Lee SH, Kim M (2007) Paresthesia as a favourable predictor of migraine prophylaxis using topiramate. Eur J Neurol 14:654–658 10.1111/j.1468-1331.2007.01804.x, 17539944
Gupta P, Singh S, Goyal V, Shukla G, Behari M (2007) Low-dose topiramate versus lamotrigine in migraine prophylaxis (the Lotolamp study). Headache 47:402–412 17371357
Li HL, Kwan P, Leung H, Yu E, Tsoi TH, Hui AC, Sheng B, Lau KK (2007) Topiramate for migraine prophylaxis among Chinese population. Headache 47:616–619 17445114, 10.1111/j.1526-4610.2007.00763_3.x
Ashtari F, Shaygannejad V, Akbari M (2008) A double-blind, randomized trial of low-dose topiramate vs propanolol in migraine prophylaxis. Acta Neurol Scand 118:301–305 10.1111/j.1600-0404.2008.01087.x, 1:CAS:528:DC%2BD1cXhsVWju7rL, 18713156
Shaygannejad V, Janghorbani M, Ghorbani A, Ashtary F, Zakizade N, Nasr V (2006) Comparison of the effect of topiramate and sodium valproate in migraine prevention: a randomized blinded crossover study. Headache 46:642–648 10.1111/j.1526-4610.2006.00413.x, 16643559
Headache Classification Committee of the International Headache Society (1998) Classification and diagnostic criteria for headache disorders, cranial neuralgia and facial pain. Cephalalgia 8:1–96
Silberstein SD (2005) Topiramate in migraine prevention. Headache 45:S57–S65 10.1111/j.1526-4610.2005.4501005.x, 15833091
Storey JR, Calder CS, Hart DE, Potter DL (2001) Topiramate in migraine prevention: a double-blind, placebo-controlled study. Headache 41:968–975 10.1046/j.1526-4610.2001.01190.x, 1:STN:280:DC%2BD387mvFymtw%3D%3D, 11903524
Korean Topiramate Study Group (1999) Topiramate in medically intractable partial epilepsies: double-blind placebo-controlled randomized parallel group trial. Epilepsia 40:1767–1774 10.1111/j.1528-1157.1999.tb01596.x
Lim SH, Kwan HC, Sjahrir MJ (2001) An open label trial of topiramate as adjunctive therapy in Asian patients with refractory partial epilepsy. Neuro J Southeast Asia 6:121–127
Acknowledgments
This study was supported by a grant from Johnson & Johnson Pharmaceuticals.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Lo, Y.L., Lum, S.Y., Fook-Chong, S. et al. A pilot study of topiramate dosages for migraine prophylaxis in an Asian population. J Headache Pain 11, 175–178 (2010). https://doi.org/10.1007/s10194-010-0193-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10194-010-0193-4