
Abstract
Background
We sought to determine whether subjective outcomes one or more years after antireflux surgery are affected by the operating surgeon.
Methods
We reviewed records of patients who had antireflux surgery from June 2000 to June 2002 and mailed the patients a 19-item survey that focused on current medication use, postoperative symptom improvement, and satisfaction with surgery. We tested the significance of predictor variables using chi-squared and Fisher exact tests for categorical variables and analysis of variance for continuous variables.
Results
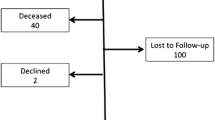
We mailed the survey to 74 patients. Ninety-one percent of the operations were initially laparoscopic, with 5 (7%) subsequently converting to open. Ninety-five percent of patients were taking protein pump inhibitors (PPIs) preoperatively. Surgeons (n = 7) were divided into four groups, with the four surgeons who did two or fewer procedures in one group. Fifty-two of 74 patients (70%) responded to the survey (mean age, [SD] 44 [21] years, 37% male). The mean duration of followup was 2.1 [0.46] years. Thirty-eight percent of patients were taking medications for gastroesophageal reflux disease at the time of survey completion. It was found that the surgeon had an influence on patients’ perceptions of the success of the surgery and whether having surgery was a good idea. We did not identify a statistically significant effect of the surgeon on preoperative symptom severity, postoperative ability to belch, dysphagia, medication use, and lifestyle.
Conclusion
A patient’s surgeon has an effect on satisfaction with antireflux surgery. Further research should clarify specific practices of the surgeon (patient selection, operative technique, followup) associated with best outcome.
Similar content being viewed by others


References
Barnett HJ, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes RB, Rankin RN, Clagett GP, Hachinski VC, Sackett DL, Thorpe KE, Meldrum HE, Spence JD (1998) Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med 339(20): 1415–1425
Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE, Lucas FL (2003) Surgeon volume and operative mortality in the United States. N Engl J Med 349(22): 2117–2127
Deschamps C, Allen MS, Trastek VF, Johnson JO, Pairolero PC (1998) Early experience and learning curve associated with laparoscopic Nissen fundoplication. J Thorac Cardiovasc Surg 15(2): 281–284
Herrmann D (1995) Reporting current, past and changed health status. What we know about distortion. Med Care 33: AS89–AS94
Hinder RA, Filipi CJ, Wetscher G, Neary P, DeMeester TR, Perdikis G (1994) Laparoscopic Nissen fundoplication is an effective treatment for gastroesophageal reflux disease. Ann Surg 220(4): 472–481
Howden C, Castell D, Cohen S, Freston JW, Orlando RC, Robinson M (1995) The rationale for continuous maintenance treatment of reflux esophagitis. Arch Intern Med 155: 1465–1471
Klapow JC, Wilcox CM, Mallinger AP, Marks R, Heudebert GR, Centor RM, Lawrence W, Richter J (2002) Characterization of long-term outcomes after Toupet fundoplication: symptoms, medication use, and health status. J Clin Gastroenterol 34(5): 509–515
Liu JY, Woloshin S, Laycock WS, Schwartz LM (2002) Late outcomes after laparoscopic surgery for gastroesophageal reflux. Arch Surg 137: 397–401
Luostarinen ME, Isolauri JO (1999) Surgical experience improves the long-term results of Nissen fundoplication. Scand J Gastroenterol 34(2): 117–120
Sato K, Awad ZT, Filipi CJ, Selima MA, Cummings JE, Fenton SJ, Hinder RA (2002) Causes of long-term dysphagia after laparoscopic Nissen fundoplication. JSLS 6(1): 35–40
Soot SJ, Eshraghi N, Farahmand M, Sheppard BC, Deveney CW (1999) Transition from open to laparoscopic fundoplication: the learning curve. Arch Surg 134(3): 278–281
Spechler S, Lee E, Ahnen D, Goyal RK, Hirano I, Ramirez F, Raufman JP, Sampliner R, Schnell T, Sontag S, Vlahcevic ZR, Young R, Williford W (2001) Long-term outcome of medical and surgical therapies for gastroesophageal reflux disease: follow-up of a randomized controlled trial. JAMA 285: 2331–2338
Statistics on surgery performed in the United States. Available at http://www.ahrq.gov/data/hcup/hcupnet.htm [accessed April 5, 2004]
Terry M, Smith CD, Branum GD, Galloway K, Waring JP, Hunter JG (2001) Outcomes of laparoscopic fundoplication for gastroesophageal reflux disease and paraesophageal hernia. Surg Endosc 15: 691–699
Waring JP (1999) Postfundoplication complications. Prevention and management. Gastroenterol Clin North Am 28(4): 1007–1019, viii-ix
Williams JL (2003) Gastroesophageal reflux disease: clinical manifestations. Gastroenterol Nursing 26(5): 95–200
Wu JS, Dunnegan DL, Luttmann DR, Soper NJ (1996) The influence of surgical technique on clinical outcome of laparoscopic Nissen fundoplication. Surg Endosc 10(12): 1164–1169
Author information
Authors and Affiliations
Corresponding author
Additional information
Presented in poster form at the annual meeting of the Society of American Gastrointestinal Endoscopic Surgeons (SAGES), Denver, Colorado, March 31–April 3, 2004.
This work was supported in part by the Canadian Association of General Surgeons and the physicians of Ontario through the Physicians’ Services Incorporated Foundation. Dr. Urbach is a Career Scientist of the Ontario Ministry of Health and Long-Term Care, Health Research Personnel Development Program.
Rights and permissions
About this article
Cite this article
Kundhal, P.S., Harnish, J.L. & Urbach, D.R. Effect of surgeon on outcome of antireflux surgery. Surg Endosc 21, 902–906 (2007). https://doi.org/10.1007/s00464-006-9024-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-006-9024-8