
Abstract
In the recent years, considerable insight has been gained in to the optimal management of adult asthma. Most adult patients with asthma have mild intermittent and persistent disease, and it is acknowledged that many patients do not reach full control of all symptoms and signs of asthma. Those with mild persistent asthma are usually not well controlled without inhaled corticosteroids (ICS). Studies have provided firm evidence that these patients can be well controlled when receiving ICS, especially when disease is of recent onset. This treatment should be given on a daily basis at a low dose and when providing a good response should be maintained to prevent severe exacerbations and disease deterioration. Intermittent ICS treatment at the time of an exacerbation has also been suggested as a strategy for mild persistent asthma, but it is less effective than low-dose regular treatment for most outcomes. Adding a long-acting beta-agonist (LABA) to ICS appears to be unnecessary in most of these patients for optimising control of their asthma. Patients with moderate persistent asthma can be regarded as those who are not ideally controlled on low-dose ICS alone. The combination of an ICS and LABA is preferred in these patients, irrespective of the brand of medicine, and this combination is better than doubling or even quadrupling the dose of ICS to achieve better asthma control and reduce exacerbation risks. An ICS/LABA combination in a single inhaler represents a safe, effective and convenient treatment option for the management of patients with asthma unstable on inhaled steroids alone. Ideally, once asthma is under full control, the dose of inhaled steroids should be reduced, which is possible in many patients. The duration of treatment before initiating this dose reduction has, however, not been fully established. One of the combinations available to treat asthma (budesonide and formoterol) has also been assessed as both maintenance and rescue therapy with a further reduction in the risk for a severe exacerbation. Clinical effectiveness in the real world now has to be established, since this approach likely improves compliance with regular maintenance therapy.
Similar content being viewed by others


Introduction
Asthma affects 300 million people worldwide (Masoli et al. 2005), with an increasing prevalence in Western Europe and the USA in particular. International guidelines stipulate goals for optimising asthma management, such as preventing chronic and acute symptoms, minimising exacerbations and emergency care, minimising the use of rescue β2-agonists and maintaining normal levels of physical activity (Global Initiative for Asthma 2004). Much has been learned in the past 25 years with regard to asthma management. Despite the fact that there is still no cure for asthma, it has been established in a great number of small and large studies that many patients can reach a good asthma control with controller treatment (Global Initiative for Asthma 2004). This can be reached by combining inhaled corticosteroids (ICS) and long-acting β2-agonists (LABA), which is the mainstay of current asthma treatment. The current paper describes the place of particularly these two types of drugs and their combination in the management of mild to moderate persistent severe asthma in particular, which constitutes the largest group of asthma patients.
Asthma management with inhaled corticosteroids only
The therapeutic options available for patients with asthma depend on the severity of the condition (Global Initiative for Asthma 2004). Generally, asthma is divided into mild intermittent, mild persistent, moderate persistent and severe persistent disease, based on respiratory symptoms, nocturnal awakening due to symptoms and the severity of airway obstruction (Table 1; Global Initiative for Asthma 2004).
ICS are the most efficacious therapy currently available for optimal asthma management, and they are prescribed to most patients with asthma (see www.ginasthma.org, entered December 2007). When short-acting beta-2-agonists are insufficiently reducing symptoms, i.e. to less than once a day, ICS are advocated as the next step in the management of newly diagnosed asthma to reach the control of symptoms and signs of asthma. If this does not occur, then a LABA is recommended as additional treatment in the management of asthma. ICS control symptoms, improve hyperresponsiveness and lung function, reduce the number of exacerbations and improve health status in most patients irrespective of the severity of their disease (Barnes 2006). Both short-term and long-term studies have shown that inhaled steroids are efficacious in asthma management. Some effects occur shortly after initiation of the treatment, while other effects increase with time of treatment. For instance, ICS improve hyperresponsiveness to a larger extent with longer duration of treatment (Kerstjens et al. 1992) and preserve the initial lung function improvement when given for long periods of treatment (Douma et al. 2002; Kerstjens et al. 1992). Long-term studies also suggest that inhaled steroids reduce the accelerated decline in lung function, which is now acknowledged to be present in a subset of asthma patients (Dijkstra et al. 2006; Lange et al. 1998).
Given these assets of inhaled steroids in asthma management, ICS are the first-line therapy for all patients who use a β2-adrenoceptor agonist inhaler more than once a day, and this is reflected in all national and international guidelines for asthma management (Global Initiative for Asthma 2004; Lemiere et al. 2004; NHLBI 2002). The efficacy of ICS is due primarily to the suppression of virtually every step in the inflammatory cascade that underlies the airway disease in asthma and the associated airway hyperresponsiveness that is present in most asthma patients. Acting via the glucocorticoid receptor, ICS repress the expression of inflammatory cytokines, their receptors, adhesion molecules and other disease-inducing mediators. These effects of ICS and their ability to promote apoptosis of many cell types including the eosinophil act to reduce the attraction and activation of inflammatory cells in the lungs, thereby attenuating inflammation (Barnes 2001). Furthermore, ICS suppress the pro-inflammatory activity of airway epithelial and smooth muscle cells, resident cells with an important pro-inflammatory capacity (Barnes 1996; Panettieri 2004). Since these cells produce chemokines, cytokines and pro-fibrotic mediators, they are no longer innocent bystanders in the inflammatory process and have become important additional targets for the anti-inflammatory actions of ICS (Barnes 1996).
All types of ICS monotherapy achieve successful control of persistent asthma in a significant proportion of patients (Adams and Jones 2006). Several studies have shown that inhaled steroids are effective in mild intermittent asthma or newly diagnosed mild asthma. Generally, the dose–response curve of ICS is relatively flat for a number of outcome measures, and for many patients, the therapeutic benefits of high-dose ICS above low-dose or medium-dose ICS may be marginal, thus most of the benefit in mild-to-moderate severity disease is gained in the low-to-moderate dose range of each drug. Furthermore, many studies have shown (Adams and Jones 2006; van der Molen et al. 1998) that for patients who require ICS, starting with a moderate dose is as effective as starting with a high dose and stepping down. Individual patients with severe persistent asthma my gain some benefit from high-dose ICS treatment.
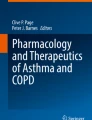
A large, 3-year double-blind study (called START, Pauwels et al. 1998) assessed whether early intervention with inhaled ICS (400 μg budesonide) prevented clinical progression of asthma in newly diagnosed, mild persistent disease (mean forced expiratory volume in 1 s [FEV1] 86% predicted and an average of 4 days with symptoms per week). These patients were newly diagnosed with asthma and had never been treated with inhaled steroids previously. The primary outcomes were the time to first very severe exacerbation (hospital visit or admission) and decline in post-bronchodilator FEV1. During the first year, approximately 34% of the patients treated with placebo needed ICS, and 4% had a severe exacerbation, compared with 20% that needed additional treatment and 2% with a severe exacerbation in the budesonide treated individuals (Fig. 1; Pauwels et al. 2003).

Proportion of events in mild asthma patients who were steroid naïve and treated with inhaled steroids (Pauwels et al. 2003)
Differences were maintained until the end of the 3-year follow-up (50% and 6% with placebo versus 30% and 3% with ICS, respectively; Pauwels et al. 2003). Decline in post-bronchodilator FEV1 was significantly larger in the placebo arm, though differences were small during this 3-year follow-up. Thus, early intervention with low-dose ICS prevented clinical progression of asthma.
Finally, one study assessed whether intermittent short-course ICS treatment, guided by a symptom-based action plan, alone or in addition to daily treatment with budesonide was more effective during 1-year treatment (Boushey et al. 2005). A third arm used the anti-leukotriene zafirlukast. The authors concluded that patients with mild persistent asthma, who were of similar severity as the START study (Pauwels et al. 2003), could be treated with intermittent courses of inhaled or oral corticosteroids in conjunction with an action plan. Indeed, the number of patients with a severe asthma exacerbation did not differ between the groups. However, numbers were low and lower than in previous studies, and follow-up was only 1-year, making it difficult to find a potential effect of either drug regimen on severe asthma exacerbation rates (total number of patients included 225). Thus, a likely better conclusion of this study is that regular inhaled steroid use is preferable, since regular use of inhaled budesonide was significantly better than intermittent use in improvement of pre-bronchodilator FEV1, asthma control scores, number of symptom-free days, airway hyperresponsiveness and markers of airway inflammation.
Prediction of beneficial response to inhaled steroids alone
It is interesting to note that some studies have investigated which factors contribute to the efficacy of instituting ICS in asthma. The most consistent beneficial factors for improvement in lung function or hyperresponsiveness are a shorter duration of asthma before treatment (Fujimoto et al. 2006), non-smoking (Fujimoto et al. 2006; Kerstjens et al. 1993; Kerstjens et al. 1995; Pedersen et al. 2007), male gender (Green et al. 2002a), better reversibility of airway obstruction (Kerstjens et al. 1993; Martin et al. 2007), sputum eosinophilia (Fujimoto et al. 2006), and higher serum IgE levels (Kerstjens et al. 1993). One study showed that short-term responders (i.e. increase of greater than 5% in FEV1 in 6 weeks) had also a long-term response when ICS were continued, supporting that lung function improvement when monitored should trigger physicians to encourage their patients to continue using inhaled steroid (Martin et al. 2007).
Asthma management with long-acting β-agonists alone?
Inhaled β2-agonists are powerful agents used to relieve the bronchoconstriction associated with asthma. By far, the most important action is stimulating the β2-receptors located in airway smooth muscle resulting in smooth muscle relaxation (Nelson 2006). This article will only deal with LABA. LABA provide longer symptom control, which is a particularly useful feature for preventing night-time symptoms. There are two main LABA, i.e. salmeterol and formoterol. Salmeterol is highly lipophilic and diffuses through the lipid bi-layer in muscle cell membranes to reach the β2-receptors, explaining the slower onset and long duration of action (Nelson 2006). Formoterol, being less lipophilic, has a faster onset of action, similar to short-acting β2-agonists, and is believed to be incorporated into the lipid bi-layer to serve as a reservoir, accounting for its prolonged action (Nelson 2006).
Frequent use of short-acting β-agonists or LABA generally indicates a significant inflammatory process that should be controlled with anti-inflammatory drugs such as ICS. The role of LABA in the management of asthma has previously been debated. The role of LABA monotherapy was specifically addressed in a study called Salmeterol Off CorticoSteroids (Lazarus et al. 2001). Subjects with mild persistent asthma were first treated with an ICS, triamcinolone acetonide (TAA) 400 μg twice daily for 6 weeks. The 164 patients whose asthma became well controlled were then randomised for 16 weeks to continue on TAA, to receive instead the LABA salmeterol (42 μg bi-daily [b.i.d.]) or placebo. While asthma control deteriorated in those placed on placebo, there was no difference between those continuing on ICS and those receiving LABA monotherapy for conventional clinical outcomes such as morning and evening peak expiratory flow (PEF), symptom scores, rescue albuterol use or quality of life. Patients who continued on salmeterol had, however, a similar rate of treatment failures and asthma exacerbations compared to those switched to placebo and a significantly higher rate than patients with ongoing steroid use. Furthermore, a difference in markers of airway inflammation developed, i.e. stable inflammatory markers in patients using ICS, whereas in those on salmeterol alone, there was deterioration in sputum eosinophils, eosinophil cationic protein, exhaled nitric oxide and methacholine sensitivity, similar to the changes seen in the placebo group. The fundamental message from this study was “The findings indicate that salmeterol should not be used as monotherapy for treatment of persistent asthma...” (Lazarus et al. 2001).
At present, the use of LABA as monotherapy clearly appears to be less effective than ICS alone (Lazarus et al. 2001; Nelson et al. 2006) and has been associated with increased asthma deaths in two post-marketing surveillance studies in the USA and UK (Castle et al. 1993; Nelson et al. 2006). An increased risk of respiratory-related mortality or life-threatening events occurred with salmeterol compared with placebo in a population of patients with asthma (Nelson et al. 2006), and these differences were significant for the African-American subset of study participants. The findings were in accordance with a study undertaken in the UK (Castle et al. 1993) in which numerically higher (though not significantly) numbers of asthma-related deaths were recorded with regular use of salmeterol. The population in the US surveillance study had, in general, very poorly controlled asthma, yet less than 50% of these patients reported being treated with ICS. The African-American population had even less well-controlled asthma, with lower lung function and an even lower proportion of patients prescribed ICS. In a meta-analysis of the LABA data, Salpeter et al. (2006) performed a search of databases up to the end of 2005 to assess the risk for severe, life-threatening or fatal asthma exacerbations associated with the use of LABA. They limited their search to placebo-controlled trials that lasted at least 3 months. The results reported for fatal and near-fatal asthma attacks largely repeated the previously published data of increased numbers of near-fatal asthma with LABA treatment from the Symbicort as Maintenance And Reliever Therapy (SMART) study (Nelson et al. 2006). In the discussion, the authors suggest that the LABA use may be responsible for the increased asthma mortality since 1960. However, as Nelson pointed out (see comments in review), asthma mortality was steadily declining in the USA since the introduction of LABA, and most studies analyzed did not require concomitant use of inhaled steroids. In a recent overview of the safety of LABA in asthma, two new more extensive meta-analyses (20,592 subjects and 6,988 subjects, as yet only available in abstract form (Oppenheimer and Nelson 2008), were discussed that showed a significant reduction in exacerbations when ICS was used in combination with LABA, as well as the risk for hospitalisation.
The data to date available suggest that a small sub-class of asthmatics may be prone to deleterious effects of LABA. However, from the data available, it cannot be ascertained whether this is some rare susceptibility to a deleterious effect of LABA or that this is the consequence of monotherapy with LABA that controls the symptoms but may mask increasing inflammation in patients who lack adequate access to medical care. Therefore, all national and international asthma consensus statements recommend the use of LABA only in combination with ICS (Masoli et al. 2005; Global Initiative for Asthma 2004). The Medicines and Healthcare Products Regulatory Agency Safety Update on LABA in the UK has also recently concluded that at present, the benefits of LABA outweigh the risk, and it is important that patients take their asthma medicine as prescribed, and this should be in conjunction with ICS (http://www.mhr.gov.uk/Safetyinformation/Generalsafetyinformationandadvice/Productspecificinformationandadvice/Asthma/index.htm).
Clinical evidence suggesting an anti-inflammatory action of LABA when added to ICS
The first clinical suggestion that LABA might be more than just a bronchodilator when they are added to an ICS came with the Formoterol And Corticosteroids Establishing Therapy (FACET) landmark study (Pauwels et al. 1998). Eight-hundred and fifty-two patients with asthma were first treated for 4 weeks with 800 μg of budesonide twice daily. They were then randomised to either budesonide 100 or 400 μg twice daily, and half in each group received additional formoterol 12 μg twice daily for 1 year. As anticipated, all the conventional measures of asthma control, pulmonary function, symptoms and rescue albuterol use were improved by the addition of formoterol to either dose of budesonide. What was not anticipated was that the addition of formoterol to either dose of budesonide reduced the occurrence of asthma exacerbations—both minor exacerbations and those requiring prednisone treatment. A meta-analysis examining the addition of salmeterol to low-dose ICS as compared to at least doubling the dose of ICS confirmed the findings of FACET; that is, the addition of a LABA produces a greater reduction in exacerbations than the higher dose of ICS (Shrewsbury et al. 2000). Exacerbations of asthma are considered to reflect ongoing airway inflammation, and hence a reduction in the exacerbation rate with a drug is considered (indirect) evidence of its anti-inflammatory activity. Direct clinical evidence for some anti-inflammatory activity of LABA when added to ICS has also been sought. In three studies, there was a significant anti-inflammatory effect (e.g. a reduction in numbers of eosinophils and mast cells) seen with the combination of an inhaled steroid and salmeterol, which was not seen with the same dose of inhaled steroid alone, or in two cases with a considerably higher dose of inhaled steroid alone (Koopmans et al. 2006; Li et al. 1999; Wallin et al. 2003). In mild disease (Kips et al. 2000), the addition of formoterol to budesonide showed comparable effects on sputum eosinophils as the treatment with a higher dose of ICS. A more recent study, however, found a more pronounced reduction in sputum inflammatory cells with a high-dose budesonide than with the addition of formoterol to a low dose of inhaled budesonide (Green et al. 2006).
Combination of LABA and ICS in daily treatment: the first studies
Greening et al (1994) conducted the first double-blind, parallel group trial of 6-month duration in 426 asthmatic subjects who were symptomatic despite maintenance therapy with the ICS, beclomethasone dipropionate (BDP; 200 μg b.i.d.). Subjects were randomised to receive salmeterol xinafoate (50 μg b.i.d.) and BDP (200 μg b.i.d.) delivered via separate inhaler devices or BDP alone at a higher dose of 500 μg b.i.d. Both treatment interventions significantly improved mean morning PEF, but the LABA/ICS combination therapy was superior at all time points. Other end points that favoured salmeterol/BDP over high-dose BDP alone included diurnal variation in PEF, daytime and night-time symptoms and rescue bronchodilator use. There was no significant difference in the exacerbation rate between the two treatment groups indicating that salmeterol, given chronically with BDP, was not associated with any risk of asthma deterioration over the duration of the study. However, there was no protective effect in this study on exacerbation rates. Except for exacerbation rates and morning PEF, the addition of salmeterol to a standard dose of BDP was more effective clinically than increasing, by 2.5-fold, the dose of BDP (Greening et al. 1994).
The clinical significance of these finding was endorsed further when the landmark FACET study established that combination therapy was also clinically superior to glucocorticoid alone when exacerbation rate was used as the primary outcome measure (Pauwels et al. 1998). Indeed, the exacerbation rate in subjects with moderately severe asthma was lower when the LABA, formoterol (9 μg b.i.d.), was added to low and high doses of another glucocorticoid, budesonide (that is 100 or 400 μg b.i.d.), when compared to the ICS alone (Pauwels et al. 1998). This study also showed that a fourfold boost of ICS improved all outcomes, apart from severe exacerbations. Other studies have subsequently shown that a twofold rise in the dose of ICS was not effective in asthma management for most outcomes assessed, including the reduction in the rate of asthma exacerbations or the prevention of exacerbations (O’Byrne and Parameswaran 2006).
Confirmation of effects: superiority of LABA/ICS combination therapy as a class effect
Since the seminal report of Greening et al. (1994), many trials have been conducted comparing the clinical effectiveness in asthma of LABA/ICS combination therapies in separate inhaler devices with a higher dose of an ICS alone. Most studies concerned mild to moderate severe asthma, and predominantly moderately severe asthma patients were included in these studies. What has emerged, unambiguously, is that the clinical superiority of salmeterol and BDP in combination over higher-dose ICS alone is unequivocal and class specific (that is, it is not limited to salmeterol or BDP but a generic effect of LABA and ICS when used in combination). Indeed, meta-analyses of nine parallel group trials in which the clinical efficacy and safety of salmeterol in combination with either BDP or fluticasone were assessed and compared to a higher dose of ICS given as a monotherapy led Shrewsbury et al. (2000) to conclude that “....giving salmeterol to patients who have symptoms on at least 400 μg BDP per day will result in better lung function, better control of symptoms, less need for rescue medication, and fewer exacerbations than increased doses of inhaled steroid.”
The results of the more recent Gaining Optimal Asthma controL (GOAL) study has also confirmed the superiority of salmeterol/fluticasone in combination yet within one inhaler device in achieving greater asthma control than the ICS alone (Bateman et al. 2004). This study in predominantly moderate to severe persistent asthma (10% with mild disease) assessed how frequently ideal asthma control can be achieved. Three groups were included: steroid-naive, low-dose, and moderate-dose ICS use at study entry, and all groups were not well controlled. The study population was randomly allocated to either increasing doses of ICS alone or similar doses together with the LABA salmeterol for 1 year. Phase I of the study was dose escalation, whereby the dose was stepped up until total asthma control was achieved or until the maximum dose was reached (fluticasone 1000 μg, or fluticasone 1000 μg and salmeterol 100 μg daily). Phase II was the time after total control was achieved or after 12 weeks on the maximum dose of drug. Table 2 shows the definition of total control and well controlled in the GOAL study, compared to the Global Initiative For Asthma guidelines.
Total asthma control, defined as no symptoms, normal lung function and no limitation of activities, was achieved in less than 50% of the overall population and less than 30% of those already taking moderate doses of ICS at randomisation, even with the highest doses of combination treatment. Well-controlled asthma, defined as mild occasional symptoms (as per Table 2), was achieved in up to 78% of patients not receiving ICS before study entry and in 62% of those already on moderate doses of ICS (Fig. 2; Bateman et al. 2004). The combination of ICS and LABA was always significantly better than ICS alone. Moreover, control was reached more rapidly and at a lower ICS dose with the combination treatment. A further analysis (Woodcock et al. 2007) investigated whether the GOAL study would show similar results when single specific endpoints, as used in the guidelines (Global Initiative for Asthma 2004), were investigated. It showed that salmeterol/fluticasone treatment resulted in an additional 66 symptom-free days per year compared with fluticasone alone, and in all strata, symptom-free days and rescue-free days were more probable in patients receiving combination therapy (Woodcock et al. 2007). Again, the outcome was better after 52 weeks of treatment (during the time that patients remained on the dose at which they had achieved total control or the maximum study dose) than with 12 weeks, which is in line with the GOAL study. Moreover, it fits with previous studies that long-term treatment is needed with ICS to reach maximal reduction in airway inflammation and hyperresponsiveness (Douma et al. 2002; Dijkstra et al. 2006; Kerstjens et al. 1992; Lange et al. 1998). The GOAL study shows that recommendations by guidelines (Global Initiative for Asthma 2004) to assess patients according to their level of control and then treat them with stable dosing, followed by stepping up of treatment to achieve and maintain asthma control, is effective. However, the danger of over-treatment is not imaginary in this way when the highest dose is maintained, and asthma guidelines recommend that once asthma control has been achieved and maintained for 3–6 months, treatment should be reviewed and dose reduction attempted, with careful monitoring to ensure that control is not lost. This was not within the scope of the GOAL study; thus, treatment reduction did not take place. In a subsequent study, Bateman et al. (2006) studied stepping-down treatment in a 12-week study comparing patients who were well controlled on salmeterol/fluticasone (50/250 μg b.i.d.) for at least 4 weeks and who were then switched to either salmeterol/fluticasone 50/100 μg b.i.d. or fluticasone 250 μg b.i.d for 12 weeks. It was shown that stepping down to the combination was more effective than to fluticasone alone, with respect to PEF, symptom control and rescue albuterol use. However, still not all patients were well controlled during the stepping down of treatment; that is, 23% and 31% were not controlled when stepping down to the combination and fluticasone-alone groups, respectively. Thus, future studies have to elucidate which patients can step down safely and after which period of treatment. This is important, also in the light of the GOAL findings that with sustained treatment, more patient will achieve higher levels of control and that the achievement of control is a function of both dose and duration of treatment (Bateman et al. 2004; Bateman et al. 2006).

Well control and total control with fluticasone and fluticasone/salmeterol in the GOAL study (Bateman et al. 2004). WC Well controlled, TC total control, FP fluticasone propionate, Salm salmeterol, S severity level
The clinical superiority of LABA/ICS combination therapies also extends to subjects with moderate persistent asthma treated with budesonide combined with formoterol. This was shown in the FACET study. Furthermore, the Oxis and Pulmicort Turbuhaler In the Management of Asthma (OPTIMA) study convincingly demonstrated that adding formoterol (4.5 μg b.i.d.) to low-dose budesonide (200 μ b.i.d.) for 1 year in subjects with moderate severe asthma was more effective than doubling the dose of ICS in increasing the time to first severe asthma exacerbation (O’Byrne et al. 2001).
Of importance, a recent meta-analysis suggested that the beneficial effects of the addition of LABA to ICS depend on the outcome measures under study (Gibson et al. 2007). For instance, in steroid-naïve patients, the number of severe exacerbations was not significantly different with the addition of LABA to ICS versus ICS alone, but the outcome measured as the improvement in PEF, reduction in rescue beta-agonist use and percent of symptom-free days did improve significantly. The greatest benefit occurred when the addition of LABA to ICS was compared with continuing ICS alone in a similar dose; that is, in that way, the number needed to treat for the prevention of a severe exacerbation is 18 (Table 3; Gibson et al. 2007). Finally, a composite score of asthma control (see above for definition) was always better with LABA/ICS treatment when comparing with a similar dose in steroid-naïve patients, in patients using a similar dose of ICS and in patients with a higher ICS dose (Gibson et al. 2007).
This was also found in a further analysis of the GOAL study comparing the above composite score of control and the separate items of this score (Bateman et al. 2007). The composite score of control took, as expected, always longer to be reached than the individual items. Night-time awakening responded most rapidly, and daytime symptoms took longest to respond. Again, the response was always better with LABA/ICS treatment than ICS treatment alone yet with one exception. Night-time awakening had a more rapid response following treatment with fluticasone alone, a finding that was unexpected and not easy to explain given the fact that salmeterol provides bronchodilation for a period that covers the nigh-time setting. Moreover, both treatments contained an ICS, which reduces persistent airway inflammation that is similarly present at day and night in patients with nocturnal awakenings (ten Hacken et al. 1998). Notwithstanding the more rapid control of night-time awakening with fluticasone, LABA/ICS combination provided again a better control at the end of 12 weeks (Table 4; Nelson et al. 2000). An important message of the study is that using any of the individual criteria of control in isolation will over-estimate a patient’s level of overall control (Table 4; Nelson et al. 2000). Moreover, to establish full control, a longer duration of treatment is necessary, supporting the conclusion of the initial GOAL study (Bateman et al. 2006).
No confirmation of superiority of LABA/ICS combination therapy in mild disease
Patients with mild persistent asthma form a sizable proportion of people with asthma (up to 70%; O’Byrne and Parameswaran 2006). Nevertheless, they are frequently unknown to their physician since they rarely visit their family doctor with symptoms of the disease and are seldom seen in a secondary or tertiary healthcare setting.
Few studies have allowed assessing whether treatment approaches with combined LABA/ICS are effective above ICS alone in mild persistent asthma. O’Byrne recently summarised these studies (O’Byrne and Parameswaran 2006). The OPTIMA study is one of them and allowed to study mild persistent asthma separately from moderate severe asthma (O’Byrne et al. 2001). The mild persistent asthma group consisted of almost 700 individuals who had never used ICS. In this group, budesonide alone (200 μg/day) was compared with the same dose of budesonide plus formoterol or budesonide plus placebo for 1 year of treatment. The primary outcome was rate of severe asthma exacerbations; this rate was 0.77 per patient per year in the placebo-treated group, falling to 0.29 per patient per year with low-dose budesonide alone. All other study outcomes, including days with asthma symptoms and nights with nocturnal symptoms, were also improved by budesonide treatment. The combination of budesonide and formoterol did not provide any additional benefit when compared with budesonide alone. Thus, for patients with mild persistent asthma, low-dose ICS alone are the preferred treatment option. By contrast and confirming earlier studies, patients with moderate persistent asthma who used ICS at study entry did show a striking and significant difference in asthma exacerbations when formoterol was added to budesonide (Fig. 3; Pauwels et al. 1998, O’Byrne et al. 2001). The findings suggest that combination treatment is not appropriate for all patients with persistent asthma and that benefit is only seen in those not ideally controlled on low doses of ICS alone.

Delivery of LABA/ICS combination therapies by a single-inhaler device
Following confirmation of the efficacy and safety of LABA and ICS administered in combination by separate-inhaler devices, a number of studies were performed comparing the efficacy and safety of salmeterol/fluticasone (Seretide/Advair; GlaxoSmithKline, Stevenage, UK) and formoterol/budesonide (Symbicort; AstraZeneca, Lund, Sweden) delivered by single-inhaler devices (Miller-Larsson and Selroos 2006). The combination of two complementary treatments in one inhaler has the advantage that it simplifies the management of asthma patients. Although differences in the effectiveness of the combination therapies between the different methods of administration were reported in some studies, the balance of evidence demonstrates similar efficacy and safety profiles irrespective of whether the components of the combination were delivered in single or separate inhalers (FitzGerald et al. 2003; Ind et al. 2004; Nelson et al. 2003; Price et al. 2007; Zetterström et al. 2001, Pohl et al. 2006, Lundborg et al. 2006).
Formoterol/budesonide as a maintenance and rescue therapy—a Symbicort SMART approach to asthma management
Despite aggressive fixed-dose combination therapy with ICS and LABA, a proportion of patients with asthma remains sub-optimally controlled, based on the need for rescue therapy and rates of severe exacerbations. Therefore, studies were set up to assess whether the regular use of the combination of budesonide and formoterol in one inhaler (so-called maintenance treatment) could also be used as rescue therapy (O’Byrne et al. 2005; Rabe et al. 2006a; Scicchitano et al. 2004). This approach is possible because formoterol is an inhaled β2-agonist that has a rapid onset and a long duration of action and can thus be used as a rescue therapy instead of a separate short-acting β2-agonist (Ringdal et al. 2003). Moreover, it has a significant dose-dependent increase in lung function with increasing doses of 6, 12, 24 and 46 μg (Ringdal et al. 1998). The strategy of combined maintenance and rescue treatment was compared in one study (O’Byrne et al. 2005) with a fourfold higher dose of ICS as maintenance and a short-acting β2 agonist as rescue during 1-year follow-up. Patients enrolled were adults and children with moderate to severe asthma. Findings of this study show that the use of this combination as both maintenance and rescue greatly reduces risk for severe asthma exacerbations when compared with other approaches (Fig. 4), with an associated reduction in oral corticosteroid use.

Outcome of SMART treatment versus fixed dose budesonide/formoterol or budesonide. PEF Peak expiratory flow, ER emergency room
This is of importance, since the FACET study (Pauwels et al. 1998) showed that the only benefit of a fourfold increase in inhaled steroid dose, used as a maintenance treatment, was the reduction in severe exacerbations. This study (O’Byrne et al. 2005) thus shows that a similar benefit can be reached when using a lower cumulative dose of inhaled steroids, yet using the formoterol/budesonide inhaler as a maintenance and rescue treatment. An unexpected finding was that this so-called SMART approach was that it did not only markedly reduce the number of severe exacerbations requiring medical attention (the primary outcome measure) throughout the 1-year treatment period. It is interesting to note that it also reduced the need for oral corticosteroids and improved symptom control including nocturnal awakenings and lung function compared with terbutaline for relief and either budesonide/formoterol or a fourfold higher dose of budesonide for maintenance therapy. A concern about this approach is that some patients might end up using the combination inhaler frequently and receive an unacceptably high dose of ICS. However, this was not the case, as the mean number of additional doses of combination inhaler was only one dose per day and very few patients required high doses.
A further study compared this approach with formoterol/budesonide- versus budesonide-adjustable dosing twice daily (Rabe et al. 2006a). Again, both treatments proved effective, and there were few treatment failures in either group. The majority received extra reliever medication on only 0.7% of the study days, and this was better with the LABA/ICS treatment; that is, 50% of the patients used only 1-day reliever treatment for 5 months, whereas this was 6 days in the budesonide-adjustable maintenance dosing group. Furthermore, the adjustable dosing provided better health-related quality of life and better patient satisfaction, despite a lower average daily ICS dose, i.e. 448 versus 1,152 μg/day in the budesonide group.
Thus, for some patients who need a maintenance treatment with a combination inhaler containing budesonide and formoterol, the inhaler can also be used as rescue when needed, thereby allowing patients to manage their asthma with one inhaler. One study showed that the budesonide component was needed to obtain the beneficial role (Rabe et al. 2006b), since the formoterol/budesonide rescue treatment reduced the number of severe exacerbations by 33% over formoterol as needed, both in addition to the maintenance treatment with formoterol/budesonide. This was, however, not due to a higher dose of budesonide used, since there was only a very modest increase in the ICS dose for the formoterol/budesonide SMART approach. It likely happened because of the early administration of the ICS, given as part of the rescue treatment at the time of worsening asthma control. Apparently, asthmatic patients are able to detect worsening of asthma quite early. This is in line with the findings in the FACET study (Tattersfield et al. 1999), showing that exacerbations are not explosive events, as previously believed, but evolve slowly over several days until the clinical worsening prompts the introduction of oral corticosteroids with/without antibiotics. Of importance is that the patients were able to reach this level of asthma control without any help of their physician but managed independently to adjust their treatment to the rapid variability of their disease. Finally, this novel treatment approach reduced both ICS and oral corticosteroid exposure, with a similar or reduced effect on morning plasma cortisol and adrenal function, compared with budesonide 800 μg/day (O’Byrne et al. 2005; Scicchitano et al. 2004).
The above studies pertain to moderate to severe asthma patients not well controlled on ICS alone. Only when patients were poorly controlled on low-dose or high-dose ICS and LABA therapy were they randomised in the above studies, and the authors gave the message that the results “should not be extrapolated to patients with intermittent asthma, however, or to those well controlled on ICS alone” (Rabe et al. 2006b). These patients can do well on the treatment they have at that time.
Prediction of beneficial response to LABA + ICS as initial maintenance therapy
It has been clearly shown that adding a LABA to ICS is more beneficial than increasing the dose of ICS with respect to clinical symptom relief in patients with all but mild asthma. However, not all patients respond equally well. Ernst et al. (2008) therefore investigated which patients might respond better to initial therapy with the combination or with ICS alone. Data from five randomised clinical trials were pooled to investigate this. Overall, the trials in moderate to severe asthma patients (daily symptoms in 71%, greater than or equal to two nights awakening per week in 42%) showed that patients were 1.8 times more likely to achieve well-controlled asthma within 12 weeks with combination therapy than with fluticasone alone. The benefit increased in subjects reporting a duration of asthma of 10 years or more to a level of 2.2 times. None of the other factors assessed, i.e. symptom frequency or severity, rescue beta-agonist use, severity of lung function impairment or degree of reversibility, was able to distinguish patients who would benefit more than average from the combination LABA/ICS treatment compared with the ICS treatment alone. The study did not assess the number of exacerbations, for which the follow-up time of 12 weeks was too short. Thus, this does not exclude that inhaled steroids may still be preferred in mild persistent disease, a group of subjects that was not specifically investigated in this meta-analysis, as was the case in the OPTIMA study (O’Byrne et al. 2001).
Furthermore, it would be of interest to know whether those individuals with longstanding asthma have a more neutrophilic or mast cell type of asthma, for which LABA might have additional benefits (Maneechotesuwan et al. 2005; Reid et al. 2003), and inhaled steroids do work less effectively (Green et al. 2002a). Thus, future studies have to investigate whether sputum measures of inflammation may better help to distinguish which patients need combined treatment, especially since a treatment with ICS aiming at the control of sputum eosinophilia and symptoms was better at improving asthma control than the usual care according to symptomatic treatment (Green et al. 2002b), though it is fair to mention that this was not tested with the combination of formoterol/budesonide as the SMART approach but with ICS and additional increase or reduction in ICS or LABA treatment. This might have a benefit since the same authors have shown that patients with asthma and sputum eosinophilia respond better to low-dose inhaled ICS in hyperresponsiveness and quality of life than non-eosinophilic asthma (Berry et al. 2007).
Formoterol/budesonide SMART and salmeterol/fluticasone maintenance
There have been only four double-blind studies (Bousquet et al. 2007; FitzGerald et al. 2005; Kuna et al. 2007; Price et al. 2007) and some open studies (Aalbers et al. 2004; Vogelmeier et al. 2005) that formally have compared the SMART approach with formoterol/budesonide with the maintenance approach with salmeterol/fluticasone.
However, they are difficult to judge, since some studies did not adjust dosing according to symptoms as needed by the patient but were driven by an approach based on the GOAL study (FitzGerald et al. 2005; Price et al. 2007). Thus step-up and step-down management was performed based on a composite score. As shown above in this overview, this may have effects on the outcome of the study. One study had a different dose of inhaled steroid used, i.e. 200 budesonide and 6 μg formoterol bid and additional doses for adjustable maintenance dosing and 500 μg fluticasone and 25 μg salmeterol for maintenance dosing (Bousquet et al. 2007). In that study, treatment with the SMART approach had a better outcome for number of exacerbations, without a difference in lung function, with a mean lower dose of ICS used in the budesonide/formoterol arm (792 versus 1,000 μg/day). However, it may well be that the patient in the salmeterol/fluticasone group would have needed less ICS. Thus, one cannot simply compare these regimens with each other.
The other study (Kuna et al. 2007) compared the 200/6- (SMART approach) with the 400/18-μg b.i.d. (fixed) treatment of budesonide/formoterol and with 125/25 μg fluticasone/salmeterol b.i.d. All treatments provided similar marked improvements in lung function, asthma-controlled days and quality of life. Budesonide/formoterol as the SMART approach reduced asthma exacerbation rates and maintained similar daily asthma control yet at a lower overall drug load compared with the fixed-dose salmeterol/fluticasone and budesonide formoterol. This suggests that indeed adjustable dosing in addition to maintenance treatment is favourable.
We have to await a study investigating the optimisation of treatment and reduction with salmeterol/fluticasone in comparison to the SMART approach with formoterol/budesonide to draw a definite conclusion. For the time being, one should just realise that both treatments are optional and have to be adjusted to the patients need, as long as no exacerbations occur and good control of asthma is present.
Conclusions
In the recent years, considerable insight has been gained in to the optimal management of adult asthma. Most patients with asthma have mild intermittent and persistent disease. Those with mild persistent asthma are usually not well controlled without ICS. Studies have provided firm evidence that these patients can be well controlled when receiving ICS, especially when disease is of recent onset. This treatment should be given on a daily basis at a low dose and when providing a good response should be maintained to prevent severe exacerbations and disease deterioration. Intermittent ICS treatment at the time of an exacerbation has also been suggested as a strategy for mild persistent asthma, but it is less effective than low-dose regular treatment for most outcomes. Adding a LABA to ICS appears to be unnecessary in most of these patients for optimising control of their asthma.
Patients with moderate persistent asthma can be regarded as those who are not ideally controlled on low-dose ICS. The combination of an ICS and LABA is preferred in these patients, irrespective of the brand of medicine, and this combination is better than doubling the dose of ICS to achieve better asthma control and reduce exacerbation risks. One of the combinations available to treat asthma (budesonide and formoterol) has also been assessed as both maintenance and rescue therapy with a further reduction in the risk for a severe exacerbation. Clinical effectiveness in the real world now has to be established, since this approach likely improves compliance with regular maintenance therapy.
Other strategies that have been shown successful are the monitoring of eosinophils in the sputum and the level of hyperresponsiveness, but these options are beyond the scope of this article, as are the treatment with leukotriene antagonists (though less effective than LABA/ICS) and other immuno-modulating agents. It goes without saying that pharmacotherapy should always be accompanied by advice of smoking cessation given the negative effects on response to inhaled steroids, next to other negative health effects. Furthermore, education about the disease and use of inhalers and allergen avoidance and a written management plan are part of an optimal treatment strategy for asthma patients.
References
Aalbers R, Backer V, Kava TT, Omenaas ER, Sandström T, Jorup C, Welte T (2004) Adjustable maintenance dosing with budesonide/formoterol compared with fixed-dose salmeterol/fluticasone in moderate to severe asthma. Curr Med Res Opin 20(2):225–240
Adams NP, Jones PW (2006) The dose–response characteristics of inhaled corticosteroids when used to treat asthma: an overview of Cochrane systematic reviews. Respiratory Med 200:1297–1306
Barnes PJ (1996) Pathophysiology of asthma. Br J Clin Pharmacol 42:3–10
Barnes PJ (2001) Molecular mechanisms of corticosteroids in allergic diseases. Allergy 56:928–936
Barnes PJ (2006) Corticosteroids: the drugs to beat. Eur J Pharmacol 533:2–14
Bateman ED, Boushey HA, Bousquet J, Busse WW, Clark TJ, Pauwels RA, Pedersen SE, GOAL Investigators Group (2004) Can guideline-defined asthma control be achieved? The gaining optimal asthma control study. Am J Respir Crit Care Med 170:836–844
Bateman ED, Jacques L, Goldfrad C, Atienza T, Mihaescu T, Duggan M (2006) Asthma control can be maintained when fluticasone proprionate/salmeterol in a single inhaler is stepped down. J Allergy Clin Immunol 117:563–570
Bateman ED, Clark TJ, Firth L, Bousquet J, Busse WW, Pederen SE (2007) Rate of response of individual asthma control measures varies and may overestimate asthma control: analysis of the GOAL study. J Asthma 44:667–673
Berry M, Morgan A, Shaw DE, Parker D, Green R, Brightling C, Bradding P, Wardlaw AJ, Pavord ID (2007) Pathological features and inhaled corticosteroid response of eosinophilic and non-eosinophilic asthma. Thorax 62(12):1043–1049
Boushey HA, Sorkness CA, King TS, Sullivan SD, Fahy JV, Lazarus SC, Chinchilli VM, Craig TJ, Dimango EA, Deykin A, Fagan JK, Fish JE, Ford JG, Kraft M, Lemanske RF Jr, Leone FT, Martin RJ, Mauger EA, Pesola GR, Peters SP, Rollings NJ, Szefler SJ, Wechsler ME, Israel E, National Heart, Lung, and Blood Institute’s Asthma Clinical Resarch Network (2005) Daily versus as-needed corticosteroids for mild persistent asthma. N Engl J Med 352:1519–1528
Bousquet J, Boulet LP, Peters MJ, Magnussen H, Quiralte J, Martinez-Aguilar NE, Carlsheimer A (2007) Budesonide/formoterol for maintenance and relief in uncontrolled asthma vs. high-dose salmeterol/fluticasone. Respir Med 101(12):2437–2446
Castle W, Fuller R, Hall J, Palmer J (1993) Serevent nationwide surveillance study: comparison of salmeterol with salbutamol in asthmatic patients who require regular bronchodilator treatment. BMJ 306:1034–1037
Douma WR, Kerstjens HA, de Gooijer A, Overbeek SE, Koëter GH, Postma DS (2002) Dutch Chrionic Nonspecific Lung Disease Study Group. Initial improvements in lung function and bronchial hyperresponsiveness are maintained during 5 years of treatment with inhaled beclomethasone dipropionate and terbutaline. Chest 121:151–157
Dijkstra A, Vonk JM, Jongepier H, Koppelman GH, Schouten JP, ten Hacken NH, Timens W, Postma DS (2006) Lung function decline in asthma: association with inhaled corticosteroids, smoking and sex. Thorax 61:105–110
Ernst P, Franssen E, Chan CKN, Okell M, O’Byrne P, Bai T (2008) Predictors of a more favourable response to combined therapy with salmeterol and fluticasone as initial maintenance therapy in asthma. Respir Med 102:77–81
FitzGerald JM, Sears MR, Boulet LP, Becker AB, McIvor AR, Ernst P, Smiljanic-Georgijev NM, Lee JS, Canadian Investigators (2003) Adjustable maintenance dosing with budesonide/formoterol reduces asthma exacerbations compared with traditional fixed dosing: a five-month multicentre Canadian study. Can Respir J 10(8):427–434
FitzGerald JM, Boulet LP, Follows RM (2005) The CONCEPT trial: a 1-year, multicenter, randomized,double-blind, double-dummy comparison of a stable dosing regimen of salmeterol/fluticasone propionate with an adjustable maintenance dosing regimen of formoterol/budesonide in adults with persistent asthma. Clin Ther 27(4):393–406
Fujimoto K, Yamaguchi S, Urushibata K, Hanaoka M, Koizumi T, Honda T, Kubo K (2006) Characteristics of asthma resistant to moderate dose inhaled corticosteroid treatment on bronchial hyperresponsiveness. Intern Med 45(14):843–849
Gibson PG, Powell H, Ducharme FM (2007) Differential effects of maintenance long-acting beta-agonist and inhaled corticosteroid on asthma control and asthma exacerbations. J Allergy Clin Immunol 119(2):344–350
Global Initiative for Asthma (2004) Global strategy for asthma management and prevention. NIH publication no. 02-3659. National Institutes of Health, Bethesda, MD
Green RH, Brightling CE, Woltmann G, Parker D, Wardlaw AJ, Pavord ID (2002a) Analysis of induced sputum in adults with asthma: identification of subgroup with isolated sputum neutrophilia and poor response to inhaled corticosteroids. Thorax 57:875–879
Green RH, Brightling CE, McKenna S, Hargadon B, Parker D, Bradding P, Wardlaw AJ, Pavord ID (2002b) Asthma exacerbations and sputum eosinophil counts: a randomised controlled trial. Lancet 360(9347):1715–1721
Green RH, Brightling CE, McKenna S, Hargadon B, Neale N, Parker D, Ruse C, Hall IP, Pavord ID (2006) Comparison of asthma treatment given in addition to inhaled corticosteroids on airway inflammation and responsiveness. Eur Respir J 27:1144–1151
Greening AP, Ind PW, Northfield M, Shaw G (1994) Added salmeterol versus higher-dose corticosteroid in asthma patients with symptoms on existing inhaled corticosteroid. Allen & Hanburys Limited UK Study Group. Lancet 344:219–224
Ind PW, Haughney J, Price D, Rosen JP, Kennelly J (2004) Adjustable and fixed dosing with budesonide/formoterol via a single inhaler in asthma patients: the ASSURE study. Respir Med 98(5):464–475
Kerstjens HA, Brand PL, Hughes MD, Robinson NJ, Postma DS, Sluiter HJ, Bleecker ER, Dekhuijzen PN, de Jong PM, Mengelers HJ (1992) A comparison of bronchodilator therapy with or without inhaled corticosteroid therapy for obstructive airways disease. Dutch Chronic Non-Specific Lung Disease Study Group. N Engl J Med 327:1413–1419
Kerstjens HA, Overbeek SE, Schouten JP, Brand PL, Postma DS (1993) Airways hyperresponsiveness, bronchodilator response, allergy and smoking predict improvement in FEV1 during long-term inhaled corticosteroid treatment. Dutch CNSLD Study Group. Eur Respir J 6:868–876
Kerstjens HA, Schouten JP, Brand PL, Schoonbrood DF, Sterk PJ, Postma DS (1995) Importance of total serum IgE for improvement in airways hyperresponsiveness with inhaled corticosteroids in asthma and chronic obstructive pulmonary disease. The Dutch CNSLD Study Group. Am J Respir Crit Care Med 151:360–368
Kips JC, O’Connor BJ, Inman MD, Svensson K, Pauwels RA, O’Byrne PM (2000) A long-term study of the antiinflammatory effect of low-dose budesonide plus formoterol versus high-dose budesonide in asthma. Am J Respir Crit Care Med 161:996–1001
Koopmans JG, Lutter R, Jensen HM, van der Zee JS (2006) Adding salmeterol to an inhaled corticosteroid reduces allergen-induced serum IL-5 and peripheral blood eosinophils. J Allergy Clin Immunol 116:1007–1013
Kuna P, Peters MJ, Manjra AI, Jorup C, Naya IP, Martínez-Jimenez NE, Buhl R (2007) Effect of budesonide/formoterol maintenance and reliever therapy on asthma exacerbations. Int J Clin Pract 61(5):725–736
Lange P, Parner J, Vestbo J, Schnohr P, Jensen G (1998) A 15-year follow-up study of ventilatory function in adults with asthma. N Engl J Med 339:1194–200
Lazarus SC, Boushey HA, Fahy JV, Chinchilli VM, Lemanske RF Jr, Sorkness CA, Kraft M, Fish JE, Peters SP, Craig T, Drazen JM, Ford JG, Israel E, Martin RJ, Mauger EA, Nachman SA, Spahn JD, Szefler SJ, Asthma Clinical Research Network for the National Heart, Lung, and Blood Institute (2001) Long-acting beta2-agonist monotherapy vs. continued therapy with inhaled corticosteroids in patients with persistent asthma. JAMA 285:2583–2593
Lemiere C, Bai T, Balter M, Bayliff C, Becker A, Boulet LP, Bowie D, Cartier A, Cave A, Chapman K, Cowie R, Coyle S, Cockcroft D, Ducharme FM, Ernst P, Finlayson S, FitzGerald JM, Hargreave FE, Hogg D, Kaplan A, Kim H, Kelm C, O’Byrne P, Sears M, Markham AW (2004) Adult asthma consensus guidelines update 2003. Can Respir J 11:9A–18A
Li X, Ward C, Thien F, Bish R, Bamford T, Bao X, Bailey M, Wilson JW, Haydn Walters E (1999) An anti-inflammatory effect of salmeterol, a long-acting beta2 agonist, assessed in airway biopsies and bronchoalveolar lavage in asthma. Am J Respir Crit Care med 160:1493–1499
Lundborg M, Wille S, Bjermer L, Tilling B, Lundgren M, Telg G, Ekström T, Selroos O (2006) Maintenance plus reliever budesonide/formoterol compared with a higher maintenance dose of budesonide/formoterol plus formoterol as reliever in asthma: an efficacy and cost-effectiveness study. Curr Med Res Opin 22:809–821
Maneechotesuwan K, Essifie-Quaye S, Meah S, Kelly C, Kharitonov SA, Adcock IM, Barnes PJ (2005) Formoterol attenuates neutrophilic airway inflammation in asthma. Chest 128:1378–1385
Martin RJ, Szefler SJ, King TS, Kraft M, Boushey HA, Chinchilli VM, Craig TJ, Dimango EA, Deykin A, Fahy JV, Israel E, Lazarus SC, Lemanske RF Jr, Leone FT, Pesola GR, Peters SP, Sorkness CA, Szwejbka LA, Wechsler ME, the National Heart, Lung, and Blood Institute’s Asthma Clinical Research Center (2007) The predicting response to inhaled corticosteroid efficacy (PRICE) trial. J Allergy Clin Immunol 119:73–80
Masoli M, Fabian D, Holt S, Beasley R (2005) The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy 59:469–478
Miller-Larsson A, Selroos O (2006) Advances in asthma and COPD treatment: combination therapy with inhaled corticosteroids and long-acting beta 2-agonists. Curr Pharm Des 12(25):3261–3279
Nelson HS (2006) Long-acting beta-agonists in adult asthma: evidence that these drugs are safe. Prim Care Respir J 15:271–277
Nelson HS, Busse WM, Kerwin E, Church N, Emmet A, Rickhard K, Knobil K (2000) Fluticasone propionate/salmeterol combination provides more effective asthma control than low-dose inhaled corticosteroid plus montelukast. J Allergy Clin Immunol 106:1088–1095
Nelson HS, Chapman KR, Pyke SD, Johnson M, Pritchard JN (2003) Enhanced synergy between fluticasone propionate and salmeterol inhaled from a single inhaler versus separate inhalers. J Allergy Clin Immunol 112(1):29–36
Nelson HS, Weiss ST, Bleecker ER, Yancey SW, Dorinsky PM, the SMART Study Group (2006) The salmeterol multicenter asthma research trial. Chest 129:15–26
NHLBI (2002) Global initiative for asthma. Global strategy for asthma management and prevention. NHLBI, Bethesda, MD
O’Byrne PM, Parameswaran K (2006) Pharmacological management of mild or moderate persistent asthma. Lancet 368:794–803
O’Byrne PM, Barnes PJ, Rodriguez-Roisin R, Runnerstrom E, Sandstrom T, Svensson K, Tattersfield A (2001) Low dose inhaled budesonide and formoterol in mild persistent asthma: the OPTIMA randomized trial. Am J Respir Crit Care Med 164:1392–1397
O’Byrne PM, Bisgaard H, Godard PP, Godard PP, Pistolesi M, Palmqvist M, Zhu Y, Ekstrom T, Bateman ED (2005) Budesonide/formoterol combination therapy as both maintenance and reliever medication in asthma. Am J Respir Crit Care Med 171:129–136
Oppenheimer H, Nelson HS (2008) Safety of long-acting beta-agonists in asthma: a review. Curr Opin Pulm Med 14:64–60
Panettieri RA (2004) Effects of corticosteroids on structural cells in asthma and chronic obstructive pulmonary disease. Proc Am Thorac Soc 1:231–234
Pauwels RA, Lofdahl CG, Postma DS, Tattersfield AE, O’Byrne P, Barnes PJ, Ullman A (1998) Effect of inhaled formoterol and budesonide on exacerbations of asthma. Formoterol and corticosteroids establishing therapy (FACET). N Engl J Med 337:1405–1411
Pauwels RA, Pedersen S, Busse WW, Tan WC, Cheny Z, Ohlsson SV, Ullman A, Lamm CJ, O’Byrne PM, START Investigators Group (2003) Early intervention with budesonide in mild persistent asthma: a randomised, double-blind trial. Lancet 361:1071–1076
Pedersen SE, Bateman ED, Bousquet J, Busse WW, Yoxalls, Clark TJ, Gaining Optimal Asthma Control Steering Committee and Investigators (2007) Determinants of response to fluticasone propionate and salmeterol/fluticasone proprionate combination in the Gaining Optimal Asthma controL study. J Allergy Clin Immunol 120:1036–1042
Pohl WR, Vetter N, Zwick H, Hrubos W (2006) Adjustable maintenance dosing with budesonide/formoterol or budesonide: double-blind study. Respir Med 100(3):551–60
Price DB, Williams AE, Yoxall S (2007) Salmeterol/fluticasone stable-dose treatment compared with formoterol/budesonide adjustable maintenance dosing: impact on health-related quality of life. Repir Res 8:46
Rabe KF, Pizzichini E, Stallberg B, Romero S, Balanzat AM, Atienza T, Lier PA, Jorup C (2006a) Budesonide/formoterol in a single inhaler for maintenance and relief in mild-to-moderate asthma: a randomized, double-blind trial. Chest 129:246–256
Rabe KF, Atienza T, Magyar P, Larsson P, Jorup C, Lallooo UG (2006b) Effect of budesonide in combination with formoterol for reliever therapy in asthma exacerbations: a randomised controlled, double-blind study. Lancet 368:744–753
Reid DW, Ward C, Wang N, Zheng L, Bish R, Orsida B, Walters EH (2003) Possible anti-inflammatory effect of salmeterol against interleukin-8 and neutrophil activation in asthma in vivo. Eur Respir J 21:994–999
Ringdal N, Derom E, Wahlin-Boll E, Pauwels R (1998) Onset and duration of action of single doses of formoterol inhaled via turbuhaler. Respit Med 92:1017–1021
Ringdal N, Eliraz A, Pruzinec R, Weber HH, Mulder PG, Akveld M, Bateman ED, International Study Group (2003) The salmeterol/fluticasone combination is more effective than fluticasone plus oral montelukast tin asthma. Respir Med 97:234–241
Salpeter SR, Buckley NS, Ormiston TM, Salpeter EE (2006) Meta-analysis: effect of long-acting beta-agonists on severe asthma exacerbations and asthma-related deaths. Ann Intern Med 144:904–912
Scicchitano R, Aalbers R, Ukena D, Manjra A, Fouquert L, Centanni S, Boulet LP, Naya IP, Hultquist C (2004) Efficacy and safety of budesonide/formoterol single inhaler therapy versus a higher dose of budesonide in moderate to severe asthma. Curr Med Res Opin 20:1403–1418
Shrewsbury S, Pyke S, Britton M (2000) Meta-analysis of increased dose of inhaled steroid or addition of salmeterol in symptomatic asthma (MIASMA). BMJ 320:1368–1373
Tattersfield AE, Postma DS, Barnes PJ, Svensson K, Bauer CA, O’Byrne PM, Löfdahl CG, Pauwels RA, Ullman A (1999) Exacerbations of asthma: a descriptive study of 425 severe exacerbations. The FACET International Study Group. Am J Respir Crit Care Med 160(2):594–599
ten Hacken NH, Timens W, Smith M, Drok G, Kraan J, Postma DS (1998) Increased peak expiratory flow variation in asthma: severe persistent increase but not nocturnal worsening of airway inflammation. Eur Respir J 12(3):546–550
van der Molen T, Meyboom-de Jong B, Mulder HH, Postma DS (1998) Starting with a higher dose of inhaled corticosteroids in primary care asthma treatment. Am J Respir Crit Care Med 158(1):121–125
Vogelmeier C, D’Urzo A, Pauwels R, Merino JM, Jaspal M, Boutet S, Naya I, Price D (2005) Budesonide/formoterol maintenance and reliever therapy: an effective asthma treatment option? Eur Respir J 26:819–828
Wallin A, Sue-Chu M, Bjermer I, Ward J, Sandstrom T, Lindberg A, Lundbäck B, Djukanovic R, Holgate S, Wilson S (2003) Effect of inhaled fluticasone with and without salmeterol on airway inflammation in asthma. J Allergy Clin Immunol 112:72–78
Woodcock AA, Gabdonas A, Boonsawat W, Gibbs MR, Bousquet J, Bateman ED (2007) Improvement in asthma endpoints when aiming for total control: salmeterol/fluticasone proprionate versus fluticasone proprionate alone. Prim Care Resp J 16:155–161
Zetterström O, Buhl R, Mellem H, Perpiñá M, Hedman J, O’Neill S, Ekström T (2001) Improved asthma control with budesonide/formoterol in a single inhaler, compared with budesonide alone. Eur Respir J 18:262–268
Giembycz MA, Kaur M, Leigh R, Newton R (2008) A holy grail of asthma management: toward understanding how long-acting β2-adrenoceptor agonists enhance the clinical efficacy of inhaled corticosteroids. Br J Pharmacol 153:1090–1104
Postma DS, Kerstjens HAM, ten Hacken NHT (2008) Inhaled corticosteroids and long-acting beta-agonists in adult asthma: a winning combination in all? Naunyn-Schmiedeberg’s Arch Pharmacol 378:203–215
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
The author wishes to dedicate this manuscript to Prof. J. Zaagsma.
It has come to the attention of the journal, that a review article published last year (Postma et al. 2008) contains several passages which are identical to text published by other authors (Giembycz et al. 2008) without giving reference to the original source of these text blocks. The journal has come to the conclusion that this constitutes plagiarism and hence has decided to retract the paper.
An erratum to this article can be found at http://dx.doi.org/10.1007/s00210-009-0418-8
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Postma, D.S., Kerstjens, H.A.M. & ten Hacken, N.H.T. RETRACTED ARTICLE: Inhaled corticosteroids and long-acting beta-agonists in adult asthma: a winning combination in all?. Naunyn-Schmied Arch Pharmacol 378, 203–215 (2008). https://doi.org/10.1007/s00210-008-0302-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00210-008-0302-y